
I wrote this post at about the same time Germany won the World Cup in Rio de Janeiro in 2014. There’s been a lot of moving and shaking in the world of exogenous ketones since then, not to mention soccer. Looking back on my post, I still consider it relevant in terms of what exogenous ketones possibly can (and cannot) do for performance. In this case, to see if exogenous ketone esters provide me a “boost” by allowing me to do the same amount of work while expending less energy (and work at a relatively lower VO2) compared to no supplementation.
I’m getting an increasing number of questions about exogenous ketones. Are they good? Do they work for performance? Is there a dose-response curve? If I’m fasting, can I consume them without “breaking” the fast? Am I in ketosis if my liver isn’t producing ketones, but my BOHB is 1.5 mmol/L after ingesting ketones? Can they “ramp-up” ketogenesis? Are they a “smart drug?” What happens if someone has high levels of both glucose and ketones? Are some products better than others? Salts vs esters? BHB vs AcAc? Can taking exogenous ketones reduce endogenous production on a ketogenic diet? What’s the difference between racemic mixtures, D-form, and L-form? What’s your experience with MCTs and C8?
Caveat emptor: the following post doesn’t come close to answering most of these questions. I only document my experience with BHB salts (and a non-commercial version at that), but say little to nothing about my experience with BHB esters or AcAc esters. But it will provide you will some context and understanding about what exogenous ketones are, and what they might do for athletic performance. We’ll likely podcast about the questions and topics above and cover other aspects of exogenous ketones in more detail.
—P.A., June 2018
§
Original publication date: August 14, 2014
Last year I wrote a couple of posts on the nuances and complexities of ketosis, with an emphasis on nutritional ketosis (but some discussion of other states of ketosis—starvation ketosis and diabetic ketoacidosis, or DKA). To understand this post, you’ll want to at least be familiar with the ideas in those posts, which can be found here and here.
In the second of these posts I discuss the Delta G implications of the body using ketones (specifically, beta-hydroxybutyrate, or BHB, and acetoacetate, or AcAc) for ATP generation, instead of glucose and free fatty acid (FFA). At the time I wrote that post I was particularly (read: personally) interested in the Delta G arbitrage. Stated simply, per unit of carbon, utilization of BHB offers more ATP for the same amount of oxygen consumption (as corollary, generation of the same amount of ATP requires less oxygen consumption, when compared to glucose or FFA).
I also concluded that post by discussing the possibility of testing this (theoretical) idea in a real person, with the help of exogenous (i.e., synthetic) ketones. I have seen this effect in (unpublished) data in world class athletes not on a ketogenic diet who have supplemented with exogenous ketones (more on that, below). Case after case showed a small, but significant increase in sub-threshold performance (as an example, efforts longer than about 4 minutes all-out).
So I decided to find out for myself if ketones could, indeed, offer up the same amount of usable energy with less oxygen consumption. Some housekeeping issues before getting into it.
- This is a self-experiment, not real “data”—“N of 1” stuff is suggestive, but it prevents the use of nifty little things likes error bars and p-values. Please don’t over interpret these results. My reason for sharing this is to spark a discussion and hope that a more systematic and rigorous approach can be undertaken.
- All of the data I’ll present below were from an experiment I did with the help of Dominic D’Agostino and Pat Jak (who did the indirect calorimetry) in the summer of 2013. (I wrote this up immediately, but I’ve only got around to blogging about it now.) Dom is, far and away, the most knowledgeable person on the topic of exogenous ketones. Others have been at it longer, but none have the vast experiences with all possible modalities (i.e., esters versus salts, BHB versus AcAc) and the concurrent understanding of how nutritional ketosis works. If people call me keto-man (some do, as silly as it sounds), they should call Dom keto-king.
- I have tried the following preparations of exogenous ketones: BHB monoester, AcAc di-ester, BHB mineral salt (BHB combined with Na+, K+, and Ca2+). I have consumed these at different concentrations and in combination with different mixing agents, including MCT oil, pure caprylic acid (C8), branch-chained amino acids, and lemon juice (to lower the pH). I won’t go into the details of each, though, for the sake of time.
- The ketone esters are, hands-down, the worst tasting compounds I have ever put in my body. The world’s worst scotch tastes like spring water compared to these things. The first time I tried 50 mL of BHB monoester, I failed to mix it with anything (Dom warned me, but I was too eager to try them to actually read his instructions). Strategic error. It tasted as I imagine jet fuel would taste. I thought I was going to go blind. I didn’t stop gagging for 10 minutes. (I did this before an early morning bike ride, and I was gagging so loudly in the kitchen that I woke up my wife, who was still sleeping in our bedroom.) The taste of the AcAc di-ester is at least masked by the fact that Dom was able to put it into capsules. But they are still categorically horrible. The salts are definitely better, but despite experimenting with them for months, I was unable to consistently ingest them without experiencing GI side-effects; often I was fine, but enough times I was not, which left me concluding that I still needed to work out the kinks. From my discussions with others using the BHB salts, it seems I have a particularly sensitive GI system.
The hypothesis we sought out to test
A keto-adapted subject (who may already benefit from some Delta G arbitrage) will, under fixed work load, require less oxygen when ingesting exogenous ketones than when not.
Posed as a question: At a given rate of mechanical work, would the addition of exogenous ketones reduce a subject’s oxygen consumption?
The “experiment”
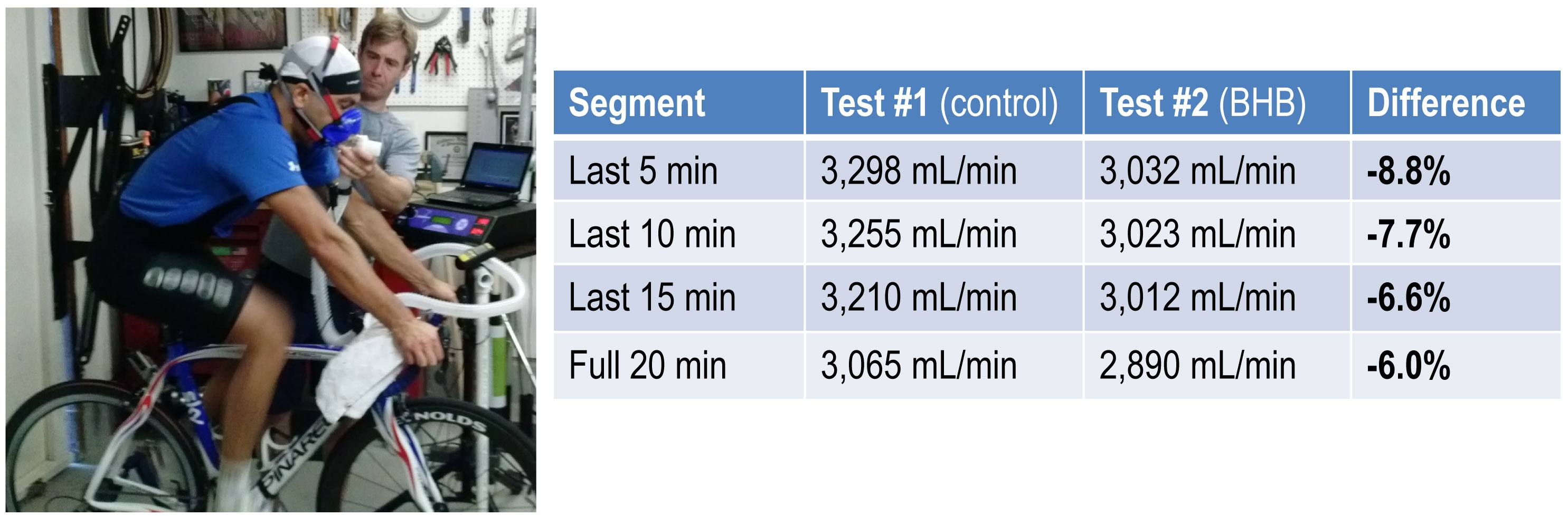
- A keto-adapted subject (me) completed two 20-minute test rides at approximately 60% of VO2 max on a load generator (CompuTrainer); such a device allows one to “fix” the work requirement by fixing the power demand to pedal the bike
- This fixed load was chosen to be 180 watts which resulted in approximately 3 L/min of VO2—minute ventilation of oxygen (this was an aerobic effort at a power output of approximately 60% of functional threshold power, FTP, which also corresponded to a minute ventilation of approximately 60% of VO2 max)
- Test set #1—done under conditions of mild nutritional ketosis, while still fasted
- Test set #2—60 minutes following ingestion of 15.6 g BHB mineral salt to produce instant “artificial ketosis,” which took place immediately following Test set #1
- Measurements taken included whole blood glucose and BHB (every 5 minutes); VO2 and VCO2 (every 15 seconds); HR (continuous); RQ is calculated as the ratio of VO2 and VCO2. In the video of this post I explain what VO2, VCO2, and RQ tell us about energy expenditure and substrate use—very quickly, RQ typically varies between about 0.7 and 1.0—the closer RQ is to 0.7, the more fat is being oxidized; the reverse is true as RQ approaches 1.0

Results
Test set #1 (control—mild nutritional ketosis)
The table below shows the data collected over the first 20 minute effort. The 20 minute effort was continuous, but for the purpose of presenting the data, I’ve shown the segmental values—end of segment for glucose and BHB; segment average for HR, minute ventilation (in mL per min), and RQ; and segment total for minute ventilation (in liters).
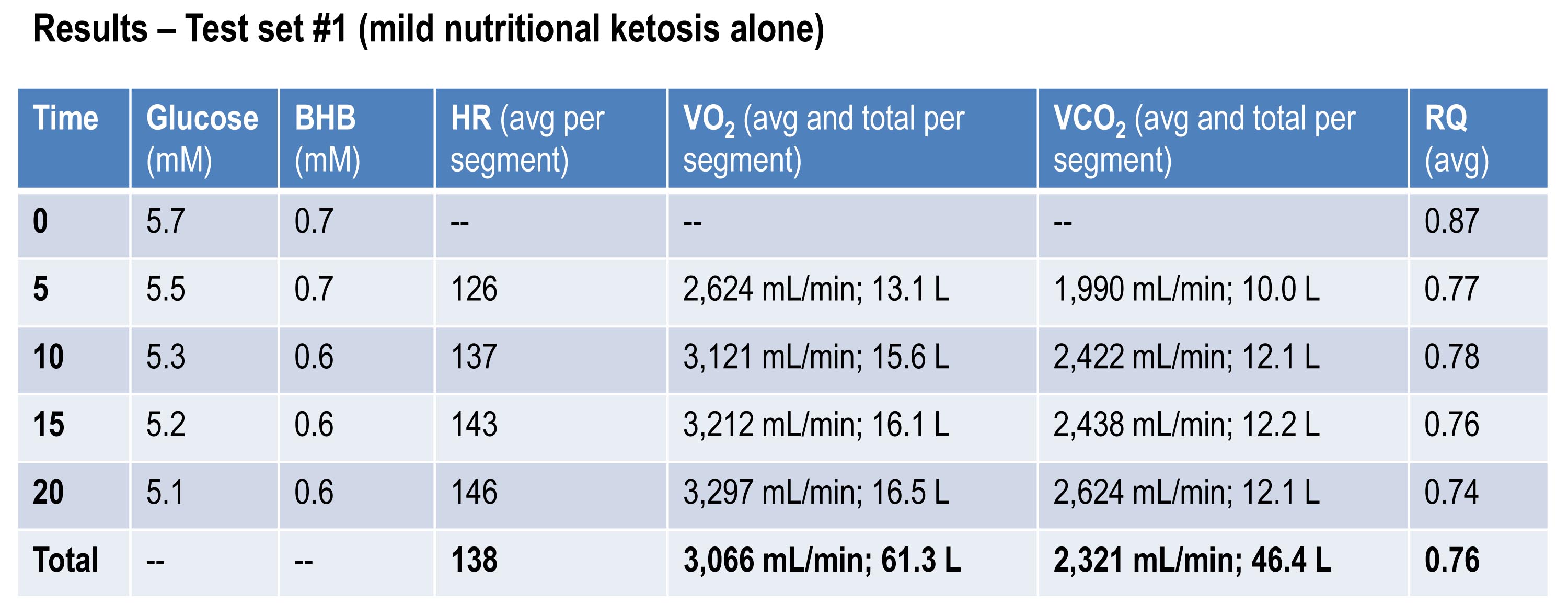
Glucose and BHB went down slightly throughout the effort and RQ fell, implying a high rate of fat oxidation. We can calculate fat oxidation from these data. Energy expenditure (EE), in kcal/min, can be derived from the VO2 and VCO2 data and the Weir equation. For this effort, EE was 14.66 kcal/min; RQ gives us a good representation of how much of the energy used during the exercise bout was derived from FFA vs. glucose—in this case about 87% FFA and 13% glucose. So fat oxidation was approximately 12.7 kcal/min or 1.41 g/min. It’s worth pointing out that “traditional” sports physiology preaches that fat oxidation peaks in a well-trained athlete at about 1 g/min. Clearly this is context limited (i.e., only true, if true at all, in athletes on high carb diets with high RQ). I’ve done several tests on myself to see how high I could push fat oxidation rate. So far my max is about 1.6 g/min. This suggests to me that very elite athletes (which I am not) who are highly fat adapted could approach 2 g/min of fat oxidation. Jeff Volek has done testing on elites and by personal communication he has recorded levels at 1.81 g/min. A very close friend of mine is contemplating a run at the 24 hour world record (cycling). I think it’s likely we’ll be able to get him to 2 g/min of fat oxidation on the correct diet.
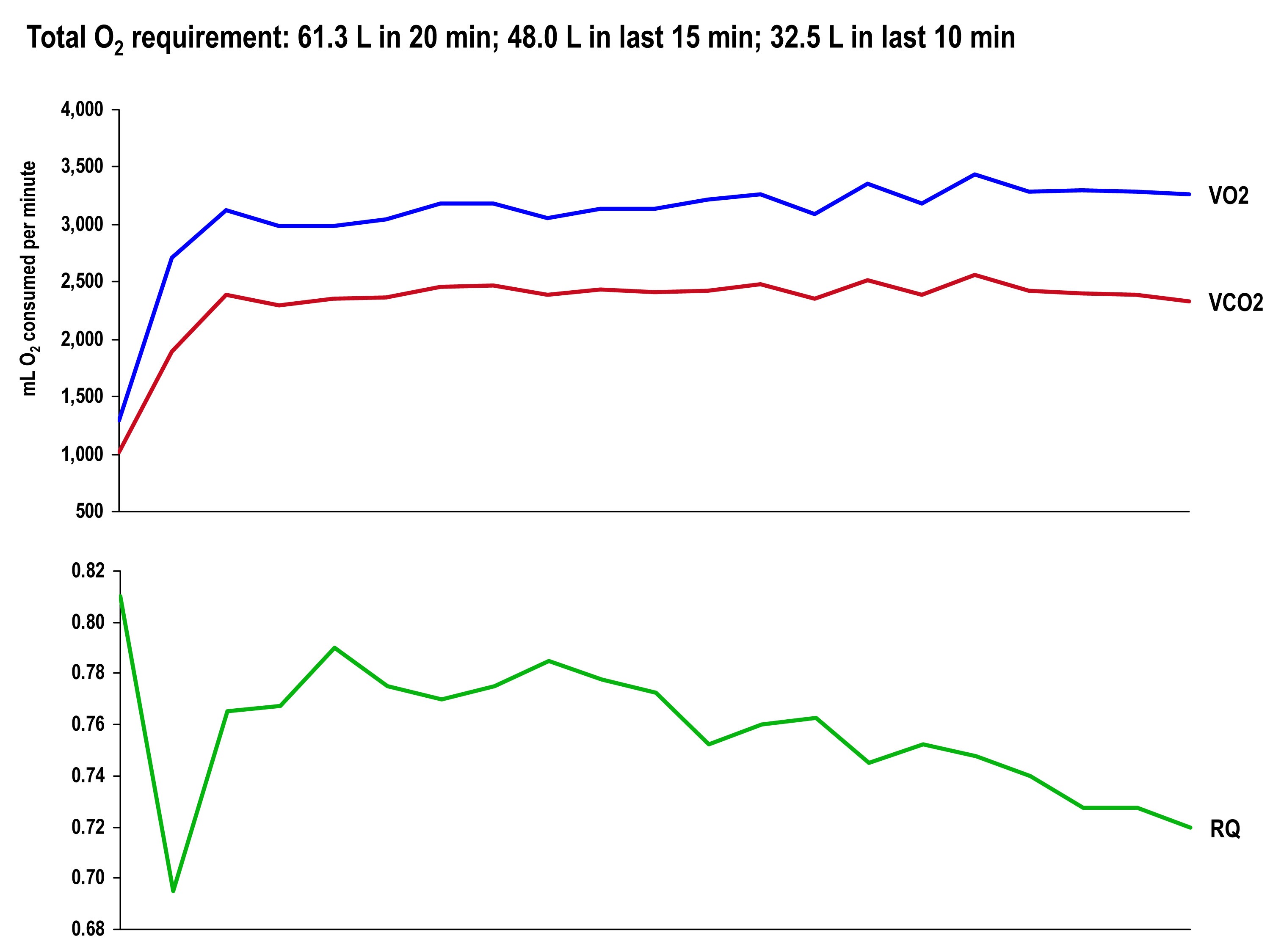
The graph, below, shows the continuous data for VO2, VCO2 (measured), and RQ (calculated).
Test set #2 (ingestion of 15.6 g BHB salt 60 minutes prior)
The table below shows the same measurements and calculations as the above table, but under the test conditions. You’ll note that BHB is higher at the start and falls more rapidly, as does glucose (for reasons I’ll explain below). HR data are almost identical to the control test, but VO2 and VCO2 are both lower. RQ, however, is slightly higher, implying that the reduction in oxygen consumption was greater than the reduction in carbon dioxide production.
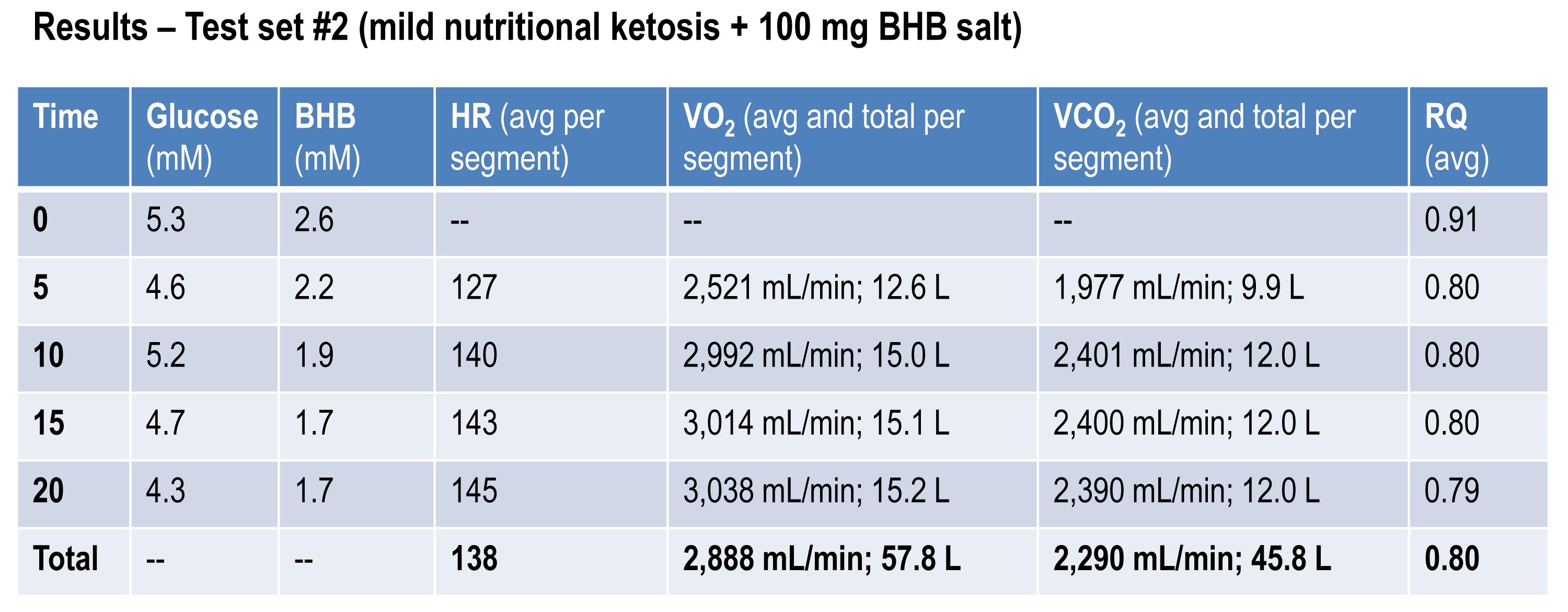
If you do the same calculations as I did above for estimating fat oxidation, you’ll see that EE in this case was approximately 13.92 kcal/min, while fat oxidation was only 67% of this, or 9.28 kcal/min, or 1.03 g/min. So, for this second effort (the test set) my body did about 5% less mechanical work, while oxidizing about 25% less of my own fat. The majority of this difference, I assume, is from the utilization of the exogenous BHB, and not glucose (again, I will address below what I think is happening with glucose levels).
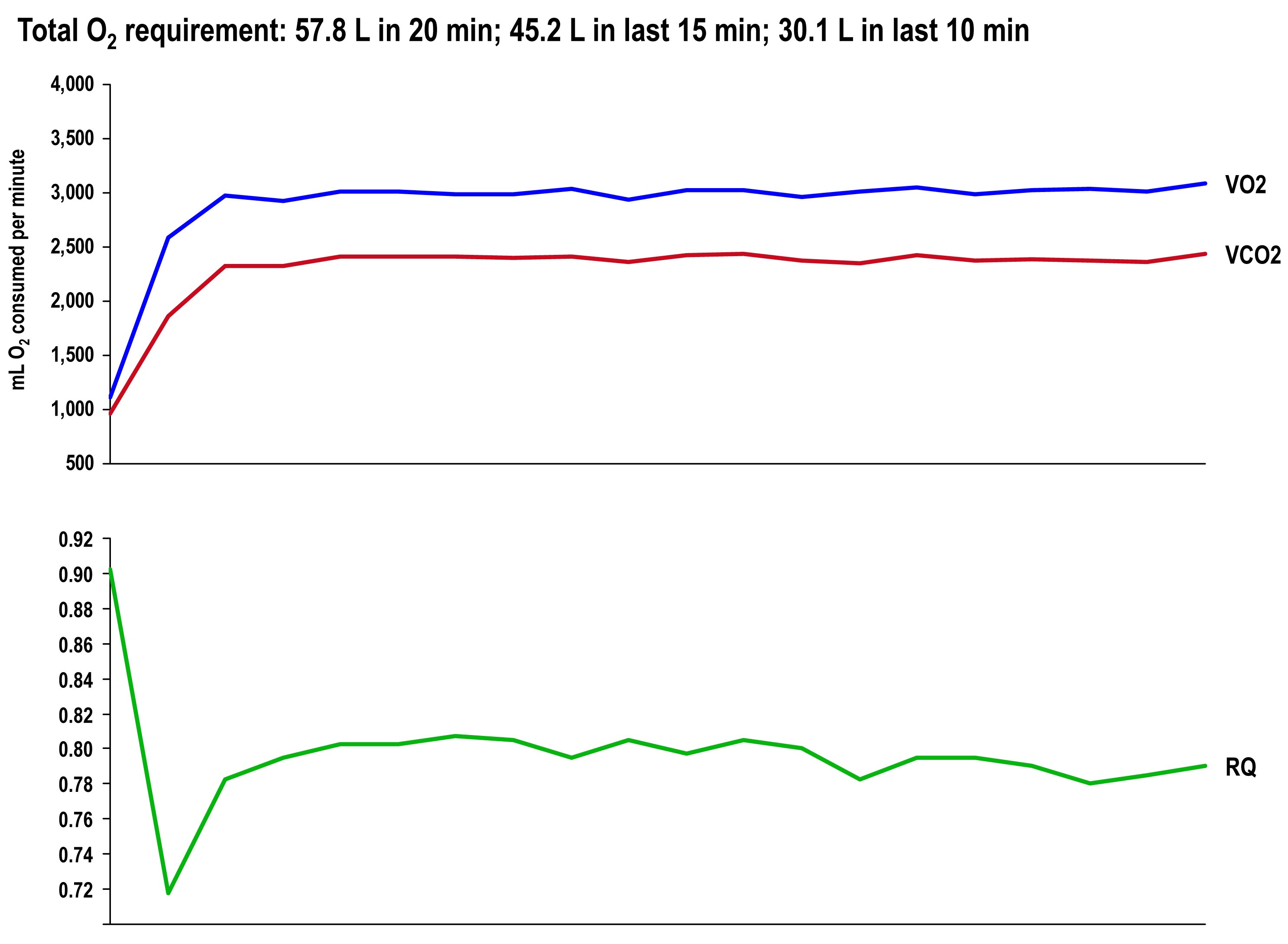
The graph once again shows the continuous data for VO2, VCO2 (measured), and RQ (calculated).
Side-by-side difference
The final graph, below, shows the continuous data for only VO2 side-by-side for the 20 minute period. The upper (blue) line represents oxygen consumption under control conditions, while the lower line (red) represents oxygen consumption following the BHB ingestion. In theory, given that the same load was being overcome, and the same amount of mechanical work was being done, these lines should be identical.
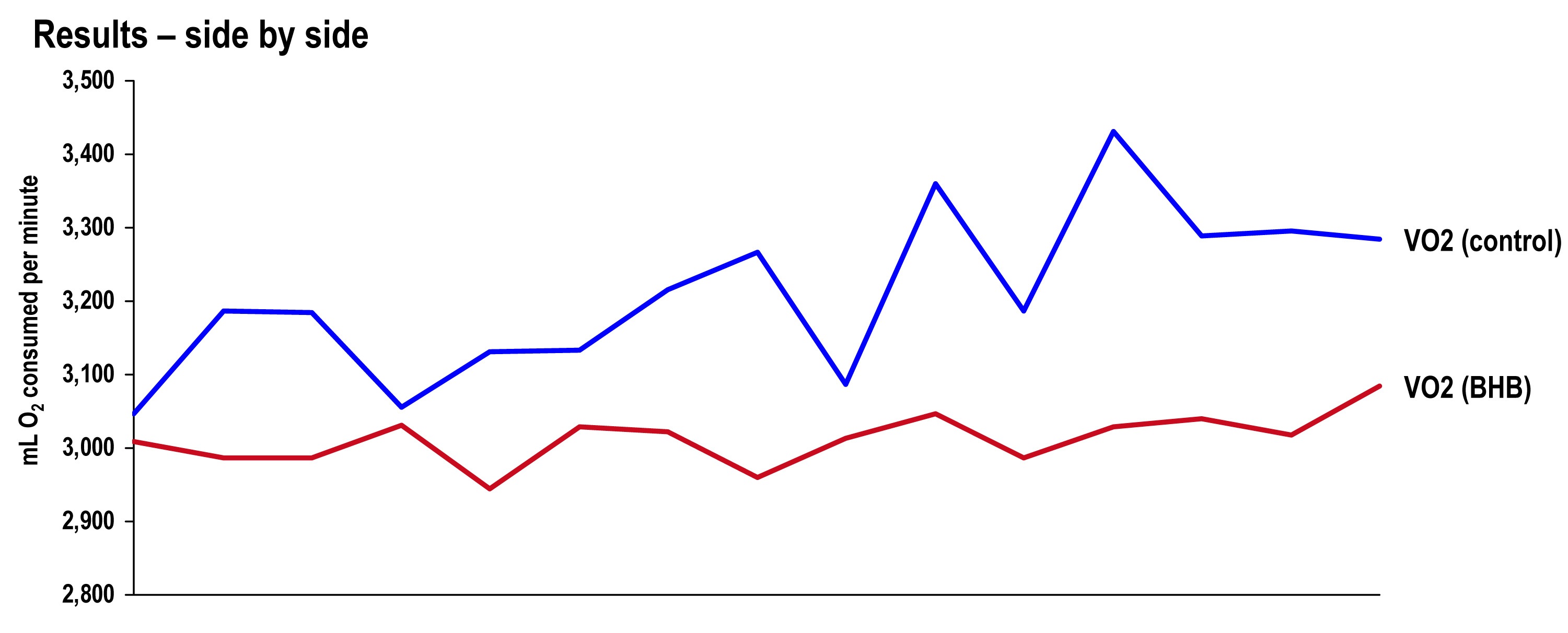
The hypothesis being tested in this “experiment” is that they would not be the same. Beyond visual inspection, the difference between the lines appears to grow as the test goes on, which is captured in the tabular data showing 5 minute segmental data.
Limitations
The most obvious limitation of this endeavor is the fact that it’s not an appropriately controlled experiment. Putting that aside, I want to focus on the nuanced limitations—which don’t impact the primary outcome of oxygen consumption—even if one were appropriately doing a real experiment.
- It’s not clear that the Weir coefficients used to estimate EE are relevant for someone in ketosis, let alone someone ingesting exogenous BHB. (The Weir formula states that EE is approximated by 3.94 * VO2 + 1.11 * VCO2, where VO2 and VCO2 are measured in L/min; 3.94 and 1.11 are the Weir coefficients, and they are derived by tabulating the stoichiometry of lipid synthesis and oxidation of fat and glucose and calculating the amount of oxygen consumed and carbon dioxide generated.) While this doesn’t impact the main observation—less oxygen was consumed with higher ketones—it does impact the estimation of EE and substrate use.
- In addition to the Weir coefficients being potentially off (which impacts EE), the RQ interpretation may be incorrect in the presence of endogenous or exogenous ketones. As a result, the estimation of fat and glucose oxidation may be off (though it’s directionally correct). That said, the current interpretation seems quite plausible—greater fat oxidation when I had to make my ketones; less when I got my ketones for “free.”
Observations from this “experiment” (and my experience, in general)
Animal models (e.g., using rat hearts) and unpublished case reports in elite athletes suggest supplemented BHB produces more ATP per unit carbon and per unit oxygen consumed than glycogen and FFA. This appears to have been the case in my anecdotal exercise.
The energy necessary to perform the mechanical work did not appear to change much between tests, though the amount of oxygen utilization and fat oxidation did go down measurably. The latter finding is not surprising since the body was not sitting on an abundant and available source of BHB—there was less need to make BHB “the old fashioned way.”
As seen in this exercise, glucose tends to fall quite precipitously following exogenous ketone ingestions. Without exception, every time I ingested these compounds (which I’ve probably done a total of 25 to 30 times), my glucose would fall, sometimes as low as 3 mM (just below 60 mg/dL). Despite this, I never felt symptomatic from hypoglycemia. Richard Veech (NIH) one of the pioneers of exogenous ketones, has suggested this phenomenon is the result of the ketones activating pyruvate dehydogenase (PDH), which enhances insulin-mediated glucose uptake. (At some point I will also write a post on Alzheimer’s disease, which almost always involves sluggish PDH activity —in animal models acute bolus of insulin transiently improves symptoms and administration of exogenous ketones does the same, even without glucose.)
In addition, the body regulates ketone production via ketonuria (peeing out excess ketones) and ketone-induced insulin release, which shuts off hepatic ketogenesis (the liver making more ketones when you have enough). The insulin from this process could be increasing glucose disposal which, when coupled with PDH activation, could drive glucose levels quite low.
If that explains the hypoglycemia, it would seem the absence of symptoms can be explained by the work of George Cahill (back in the day; see bottom figure in this post)—when ketone levels are high enough they can dominate brain fuel, even ahead of glucose.
Finally, these compounds seemed to have a profound impact on my appetite (they produced a strong tendency towards appetite suppression). I think there are at least two good explanations for this, which I plan to write about in a dedicated post. This particular topic—appetite regulation—is too interesting to warrant anything less.
Open questions to be tested in real experiments
- Are these results reproducible? If so, how variable are the results across individuals (by baseline metabolic state, diet, fitness)?
- Would the difference in oxygen consumption be larger (or smaller) in an athlete not already keto-adapted (i.e., not producing endogenous ketones)?
- Would the observed effect be greater at higher plasma levels of BHB (e.g., 5 to 7 mM), which is “easily” achievable with exogenous ketones?
- Would the observed effect be the same or different at higher levels of ATP demand (e.g., at FTP or at 85-95% of VO2 max)?
- Would the trend towards improved energy efficiency continue if the exercise bout was longer in duration (say, greater than 2 hours)?
- How will exogenous ketones impact exercise duration and lactate buffering?
- Why do exogenous ketones (both BHB and AcAc it seems) reduce blood glucose levels so much, and can this feature be exploited to treat type 2 diabetes?
- Are there deleterious effects from using exogenous ketones, besides GI side-effects?
- What are the differences between exogenous BHB and AcAc (which in vivo exist in a reversible equilibrium) on this particular phenomenon? (Work by Dom D’Agostino’s group and others have shown other differences in metabolic response and clinical application, including their relative impact on neurons.)
Photo by Alexey Lin on Unsplash

Peter,
I wonder whether you know or have in mind doing some other types of experiments relating to cognitive self-control. You have mentioned before that keto-adapted people seems “to work continuously” and don’t lose focus (it happens to me). I wonder whether one could design some experiments along the lines of
https://www.uky.edu/~njdewa2/gailliotetal07JPSP.pdf
to see whether giving exogenous ketones will improve attention in cognitive tasks.
Yes, I’d love to see such an experiment done well.
Hi Peter,
I recently saw you on video stating that your chosen food while training was carbohydrates – either by eating cashew nuts for slow release or “superstarch”. Would your results here change that choice in any way? I personally am considering using dried coconut meat instead of cashews due to the very high MCT oil content and the similar overall carb content – just a little lower than cashews.
Last weekend I was in a hill climbing (14km long and 1km vertical ) bicycle race and as I appear to be properly keto-adapted decided to attempt it in this state – with no additional carbs. The race took me 58 mins 53secs and my average heart rate was 95.4% of maximum over this period. My only addition was to supplement ketones about an hour before the start – from coconut oil. Only one one single occasion – 5 years ago at age 50 was I able to go under this time and match this heart rate – but I was using carbs. On that occasion I was noticeably breathing much more heavily and had a post exercise asthma attack immediately on stopping after crossing the finish line due to hyperventilation (the body eliminating CO2 to keep blood acid in balance). On this recent occasion – without carbs – there was no asthma attack. Mentally and physically I felt less stressed altogether and was totally surprised to be able to sustain such a high output level under ketosis.
I should add that my overall strength is relatively low at the moment due to having lost 28.5lb in weight over the last few months – due to both fasting and a ketogenic diet. Strength building will be on the cards soon instead of weight loss and I’m confident that next year the 90 second gap to my 5 year old record will be broken.
Don’t know where to post this but can you comment on this recent finding that artificial sweeteners have been shown to alter gut bacteria and create glucose intolerance?
https://www.sciencedaily.com/releases/2014/09/140917131634.htm
See response elsewhere on this thread.
Hi Peter,
Any quick comments on the new Nature study regarding artificial sweeteners? Have the results surprised you at all – particularly the 3rd part of the study (despite being very preliminary)?
The mouse data are useless. Who cares what happens in a mouse. Not the species of interest. The experiment that needs to be done is as follows:
2 groups eat the exact same food for 2 months Group 1: drinks 3 soda waters per day; Group 2: drinks 3 diet sodas per day
Both groups consume the same # of calories, type of calories, etc. and even same amount of fluid and carbonation.
Measure glucose disposal and other tests of insulin resistance pre- and post.
Easy study…hope it gets done. Until it does, I’m not convinced that diet soda is harmful, but it’s a very interesting question and it needs resolution.
Hi, Peter,
I have read Volek and Phinney, have followed Ben Greenfield, and a bit of the IF pioneers, and wonder how you would weigh in on low carb and thyroid issues? and, for that matter, higher cortisol levels in endurance athletes? I remember reading Ben Greenfield saying that you could potentially f**k up your thyroid doing low-carb and endurance training. And, despite doing all of what he suggests to curtail potential damage, how would I know if my thyroid was having issues?
I am a month in on a ketogenic diet and have had blood lipid tests (all of which have come back well within super-healthy) but I am having a hard time getting above 1.0 mM for blood ketones. I have just reached the peak of my training cycle (60-75 miles a week of running) and am beginning tapering for a 50K and for the most part, feel fine. And, worth noting, during the last month, I have at most used two servings of UCAN and Vespa in my 20-27 mile runs. I’m always surprised by how NOT hungry I am afterwards compared to when I was a carb-loader. However, I feel like I may not be reaping the full rewards/advantages of being in NK if I can’t push into the higher blood ketone levels.
Any pointers would be appreciated. And, this blog of yours is an absolute gold mine for any athlete dabbling in self experimentation to improve performance!
Thanks,
Leo
My thoughts and now my clinical experience on this topic are so complex that they warrant an entire blog post, rather than a quick response (at the risk of “pulling a Fermat”). But I don’t want to promise anything. Blogging is currently priority #11 on a list of 10 things in my life.
https://caloriesproper.com/ketoadaptation-and-physiological-insulin-resistance/ . Many people experience a drop in ketones after the intial adaption period. I think its important to consider if more ketones equal more performance, health etc. if you’re already doing good.
Hi Peter,
I remember someone asking you about what is your target market and your answer was, “I do not have one”. I think that you do have a “specific” target market, which are people who are not happy with the standard diet and they are looking for an alternative diet.
The reason I mentioned this is because I have discussed this with others and look at me like I have two heads. I have discussed it with a few doctors and some intelligent people (who are suppose to be open minded) and still, I get this crazy, you are dying from the inside look. And it is very, very difficult to even get some of these people to read the research or at least read about the subject. Your target market is a few step ahead from most people (maybe some are just jumping from diet to diets, but I would like to say most of your followers like the scientific research behind your information).
That out of the way….
All my life I have been checking my cholesterol (standard) and that’s what I have been going by. My doctor of course also recommends that (I do not have any cardiac conditions, but I like to know where I stand. I am 28). I started reading about nutrition about 7 months ago. I started reading about the people who disagree with the standard american diet and see what their reasons were. I started with the dietdoctor.com and from there I jumped on your blog and some other blogs as well. I like your blog because you are all about the numbers (which I think most of your followers like that about you).
I have an autoimmune disease (plaque psoriasis). I dropped eating grains 7 months ago and I lost about 20 pounds (in a 2 month period). My psoriasis is not as itchy but still there, still red. There is something else that is going on… I have read a few “autoimmune protocol” and have experimented (dropped all dairy) nothing. Now I read on thepaleomom.com which is the “Autoimmune Protocol”. Im a give it a try for 3 months or so and see if any changes happen. (Thought i’d tell you a little of my back story).
I have been reading about which tests to do (directlabs.com there is a never ending list). I like to know if what I am doing is helping or not, then modify it. I have been searching around how accurate these tests are, some say they are accurate and some say they are not (who to believe…).
All my life I thought the standard cholesterol was “it”. Predicting cardiac diseases. I do not have a medical background. The only knowledge I have gained is from reading your blog and others. Before this I was eating a “balanced” diet, spread your food throughout the day, UNINFORMED.
I never knew about NMR until I read it on your cholesterol series. And my doctor never recommended (I guess I am getting another doctor). I am a business person and my time and knowledge is business (human behavior as well, but that is more of a hobby). I do not have the time to read all of these theories about nutrition. Before I would ASSUME that the information out there was the BEST to the knowledge and tools we have in this society, which I was wrong…. So now I have to put the time myself to read all of the information that is out there and then make a decision of what/how I should eat among other things.
I noticed on your “coming soon” list there is a “What tests to get done if you want to track your health”. I think many people would benefit on your opinion of which tests to take. This way, they can track their health and modify it by their body’s reaction (which differs from person to person). I understand your schedule is extremely busy, but thought I’d share my input.
Thank you for what you are doing again.
(This was a quick ramble so dont mind structure of the paragraphs and the the grammatical errors)
Hi Peter,
Thank you for this great post and experiment, I hope it can be continued in a more intense research setting. Do you see any use for compound-specific isotope analyses in determining the actual source of material being utilized–for example, I am guessing that ketones that are burned from fat would have a different d13C than exogenous ketones, and you can even have an isotopic tracer attached to the exogenous ketones, so that you can isolate the CO2 released from respiration and determine the % of C from exogenous vs. endogenous ketones.
I have not yet gone through all of the comments so I don’t know if this has already been addressed, but can there be any detrimental side effects of having this amount of ketones?
I am at present in deep ketosis and training for mountain bike endurance racing. I raced my first 24 hour race very low carb and it went extremely well except for the terrible sinus headache I got from the weather/allergies. But, I didn’t have to eat much and I never bonked. If only I didn’t love pizza so much…
Peter,
Realised I have not commented on this post to date (the shame) as I have little to add but am continually fascinated with your n=1 adventures.
Wish to echo comments of others in that we really appreciate (& value) the time you devote to this, as nothing compares (that I have found). Your endless jet fuelled energy and GRIT are no doubt how you manage to accomplish so much.
As a parting note, let me add, the fact that you have no target audience is one of the things I (and probably others) like about you (or your blog) the most. It seems many want a chunk of your inquisitive mind (& time) but we are more than happy to settle for whatever crumbs you can spare.
Quality, not quantity.
Thank you, JJ. With that freedom I may start writing about even more of my far out obsessions…
There’s this show on Cinemax out now called The Knick. It shows us the life of early 1900 medicine and how medicine was still primitive with experiment procedures and people dying on the operating table normally, yet the doctors still fought the good fight. It’s really interesting.
Medicine and technology have advanced exponentially and while there’s always something new to learn, we’ve made large strides.
I was just thinking today how the field of nutrition is kinda in its primitive stages similar to how medicine is depicted on that show, figuratively speaking of course. Medicine has made those strides and nutrition still has yet to take major strides relative to medicine. If people really see the importance in it, as yourself, then maybe the field can grow.
What your doing with your organization should have been attempted 30 years ago. But it’s fine, we have technology now.
Fine. Here’s a better one.
Lebron James and Ray Allen adopt low carb. They site Volek. Things like this can help.
https://www.examiner.com/article/lebron-james-details-low-carb-ketogenic-paleo-weight-loss-no-sugar-for-67-days
Never discount the role of celebrities!
Peter,
Your emotional stretch in your TED presentation was inspirational. You model humility combined with the best forms of curiosity for those who care about health.
Might you comment upon breastfeeding versus manufactured “infant formula” as you may understand such from the dietary perspectives, such as ketonemia, you recognize and discuss for older folk?
Your leadership is desired!
Thank you for moving with your focus and your work!
Amita
Well, this is a topic near and dear to my heart as we have a 3 week old baby at home! I’m not an expert on this, and a lot of the data I’ve seen are weak. While I realize there are many circumstances that prevent women from being able to breastfeed it seems that doing so, especially early on, trumps formula. In addition to the benefits of BF (e.g., passive immunity), there are downsides to formula, namely the ingredients. On my to-do list is to find infant formula (I’m sure our little guy will need it eventually) that doesn’t contain crap.
Congratulations! We discovered neocate after many bad episodes with other formulas.
Excellent. Will check it out.
I thought I caught the phrase “my kids” (plural) in one of your posts. Congratulations on your new little guy! Wonderful news. PS Anecdote alert: I’ve also heard good things about neocate from a friend of mine who had trouble breastfeeding. For a funny, wise perspective on women who have challenges breastfeeding and the folks who judge them, read the relevant chapter in Bossypants, by Tina Fey.
Thank you, Kelley. The little guy is pretty cool. We’ve given him a great middle name, too.
Congratulations to the Attias!
Thank you so much!
Many congratulations on the new Addition to the family Peter! Wish you a happy and lessed family life .
Sorry, happy and BLESSED family life.
Appreciate it, Norm.
Yes, Peter, Congratulations, health, happiness, and contentment to your entire family! Thanks for sharing with us!
Thank you, Ellen!
Don’t assume your baby will need formula. It’s possible to utilize a little hormone hack that will reduce the amount of time spent pumping. Contact me if you are interested.
Hi Peter,
I didn’t know where to post this but was interested in your opinion given your experience. I just started a very low carb diet two weeks ago and my ketones raised to 0.5mmol/L today so officially ketoadapted I guess. I’ve done some mild intermiitent running with walking. I had my blood tests done a couple of days ago and the doctor said he could count on his hands how many times he gets blood tests that good. But what was the most interesting is it seems to have eliminated symptoms of my Thalassemia. As you probably know Thalassemia means I don’t bind iron very well, and I have never been able to give blood due to having such a low iron count. Here are my blood tests – https://saturatedinfats.com/2014/09/27/ketogenic-diet-has-eliminated-thalassemia/
The iron part is at the bottom. Do you have any idea as to why this might happen on a low carb diet?
Hi Daniel,
after two weeks you are probably not keto adapted but merely in ketosis – keto adaptation will usually only occur after 3+ weeks of constant ketosis and is characterised by your energy levels recovering to pre-ketosis levels, which is most likely due to mitochondrial ramp-up. check here; https://caloriesproper.com/ketoadaptation
Darkbloom
See an example paper below re a thalassemia strategy that I think applies in this situation. Butyric acid was an early agent of investigation into epigenetic effects of histone deacetylase inhibition. Butyrate circulates in small amounts normally, absorbed from microbial production in the distal gut. Beta-hydroxybutyrate, the ketone body, is a related molecule, and also an effective histone deacetylase inhibitor. See the very informative papers by Eric Verdin and JC Newman on this topic. HDAC inhibition permits transcriptional activity at the acetyated gene promotion sites. The idea is, you still have a silenced fetal globin gene, and if an agent can promote restoration of transcription of that, the beta-thalassemia may benefit. The HDAC activity of BHB was shown to promote a number of stress-response and antioxidant genes (catalase, superoxide dismutase, and others) and the full spectrum of genes promoted by this mechanism is not yet known. I suspect by increasing your circulating BHB you may be activating the transcription of fetal globin protein.
About a year ago, a U. of Oxford ketone body researcher shared with me that their group was seeking a grant for study of BHB in sickle cell anemia. That would possibly be the same strategy.
Rob Coberly
1. Experientia. 1993 Feb 15;49(2):133-7.
Butyrate-induced reactivation of the fetal globin genes: a molecular treatment
for the beta-hemoglobinopathies. Perrine SP(1), Faller DV.
**emphasis added below**
The inherited beta-hemoglobinopathies (sickle cell disease and beta thalassemia)
are the result of a mutation in the adult (beta) globin gene. The fetal globin
chain, encoded by the gamma globin genes, can substitute for the mutated or
defective beta globin chain, but expression of the gamma globin gene is
developmentally inactivated prior to birth. Re-inducing expression of the normal
fetal globin genes is a preferred method of ameliorating sickle cell disease and
the beta thalassemias. Stimulation of as little as 4-8% fetal globin synthesis in
the bone marrow can produce > 20% fetal hemoglobin in the peripheral circulation,
due to enhanced survival of red blood cells containing both sickle and fetal
hemoglobin, compared to those containing sickle hemoglobin alone. **Butyric acid
and butyrate derivatives are generally safe compounds which induce fetal
hemoglobin production by stimulating the promoter of the fetal globin genes.**An
initial trial with the parent compound, delivered as Arginine Butyrate, has
demonstrated rapid stimulation of fetal globin expression to levels that have
been shown to ameliorate these conditions. Phase 1 trials of an oral butyrate
derivative with a long plasma half-life have just begun. These agents now provide
a specific new approach for ameliorating these classic molecular disorders and
merit further investigation in larger patient populations.
PMID: 7680003 [PubMed – indexed for MEDLINE]
He won’t need “formula eventually” if you and your wife simply refuse to get involved in anything that would stop or hinder your wife from breastfeeding every moment of every day until your child weans himself or another baby comes along and takes his place. Our families and wives and children are everything there is in life. Totally 100%. A glorious and wonderful existence when we live it together 24/7 365 like nature intended. Always and forever. A gift to all who are smart enough to not let this be taken away from them.
Hi Peter,
I assume you have your reasons for not specifically answering my previous question about what supplements you would now choose to use during training session – given the effect of exogenous ketone (or more accurately MCT) supply.
I have a few observations to add. Bear in mind that I am supplementing both ketones and carbs in low quantities when training or racing.
Observation 1 – You appear to be correct in that any carbs consumed during an event – at least when consumed a few hours into the event – do not impact ketosis. You describe this as being due to a “carb debt”. (I have measured approx 1.7 mmol/L before a competition and 3.4 mmol/L after despite eating carbs) Reading about the Ranulph Feinnes/ Mike Stroud 1992/3 expedition to be the first ever to walk unaided across the Antarctic however raises a question mark over the “carb-debt” idea. The two adventurers – in a bid to reduce their carrying weight ended up with a high concentration of fat for their food – which I calculate to have provided 75% of their calories. They were burning over 11,000 Kcal per day – every day for 6 weeks – measured using radio isotopes. They took blood samples every few days. By the end of their trip their blood glucose levels were so low they would normally have been dead at 0.2 mmol/L. When the readings were analysed the medical experts initially thought they were simply in error – but they were not.
My point is this: What is a “Carb-debt” when the body can apparently normalise to 0.2 mmol/L? Would it not be better to aim for this than feed a system (with carbs) that assumes 4 mmol/L minimum is “normal” and necessary?
Observation 2 – During cycling competition I can maintain an anaerobic level for over 4 hours with much of this apparently “red-lining”. So if I’m now not actually burning carbs and burning ketones instead then is this actually correct to call this “anaerobic” in the sense of being 70% carb burning – which it now clearly is not?
Observation 3 – At almost exactly 4 hours and 30 minutes into an event – no matter what I’ve been doing in terms of effort up to this point – there is an effect like a switch being thrown that brings a strong resurgence of energy. This doesn’t affect heart rate but it allows much more power to be accessed without a raise in average heart rate. So far once this has started it remains constant until the termination of the event – from two to three hours later. I have absolutely no idea why this happens – but I can almost set my watch by it because the timing is so precise.
I’m in an introductory biology class and we are learning about glycolysis, gluconeogenesis, and what happens to the food you eat. However, no mention of ketosis. Wish there was something about fat metabolism in my textbook.
Dang.
p.s. Peter, you are my idol! I am majoring in biochemistry, and I think my interest is inspired by this blog.
Hmmm, keep looking, it’s got to be in there somewhere! Or recommend a better text to the prof.