
Regular physical activity is one of the most important things people can do to improve their health according to the national physical activity guidelines. Exercise is associated with the reduction in risk of many adverse conditions, including the four horsemen of chronic disease: metabolic dysregulation, cardiovascular disease, cancer, and neurodegeneration. (Metabolic dysregulation has many faces, including type 2 diabetes, systemic insulin resistance, metabolic syndrome, and non-alcoholic fatty liver disease.) Exercise is also associated with a lower risk of chronic lung disease, as well as with a lower risk of frailty and the debilitating or deadly falls and injuries that accompany it. In other words, exercise is associated with a lower risk of the conditions that kill the majority of US adults over the age of 40. Exercise might be the most potent “drug” we have for extending the quality and perhaps quantity of our years of life.
But the benefits of exercise on mortality have never been assessed in the setting of a randomized controlled trial (RCT), which can help us determine if there’s a cause-and-effect relationship. Is exercise a marker or a maker of improved health? Are all types of exercise created equal when it comes to longevity? Until recently, these questions had not been addressed in an RCT. Enter the Generation 100 study, the results of which were published in October of 2020 in the BMJ: “Effect of exercise training for five years on all cause mortality in older adults—the Generation 100 study: randomised controlled trial.”
Want more content like this? Check out our episode on the importance of muscle mass, strength, and cardiorespiratory fitness for longevity and our article on metformin and exercise.
About the Generation 100 Study
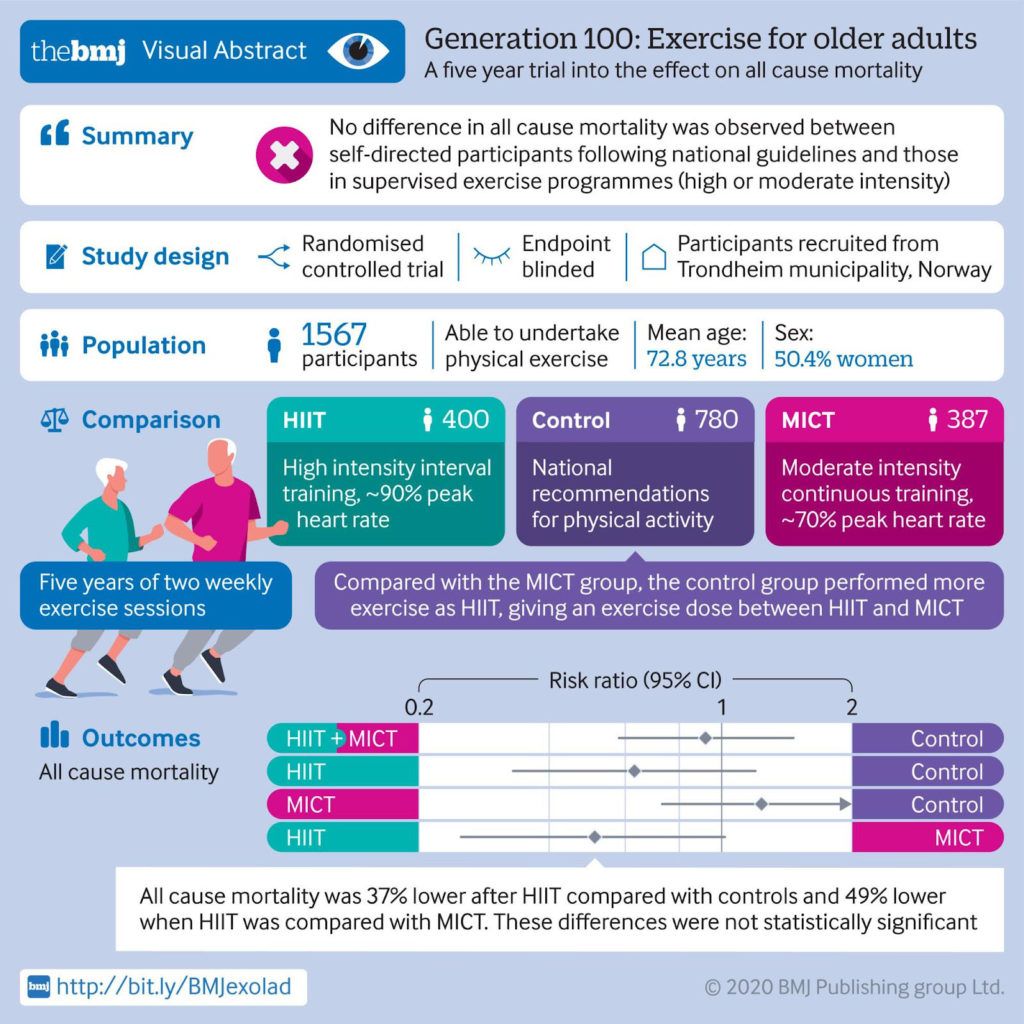
Researchers from Norway conducted a five-year study to test the effect of exercise and mortality in adults in their seventies living in the city of Trondheim. More than 1,500 participants in this study were randomized into one of three groups: a control group, high-intensity interval training (HIIT), or moderate-intensity continuous training (MICT).
About half of the participants were assigned to the control group and were asked to follow the Norwegian physical activity guidelines for 2012, which recommends 30 minutes of moderate-level physical activity almost every day. The recommendations tell adults—including the elderly—to engage in at least 150 minutes of moderate-intensity physical activity throughout the week, or engage in at least 75 minutes of vigorous-intensity physical activity throughout the week, or engage in an equivalent combination of moderate- and vigorous-intensity activity.
The other half of participants were assigned to the HIIT or MICT groups. Participants in the HIIT group were asked to exchange two of the five 30-minute moderate-intensity physical activity sessions each week (as recommended by Norwegian health authorities) with two “4-by-4” HIIT sessions, consisting of a 10-minute warm-up followed by four four-minute intervals at approximately 90% peak heart rate with three minutes of active recovery (about 60% of peak heart rate) in between. Participants in the MICT group were asked to exchange two of the five guideline-recommended 30-minute moderate-intensity physical activity sessions each week with two MICT sessions, consisting of 50 minutes of continuous work at about 70% of peak heart rate.
All participants were asked to follow their respective protocols for five years. Every sixth week, both the HIIT and MICT groups met separately for supervised spinning sessions with an exercise physiologist, wearing heart rate monitors to ensure the recommended heart rates were achieved. Supervised training with exercise physiologists present was also offered twice per week in different outdoor areas over the course of the study. For the control group, no supervision was provided.
After five years, just under 5% of the participants assigned to the control group had died, while the mortality rates in participants assigned to the HIIT and MICT groups were about 3% and 6%, respectively. The combined mortality rate of the HIIT and MICT participants was 4.5%.
The investigators concluded that combined MICT and HIIT has no effect on all-cause mortality compared with recommended physical activity levels, but they did observe a lower all-cause mortality trend in the participants assigned to HIIT compared with those assigned to MICT and controls. All-cause mortality was nearly 40% lower in participants assigned to HIIT compared with controls, and about 50% lower when HIIT was compared with MICT, but these differences were not statistically significant. The New York Times reported on the trial with the following headline: “The Secret to Longevity? 4-Minute Bursts of Intense Exercise May Help.” A visual abstract of the study is provided in the Figure below, courtesy of the BMJ.
Figure. Visual abstract of the Generation 100 study.
Understanding the Results of the Generations 100 Study
Given the results, should we conclude that exercise has no effect on all-cause mortality? Recall that participants in the control group were asked to follow the Norwegian physical activity guidelines, which recommends 30 minutes of moderate-level physical activity almost every day. Again, the Norwegian guidelines, which are almost a carbon copy of the US guidelines, recommend that all adults — including the elderly — engage in at least 150 minutes of moderate-intensity physical activity throughout the week, or engage in at least 75 minutes of vigorous-intensity physical activity throughout the week, or engage in an equivalent combination of moderate- and vigorous-intensity activity. The recommendations also add that the amount of daily activity needed to avoid weight gain is about 60 minutes of moderate-intensity activity or a somewhat shorter duration of vigorous-intensity activity.
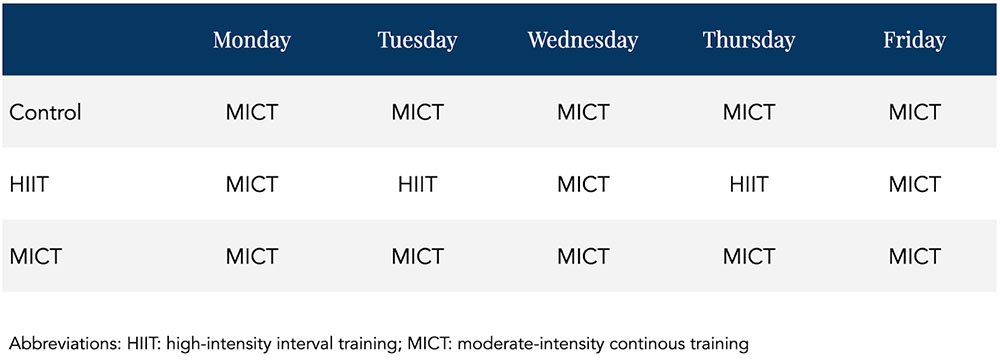
Also recall that the control group was compared to a HIIT and MICT group, which were essentially asked to follow the same recommendations as the control group three days out of the week. HIIT and MICT groups only differed from controls in that they were asked to exchange two of the 30-minute moderate-intensity physical activity sessions each week with two days of HIIT and MICT sessions, respectively. The control group was essentially asked to do five half-hour MICT sessions per week. The MICT group was asked to do five MICT sessions per week with three sessions lasting 30 minutes and two sessions lasting 20 minutes longer. The HIIT group was asked to do three 30-minute MICT sessions per week and two HIIT sessions per week.
How different is the control group from the MICT group? Not much. In fact, looking at the Table below showing possible weekly schedules for each group, the control and MICT groups would seem completely identical.
Table. Theoretical weekly exercise schedule for the three arms of the study.
Limitations of Randomized Control Trials (RCTs)
Essentially, the study compared people asked to exercise regularly with people asked to exercise regularly with occasional supervision. Here was an opportunity to “find out if exercise directly affects lifespans,” as the Times put it, and yet the investigators designed a control group that wasn’t suitable to find this out. With virtually no difference in the variable of interest between control and experimental groups, statistically significant differences in results would be highly unlikely even if a true association were present.
Why didn’t the investigators ask participants in the control group to be sedentary in order to test the effect of exercise on mortality? According to the Times, the investigators felt that it would be unethical. Do you see the dilemma? In order to conduct a proper RCT to find out if exercise has an effect on mortality, researchers need a control group that is asked not to exercise. If they think that’s unethical, it means they’re already convinced that exercise directly affects lifespans.
The investigators acknowledged the high level of physical activity in the control group, “which probably reduced the study’s ability to detect statistically significant effects of exercise training on primary outcomes.” They suggested that “New concepts or study designs are needed to avoid the Hawthorne effect in future studies.” The Hawthorne effect refers to the alteration of behavior by the participants of a study due to their awareness of being observed. Without getting into obvious reasons why there was such a high level of adherence in this study independent of the Hawthorne effect, this brings up another dilemma. The researchers suggest the use of new study designs for further investigation, presumably designs in which the control group is less active than they were in this published study. But if these investigators, who believe that asking people to be sedentary is unethical, came up with a new concept or study design intended to make the control group more sedentary than the intervention groups, wouldn’t they still encounter the same ethical concerns? It’s difficult to reconcile the fact that one of the supposed problems with this study is that the control group followed their assignment too well.
The bottom line is that the control group is completely inappropriate from the standpoint of trying to determine cause and effect in this study. Instead, the best the investigators could do based on their design is to test whether asking people to exercise with occasional supervision lowers mortality compared with asking people to exercise with no supervision. I think that’s a shame. But the goal of establishing rigorous scientific evidence for well-known health principles does not justify willfully causing harm (or withholding help) to a group of people. No RCT is necessary to prove, for instance, that having crude arsenic for breakfast increases mortality relative to eating eggs and toast, and to run such a study would constitute mass murder, not science.
The looming question is: where do we draw the line? Are we already so confident that exercise directly affects lifespans that this question should be similarly exempt from a randomized controlled clinical trial? And how do we gain further reliable insight into such “forbidden” research questions? Most likely, a combination of approaches is needed. We might find some utility in certain observational data, as well as in cellular mechanistic studies. Further, randomized study designs can often be applied to address topics highly relevant to the research question – for instance, one might test effects of shorter-term exercise patterns on molecular markers associated with chronic disease risk.
On the question of exercise and longevity, various alternative investigation approaches each might provide only a small piece of the puzzle. But together, they’d likely stand a better chance of answering this question than a single study designed with an inadequate control group and practically no chance of detecting a true underlying effect.
– Peter
The essence of maintaining proper health in a nutshell…
One must keep on moving for better and longer life.
Confirmed by personal experience. At age 79 I am still fully prescription drug free and totally independent. My only exercise are long-distance hiking, gardening, using stairs many times daily and doing my own shopping, lifting and toting of groceries etc. I even have my coffee pot and daily essentials on the top shelf which requires tip-toes and full reach for a short person like me. My prescription for longevity is opt for physical inconvenience and challenges in your daily life as I simply don’t enjoy group activities or exercise equipment. Not scientific at all but seems to work for me.
The Times headline is typical. “Journalism” today is focused more on clicks than substance. The victims are the people without time or energy to seek out the real answers, most of America. We see similar misleading articles on various diets leaving a gaping need for the type of content and perspective you give.
The Generation 100 study, with it’s lack of a true control is an admission of what we all know. Exercise does extend life versus the average, sedentary lifestyle. I have only to look at myself versus my parents for the empirical evidence. The phrase “move it or lose it” rings true.
What about the study being underpowered? If you have a 50% reduction in mortality rate and this is not statistically significant, doesn’t this simply mean that the sample size is too small or that there aren’t sufficient participants that meet the primary endpoint?
I agree, Jaap. If your intervention makes a 50% difference but it is not statistically significant, then the problem is not that your intervention is not effective enough. The problem is that your study is underpowered.
It is surprising to me, though, that the overall mortality rate was only 5% over 5 years, given that the average age at the start of the study was 73 years old. Looking at mortality tables, I would have expected the 5-year mortality rate to be closer to 15%.
As i can tell, it’s not new that HIIT is the best there is. The question is how many days a week. Looks to me like two days is fine. And combination with light activities
Peter, wouldn’t it had been possible to tell the control group nothing at all, and do a yearly or monthly self reported assessment on their lifestyle from which you could derive directly or indirectly their physical activity? And then use as final control group only those who did not excercise?
Love your work, your knowledge and content.
Your description of the HIIT protocol did not show that after the ten minute warm-up there are four intervals, each of 1 minute at greater than 90%, followed by a 3 minute recovery. Your description implied that there were four intervals of 4 minutes each, followed by a 3 minute recovery period. Crikey!
Thank you for the correction, Alan.
I read the protocol described here and was like…?!?! 4 minutes at 90% ?!?!
I can maintain 90% for a few seconds, but certainly never 4 minutes. Even one full minute at 90% sounds hellish to me.
Isn’t VO2Max was a known marker of reduced all cause mortality and enough to show a link between exercise and longevity?
Blue zoners don’t- to my knowledge- engage in HIIT . But they move a lot. They are alive and thriving in today’s world- with all of its challenges and benefits. HIIT is amazing, and study-able, but it’s not the only game in town.
The idea of Blue Zones may be based on poor science.
https://sciencebasedmedicine.org/blue-zones-diet-speculation-based-on-misinformation/
The elephant in the room though remains the fact that there is no data relating to what all parties ate, nor what they ate over the previous 40 odd years. As is well known by now (almost to a boring degree) dietry lifestyle has a huge outcome on mortality in the aged, so yes, somewhat of a waste of time and money.
Dr. Attia
Thanks this is interesting. How about studying the population of say, Apple Watch wearers over five years? Ask for permission to participate in the study when setting up the new watch, then observe as movement data naturally divides itself into quadrants over several years and follow up with participants. Everybody has good intentions when they first make the purchase, but actual habits will play out over the long term and possibly provide some useable data.
It is indeed unfortunate that the design of this lengthy study made it pretty much inconclusive. The ethical issue could be avoided by simply giving no instruction to the control group so they continue with their regular habits which would mean for a lot of them a mostly sedentary lifestyle. Then equip all of them with a fitness tracker and assess actual physical activity and heart rate performance via the logged data and compare it to health developments and morbidity in each group. Am I missing something here Thanks. Ortwin
This would have been simple, and a much better design. I wish you had been on the study design team.
To me the key question is: did the control group follow the recommendations. If they did, then the study is not really doing what it says it does. On the other hand, if the control group didn’t exercise (which is what most people do irrespective of recommendations), then it is interesting. I don’t think we should dismiss the findings out of hand.
Hi Peter,
Do we really need studies on everything? Aren’t some things just fucking obvious? Do we really need oxygen to breathe? – well we’re not exactly sure – so let’s see – we better do a study and make sure. Human beings were constructed to move, work and stay active. Isn’t that why we have arms and legs? We’ve constructed a society to make everything easy and convenient – unhealthy food and no movement. If you eat that food and don’t move – I think it’s safe to conclude that you might run into physical problems. Do we need studies and control groups to conclude that bad food and no movement (or just one of these) decreases quality of life and shortens life span? Can’t people just look around in their own circle and make that conclusion?
Looking at the Norwegian actuarial life tables, about 9% of Norwegian 72-year-olds would have been expected to die during that 5-year period. So here is my crude analysis.
Chance of dying over a 5-year period starting at age 72:
HIIT group 3%
MICT group 6%
All-Population 9%
The All-Population number includes everyone in Norway, exercisers and non-exercisers. Since the exerciser death rate is lower than average (6% or less), the non-exerciser death rate would need to be higher than average (maybe 11% or more), to average out to 9%, depending on the ratio of non-exercisers in the total population.
There are many flaws with my analysis above, but my hypothesis is that HIIT reduces your risk of dying dramatically. Possibly an odds ratio of 3 or greater. I would further hypothesize that a similar relationship holds across all ages, but likely less dramatic the younger you are, since risk of death in general is much lower at younger ages.
Here is another interesting, yet unsurprising, statistic I learned while looking at the life tables. A Norwegian 72-year-old has about a 9% chance of dying within 5-years. A 72-year-old in the USA has about a 12% chance of dying within 5-years.
https://www.ssb.no/en/statbank/table/07902
https://www.ssa.gov/oact/STATS/table4c6.html
Reading this, I wonder about adaptation and aging. Usually, doing the same thing over and over again brings adaptation, which in turn means no more gain. Over a certain age, does this adaptation means more decline? My instinctive approach would be to do something for a while untill I see… what? I guess you can still see gains. If you want to participate in the centanial Olympics, you surely need to vary more than a weekly schedule.
Why not just use a group of willingly sedentary people as the control (which is most of the U.S. population as far as I can tell)?