I wrote this post almost six years ago (March 21, 2012), but it’s the gift that keeps on giving.
These days, I feel a lot like Bill Murray in Groundhog Day, where at least a few times a year, my inbox is stuffed with concerned individuals forwarding me a paper (or, much more the case, a story about a paper) implying red meat is going to send me to an early grave. The irony is that being stuck in some sort of sadistic red-meat time loop probably will do the trick. But at least I have meditation to help with that.
To be fair, the red-meat-studies are not the only culprit. As I mentioned in a Nerd Safari on epidemiology, John Ioannidis and Jonathan Schoenfeld picked 50 ingredients at random out of a cookbook and determined if each was associated with cancer. They found that at least one study was identified as showing an association for an increase or decrease in cancer for 40 out of the 50 ingredients. (The 10 that didn’t make the list were more “obscure,” as the authors put it: bay leaf, cloves, thyme, vanilla, hickory, molasses, almonds, baking soda, ginger, and terrapin. Thank heavens I can still have my terrapin.)
It’s probably not unfair to say that I put together this post as a coping mechanism. Fight fire with fire. You want a time loop? You may see the following post make its way to the front of the queue several times a year. While it’s of course not the best tack for me to close my eyes and block my ears to the latest article that forces a visceral reaction, it’s important to put things in context first.
This time around, I’m posting not because a new study just came out on red meat and mortality (although I haven’t checked my email in the past five minutes), but because we’re doing a series on this very topic of observational epidemiology.
Studying Studies: Part I – relative risk vs. absolute risk
Studying Studies: Part II – observational epidemiology
Studying Studies: Part III – the motivation for observational studies
I must admit, re-reading this post for the first time, I thought to myself, ‘Wow, Peter. Chill out…you really wrote that?’ Kinda like when I look at a picture of me from the 90’s. Dude, you wore that?
—P.A., January 2018
§
“For the greatest enemy of truth is very often not the lie—deliberate, contrived and dishonest—but the myth—persistent, persuasive, and unrealistic. Too often we hold fast to the clichés of our forebears. We subject all facts to a prefabricated set of interpretations. We enjoy the comfort of opinion without the discomfort of thought.”
– John F. Kennedy, Yale University commencement address (June 11, 1962)
I’m going to devote this post to a discussion on what I like to call the Scientific Weapon of Mass Destruction: observational epidemiology, at least for public health policy
I had always planned to write about this most important topic soon enough, but the recent study out of Harvard’s School of Public Health generated more than enough stories like this one such that I figured it was worth putting some of my other ideas on the back-burner, at least for a week. If you’ve been reading this blog at all you’ve hopefully figured out that I’m not writing it to get rich. What I’m trying to do is help people understand how to think about what they eat and why. I have my own ideas, shared by some, of what is “good” and what is “bad,” and you’ve probably noticed that I don’t eat like most people.
However, that’s not the real point I want to make. I want to help you become thinkers rather than followers, at least on the topic of health sciences. And that includes not being mindless followers of me or my ideas, of course. Being a critical thinker doesn’t mean you reject everything out there for the sake of being contrarian. It means you question everything out there. I failed to do this in medical school and residency. I mindlessly accepted what I was taught about nutrition without ever looking at the data myself.
Too often we cling to nice stories because they make us feel good, but we don’t ask the hard questions. You’ve had great success improving your health on a vegan diet? No animals have died at your expense. Great! But, why do you think it is you’ve improved your health on this diet? Is it because you stopped eating animal products? Perhaps. What else did you stop eating? How can we figure this out? If we don’t ask these questions, we end up making incorrect linkages between cause and effect. This is the sine qua non of bad science.
Most disciplines of science—such as physics, chemistry, and biology—use something called the Scientific Method to answer questions. A simple figure of this approach is shown below:
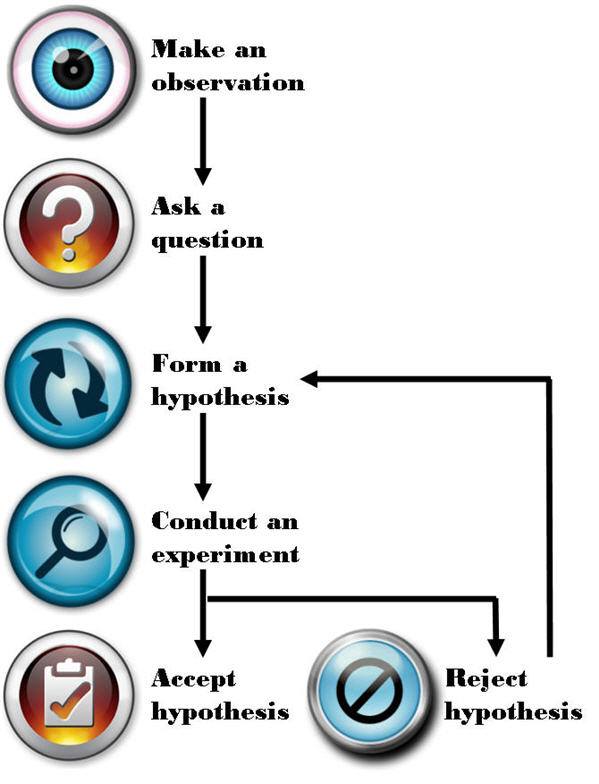
The figure is pretty self-explanatory, so let me get to the part that observational epidemiology inherently omits: “Conduct an experiment.” There is no shortage of observations, questions, or hypotheses in the world of epidemiology and public health—so we’re doing well on that front. It’s that pesky experiment part we’re getting hung up on. Without doing controlled experiments it is not possible to distinguish the relationship between cause and effect.
What is an experiment?
There are several types of experiments and they are not all equally effective at determining the cause and effect relationship. Climate scientists and social economists (like one of my favorites, Steven Levitt), for example, often carry out natural experiments. Why? Because the “laboratory” they study can’t actually be manipulated in a controlled setting. For example, when Levitt and his colleagues tried to figure out if swimming pools or guns were more dangerous to children—i.e., Was a child more likely to drown in a house with a swimming pool or be shot by a gun in a home with a gun?—they could only look at historical, or observational, data. They could not design an experiment to study this question prospectively and in a controlled manner.
How would one design such an experiment? In a “dream” world you would find, say, 100,000 families and you would split them into two groups—group 1 and group 2. Group 1 and 2 would be statistically identical in every way once divided. Because of the size of the population, any differences between them would cancel out (e.g., socioeconomic status, number of kids, parenting styles, geography). The 50,000 group 1 families would then have a swimming pool installed in their backyard and the 50,000 group 2 families would be given a gun to keep in their house.
For a period of time, say 5 years, the scientists would observe the differences in child death rates from these two causes (accidental drownings and gunshot wounds). At the conclusion, provided the study was powered appropriately, the scientists would know which was more hazardous to the life of a child, a home swimming pool or a home gun.
Unfortunately, questions like this (and the other questions studied by folks like Levitt) can’t be studied in a controlled way. Such studies are just impractical, if not impossible, to do.
Similarly, to rigorously study the anthropogenic CO2 – climate change hypothesis, for example, we would need another planet earth with the same number of humans, cows, lakes, oceans, and kittens that did NOT burn fossil fuels for 50 years. But, since these scenarios are never going to happen the folks that carry out natural experiments do the best they can to statistically manipulate data to separate as many confounding factors as possible in every effort to identify the relationship between cause and effect.
Enter the holy grail of experiments: the controlled experiment. In a controlled experiment, as the name suggests, the scientists have control over all variables between the groups (typically what we call a “control” group and a “treatment” group). Furthermore, they study subjects prospectively (rather than backward-looking, or retrospectively) while only changing one variable at a time. Even a well-designed experiment, if it changes too many variables (for example), prevents the investigator from making the important link: cause and effect.
Imagine a clinical experiment for patients with colon cancer. One group gets randomized to no treatment (“control group”). The other group gets randomized to a cocktail of 14 different chemotherapy drugs, plus radiation, plus surgery, plus hypnosis treatments, plus daily massages, plus daily ice cream sandwiches, plus daily visits from kittens (“treatment group”). A year later the treatment group has outlived the control group, and therefore the treatment has worked. But how do we know EXACTLY what led to the survival benefit? Was it 3 of the 14 drugs? The surgery? The kittens? We cannot know from this experiment. The only way to know for certain if a treatment works is to isolate it from all other variables and test it in a randomized prospective fashion.
As you can see, even doing a prospective controlled experiment is not enough, like the one above, if you fail to design the trial correctly. Technically, the fictitious experiment I describe above is not “wrong,” unless someone—for example, the scientist who carried out the trial or the newspapers who report on it—misrepresented it.
If the New York Times and CNN reported the following: New study proves that kittens cure cancer! would it be accurate? Not even close. Sadly, most folks would never read the actual study to understand why this bumper-sticker conclusion is categorically false. Sure, it is possible, based on this study, that kittens can cure cancer. But the scientists in this hypothetical study have wasted a lot of time and money if their goal was to determine if kittens could cure cancer. The best thing this study did was to reiterate a hypothesis. Nothing more. In other words, this experiment (even assuming it was done perfectly well from a technical standpoint) learned nothing other than the combination of 20 interventions was better than none because of an experimental design problem.
So what does all of this have to do with eating red meat?
In effect, I’ve already told you everything you need to know. I’m not actually going to spend any time dissecting the actual study published last week [March 12, 2012] that led to the screaming headlines about how red meat eaters are at greater risk of death from all causes (yes, “all causes,” according to this study) because it’s already been done a number of times by others this week alone. Three critical posts on this specific paper can be found here, here, and here.
I can’t suggest strongly enough that you read them all if you really want to understand the countless limitations of this particular study, and why its conclusion should be completely disregarded. If you want bonus points, read the paper first, see if you can understand the failures of it, then check your “answer” against these posts. As silly as this sounds, it’s actually the best way to know if you’ve really internalized what I’m describing.
Now, I know what you might be thinking: Oh, come on Peter, you’re just upset because this study says something completely opposite to what you want to hear.
Not so. In fact, I have the same criticism of similarly conducted studies that “find” conclusions I agree with. For example, on the exact same day the red meat study was published online (March 12, 2012) in the journal Archives of Internal Medicine, the same group of authors from Harvard’s School of Public Health published another paper in the journal Circulation. This second paper reported on the link between sweetened beverage consumption and heart disease, which “showed” that consumption of sugar-sweetened beverages increased the risk of heart disease in men.
I agree that sugar-sweetened beverages increase the risk of heart disease (not just in men, of course, but in women, too) along with a whole host of other diseases like cancer, diabetes, and Alzheimer’s disease. But, the point remains that this study does little to nothing to add to the body of evidence implicating sugar because it was not a controlled experiment.
This problem is actually rampant in nutrition
We’ve got studies “proving” that eating more grains protect men from colon cancer, that light-to-moderate alcohol consumption reduces the risk of stroke in women, and that low levels of polyunsaturated fats, including omega-6 fats, increase the risk of hip fractures in women. Are we to believe these studies? They sure sound authoritative, and the way the press reports on them it’s hard to argue, right?
How are these studies typically done?
Let’s talk nuts and bolts for a moment. I know some of you might already be zoning out with the detail, but if you want to understand why and how you’re being misled, you actually need to “double-click” (i.e., get one layer deeper) a bit. What the researchers do in these studies is follow a cohort of several tens of thousands of people—nurses, health care professionals, AARP members, etcetera—and they ask them what they eat with a food frequency questionnaire (FFQ) that is known to be almost fatally flawed in terms of its ability to accurately acquire data about what people really eat. Next, the researchers correlate disease states, morbidity, and maybe even mortality with food consumption, or at least reported food consumption (which is NOT the same thing). So, the end products are correlations—eating food X is associated with a gain of Y pounds, for example. Or eating red meat three times a week is associated with a 50% increase in the risk of death from falling pianos or heart attacks or cancer.
The catch, of course, is that correlations hold no causal information. Just because two events occur in step does not mean you can conclude one causes the other. Often in these articles you’ll hear people give the obligatory, “correlation doesn’t necessarily imply causality.” But saying that suggests a slight disconnect from the real issue. A more accurate statement is “correlation does not imply causality” or “correlations contain no causal information.”
So what explains the findings of studies like this (and virtually every single one of these studies coming out of massive health databases like Harvard’s)?
For starters, the foods associated with weight gain (or whichever disease they are studying) are also the foods associated with “bad” eating habits in the United States—french fries, sweets, red meat, processed meat, etc. Foods associated with weight loss are those associated with “good” eating habits—fruit, low-fat products, vegetables, etc. But, that’s not because these foods cause weight gain or loss, it’s because they are markers for the people who eat a certain way and live a certain way.
Think about who eats a lot of french fries (or a lot of processed meats). They are people who eat at fast food restaurants regularly (or in the case of processed meats, people who are more likely to be economically disadvantaged). So, eating lots of french fries, hamburgers, or processed meats is generally a marker for people with poor eating habits, which is often the case when people are less economically advantaged and less educated than people who buy their food fresh at the local farmer’s market or at Whole Foods. Furthermore, people eating more french fries and red meat are less health conscious in general (or they wouldn’t be eating french fries and red meat—remember, those of us who do eat red meat regularly are in the slim minority of health-conscious folks). These studies are rife with methodological flaws, and I could devote an entire Ph.D. thesis to this topic alone.
What should we do about this?
I’m guessing most of you—and most physicians and policy makers in the United States for that matter—are not actually browsing the American Journal of Epidemiology (where one can find studies like this all day long). But occasionally, like last week, the New York Times, Wall Street Journal, Washington Post, CBS, ABC, CNN, and everyone else gets wind of a study like the now-famous red meat study and comments in a misleading fashion. Health policy in the United States—and by extension much of the world—is driven by this. It’s not a conspiracy theory, by the way. It’s incompetence. Big difference. Keep Hanlon’s razor in mind—Never attribute to malice that which is adequately explained by stupidity.
This behavior, in my opinion, is unethical and the journalists who report on it (along with the scientists who stand by not correcting them) are doing humanity no favors.
I do not dispute that observational epidemiology has played a role in helping to elucidate “simple” linkages in health sciences (e.g., contaminated water and cholera or the linkage between scrotal cancer and chimney sweeps). However, multifaceted or highly complex pathways (e.g., cancer, heart disease) rarely pan out, unless the disease is virtually unheard of without the implicated cause. A great example of this is the elucidation of the linkage between small-cell lung cancer (SCLC) and smoking—we didn’t need a controlled experiment to link smoking to this particular variant of lung cancer because nothing else has ever been shown to even approach the rate of this type of lung cancer the way smoking has (reported relative risk of SCLC in current smokers of more than 1.5 packs of cigarettes a day was 111.3 and 108.6, respectively—over a 10,000% relative risk increase). As a result of this unique fact, Richard Doll and Austin Bradford Hill were able to design a clever observational analysis to correctly identify the cause and effect linkage between tobacco and lung cancer. But this sort of example is actually the exception and not the rule when it comes to epidemiology.
Whether it’s Ancel Keys’ observations and correlations of saturated fat intake and heart disease in his famous Seven Countries Study, which “proved” saturated fat is harmful or Denis Burkitt’s observation that people in Africa ate more fiber than people in England and had less colon cancer “proving” that eating fiber is the key to preventing colon cancer, virtually all of the nutritional dogma we are exposed to has not actually been scientifically tested. Perhaps the most influential current example of observational epidemiology [circa 2012] is the work of T. Colin Campbell, lead author of The China Study, which claims, “the science is clear” and “the results are unmistakable.” Really? Not if you define science the way scientists do. This doesn’t mean Colin Campbell is wrong (though I wholeheartedly believe he is wrong on about 75% of what he says based on current data). It means he has not done sufficient science to advance the discussion and hypotheses he espouses. If you want to read detailed critiques of this work, please look to Denise Minger and Michael Eades. I can only imagine the contribution to mankind Dr. Campbell could have given had he spent the same amount of time and money doing actual scientific experiments to elucidate the impact of dietary intake and chronic disease. [For example, Campbell would have designed a prospective study following subjects randomized to one of two different types of diets for 10 years: plant-based and animal-based, but with all other factors controlled for.] This is one irony of enormous observational epidemiology studies. Not only are they of little value, in a world of finite resources, they detract from real science being done.
Featured Image credit: Design by K. Pauley (CC BY-SA 2.0)



Here is a link to example 2xw2 Designed Experiment https://web.mst.edu/~psyworld/between_subjects.htm
Great post as always Pete. I can not believe how many posts you respond to – amazing. Keep it up bro!
Thanks, John. Glad you enjoyed it. Hope it helps with family questions.
This is a terrific post. You take a complicated subject and dissect it in a clear, lucid style that can be easily understood by people who never thought once about the validity of these nutritional studies. Thank you. I’m going to share this article with as many people as I can.
I read the sugar study as well, and thought, oh, this is coming from the same study on red meat. Well, this is worthless.
“Whole Paycheck” is what everyone calls it around here.
Peter wrote: “You’ve had great success improving your health on a vegan diet? No animals have died at your expense. Great!”
Oh, but animals DID die. That’s the thing that’s so dishonest about the vegans’/vegetarians’ “ethical” stance — and so aggravating when they try to push their agenda on the rest of us. What do they think happens to all the gophers and rabbits and snakes and birds, etc., etc., etc. that are in the fields when the plows and the planters and the combines go through to produce the soy and the grain for their tofu burgers?
Good point, especially given that these animals were just chopped up by the machines. For people who are concerned about animal welfare make sure the meat you eat comes from animals that were humanely raised (pasture-fed), transported and slaughtered. That way their meat contains fewer stress hormones and is healthier, too.
Most of that corn and soy feed the livestock to support the meat industry. Plus the animals in the meat industry are in prison. They can’t leave and are not free to move to a different field. The animals in the fields have the “FREEDOM” to move to a different field. This simply boils down to intentions: in the meat industry the intentions are to kill. If an animal is sad to say accidentally run over by a plow, then it was an accident. And as I said earlier, most of the corn and soy feed the animals intended to be slaughtered. You can’t win this argument on ethics here. Vegans and Vegetarians give up meat because it actually does save lives of animals. On top of that, most of them try not to hurt flies or spiders in the house. They don’t use mouse traps. They try not to wear leather unless maybe it is from a second hand store. They do a lot for ethics for animals and this is debate will always win because it is so obvious.
I love this blog. Perfect science reading for my 14-year-old daughter’s homeschooling for tomorrow. I wish all kids learned this in highschool and we’d have far fewer sick people in this country who believe everything their doctors tell them without asking questions and doing their own research. Keep up the good work. 🙂
Birgit
“Reading stupid epidemiology studies INCREASE all causes of MORTALITY”. All the stress and needless excess worrying is killing people that beside all the wrong and contradictory advice they get from them. I just need some funding to show causality. Je,je
In another matter I wanted to ask you Peter. I have a friend who I recommended a kenotic diet because he needed to lose some weight to lower BP. I talked to him the other day and he told me he was very happy with the results. That also he had been suffering from Fibromyalgia all his life and the kenotic diet had resolved all his symptoms. The pain, mental fog and mood swing etc. I was quite surprise. Do you know of any plausible mechanics on why the kenotic may help with Fibromyalgia?
Sam, I have heard this from others also, but have not had the time to really dig into the mechanism of action. Glad to hear he’s having great results.
If you google “primal” or “paleo” diet you might find a possible mechanism. I don’t remember the ins and outs precisely, but they propose that many auto-immune disorders are caused by food antigens that screw with the immune response. Something about gluten and other grain based prolamines affecting the trans-glutaminase system which is found in tissues all over the body, and therefore can explain the resolution of neurological/dermatologic/orthopedic/systemic inflammation/etc problems when people go “paleo”.
It’s an interesting idea, but to my knowledge it has not been rigorously tested yet. The sheer number of people who have resolution of symptoms once they stop eating grains/beans makes me think there is “something” there.
Hi Sam,
I started a ketogenic diet 3 years ago, as I heard it can help reduce chronic pain. I was told I had Fibromyalgia. Within a few months, my pain level was reduced. Also my blood pressure was more normal, my low blood sugar was more controlled, and my mood improved. Also my overactive bladder was no longer overactive. My social anxiety was reduced, and I lost the 20 pounds I was overweight. On such a diet, as to pain, well grains and sugar seem to cause inflammation, and we are without those, and the brain runs on ketone bodies, which increases Gaba, and reduces glutamate. This seems to reduce pain levels. Here is one study, but it admits this is a hypothesize. MSG consumption has been suggested as a trigger for Fibro.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2722878/
I am just glad I started the diet, but just wish I had known all this years ago. I read Sugar Blues, and 2 more books on sugar in the 1970s, and I cut down a lot, but those books did not mention ketosis(very low carb and high fat), much at that time.
At the end of the day, doing a controlled experiment on anything to do with human metabolism is nearly impossible. I am a chemical engineer with a six sigma background and have done my share of experiments following the scientific method. Pick a key input varable, change it and observe the change in output. Simple. With metabolic science, there are too many variables that we can’t control in a sample group greater than n=1. To conduct an even remotely meaningful experiment on red meat consumption, you would have to prescribe (and assume that they are followed) EXACT diets for all participants, with one group getting red meat and the other getting none. Macronutrient composition would have to be identical, calorie intake on some normalized basis would have to be identical, exercise, sleep, sun exposure, climate exposure, and a myriad of other things would all have to be the same for the results to mean anything at all. Not Possible. Then, you can throw in the question of genitics and everything goes right out the window.
For those of us who have reson to tinker with our diets, the only experiment that matters has n=1. Read everything you like. If you find a hypothesis that you think has merit, do a controlled experiment on yourself. If after changing a variable, you burn excess fat, feel better, have a better lipid profile, can get off your meds or whatever improves your being, then you have proven something that works for you. If you fail to lose fat, feel worse, or whatever, then you go back to the start and try changing something else. Again, simple (if you have the discipline to track inputs and outputs and record results.)
Seven months ago I started eating a low carb diet. I was 341 lbs with a lean body mass of 210 lbs. Between September and Christmas, I weighed and measured food, wrote down everything I ate, tracked macronutrient consumption and calories, and tracked ketosis. I lost about 40 lbs of fat while keeping lean mass essentially constant. Then the weight loss slowed and stopped. I still felt good but was frustrated and stuck at 300lbs. What changed you ask? I stopped tracing everything because I had been doing it for so long that I just knew what to eat. I recently posted another comment and asked Peter for some suggestion on what to change to restart the fat loss. I knew the answer to the question before I posted it, I had just gotten lazy. Peter suggested changing only one variable at a time and it dawned on me that I was no longer being scientific. I started weighing, writing, and checking again. I was no longer in ketosis despite very low carb intake, but my protein intake had increased. I reduced my protein intake and voila…. ketosis returned and so did fat loss. I am now at 289 and dropping.
Food is the most powerful drug on the planet. Don’t ever believe otherwise. Unfortunately, unlike other addictive substances, you can’t just stop taking it. The results of that expoeriment would not be good. So, we are stuck trying to manage a necessary addiction while weeding through the advice of the so called “experts” on how best to do so.
Dr. Attia IS an expert on this stuff and his opinions are very much worthy of your attention. However, he is an expert on what optimizes HIS health and performance, not necessarily yours. He is disciplined enough to do controlled experiments on himself and report the results to the rest of us as a hypothesis that we can attempt to prove in our own n=1 experiments. At the end of the day, n=1 is really all that matters to you.
Thank you for doing this Peter, it is great and necessary work!
Mike.
From the science point of view, what valid cases are there for only doing observational studies?
You pointed out that in the case of climate science and social economics, it is impossible to do a clinical study. Is this the only valid case? What makes it “impossible” enough to justify only observational studies?
It sounds to me like there is no valid reason to *not* do clinical studies in nutrition, because “hard” is not “impossible”.
As a side note, when it is “impossible”, how do you then do science with only observational studies?
See post. I address all of these questions.
Have you thought of approaching the Gates Foundation to fund research on low carb/high fat diets? While their Global Health Initiative seems to focus mostly on infectious diseases, I think you could make a detailed and strongly supported argument that the “diseases of western civilization” (diabetes, heart disease, etc) also have a strong impact on global health and deserve funding consideration. They see themselves as funding research that is “outside of the box”, which pretty much describes low carb/high fat diets given the current conventional nutrition wisdom. Of course they may open themselves up to ridicule, but they’ve shown with some of their funding decisions that they are willing to weather the controversy…and they have the money and independence to do it.
Yes. Lots of ideas like this in store. Of course, not sure if this will interest them, but we’ll ask.
I found another good quote,
“If we are to believe this hypothesis we must forget everything we learned in the last 70 years and start all over again.” Thomas Chamberlain a pre-eminent geologist upon hearing Alfred Wegener talk about “continental drift” and the evidence he’d collected to demonstrate its reality.
I could so easily imagine somebody saying the exact same thing to Gary Taubes…
Hi Peter,
Apologies if you have addressed this in another post or question. I haven’t been cheating on you by visiting naughty web sites, but I came across the PCRM site and noted they too are promoting the red meat is killing us so called study. I also noticed the following:
https://www.pcrm.org/media/news/billboard-warns-chicago-of-hot-dog-butt-cancer
I wonder if it is the hotdog or the white processed bun with more cancer causing potential? I also noticed than unlike your web site where we are free to comment, free to question, and you are not afraid to answer, there was no way of commenting on their blog pages. What do they have to hide?
No idea…
Hi Peter,
Here’s my n=1 experiment. For years I ate ‘virtuously’: high-complex carbs (300-400 grams per day) from brown rice, legumes, whole-grain flour, fruit and vegs, lean protein, minimal fat (olive/poly veg oil). I exercised 4x per week (4 miles treadmilled @12% incline, weight-lifting). Slim and trim ,I weighted about 127 pounds. Still my TC kept climbing over time.
Then my lipid panel
Dec 17, 2010 Pre-statin lipid panel
Total Cholesterol: 206
Triglyceride: 61
HDL: 42
LDL 152
alarmed my doc, blamed it on genetic traits and prescribed me statin Simvastatin on 12/24/10. I continued to eat the same high-carb way and maintained the same workout routine. Statin worked its magic on TC as shown in next 2 results:
Feb 1, 2011 Statin lipid panel
Total Cholesterol: 121
Triglyceride: 68
HDL: 41
LDL 66
Aug 3, 2011 Statin lipid panel
Total Cholesterol: 119
Triglyceride: 87
HDL: 35
LDL 67
The worsening markers HDL and TG in the statin panels and fingering genetics as root cause bugged me; so I started learning about macronutrients and role of insulin. I shifted paradigm. On 12/20/11 I stopped taking statin and ate LCHF (<50 grams carb per day mostly from green vegs and abstained carb-rich food, about 50 grams protein, lots of mon-unsaturated fat). I did not track caloric intake. I continued the same workout regime.
Here’s the first post-statin lipid panel:
3/17/12 post statin lipid panel
Total Cholesterol: 241
Triglyceride: 50
HDL: 60
LDL 171
Low carb gets me low TG. Eating mono-unsaturated fat and fatty meat begets higher HDL. My HDL and TG markers and ratios improved. In hindsight, I should not been alarmed by the results of Dec 17, 2010 Pre-statin lipid panel. All I had to do was to go LCHF. My bad on my ignorance and relying on my doctor’s advice. Books and blogs, such as yours, give me the knowledge and confidence to flip the conventional dogma. Oh, though not my intention, I lost about 4 pounds from 3 months of LCHF.
Peter, I’ll be writing a lot about lipids in the future, but based on the standard lipid panels you’re showing, the only thing we can even use remotely as a proxy for your insulin resistance and risk of disease is your ratio of TG to HDL-C, which went from 1.5 to 1.7 to 2.5 to 0.8. Very nice trend. Anything above 3 is pretty bad; below 1.0 is ideal. Of course, these are just indirect proxies for risk (which we can’t be assessed any further from these labs). The only thing that really matters is LDL-P, LDL particle number (vs. LDL-C, or LDL cholesterol, which is what they’re checking).
It does, however, look like you’ve improved your health a lot.
Peter,
The NYT has been leading the anti-meat crusade…now they have thrown down the gauntlet with an essay contest.
https://www.nytimes.com/2012/03/25/magazine/tell-us-why-its-ethical-to-eat-meat-a-contest.html
I am going to write a response. I’d love to read yours.
You just read mine. That’s what this blog post was!
I think they are looking more for a defense of the ethics of eating meat. I’m not sure of I can limit myself to 600 words. My parents are vegetarians, so I am sick of hearing variations of the “save the planet, animals have big brown eyes, kumbaya” hymn over and over again. I’m going to let them have it!
I’m pretty sure the New York Times contest is set up to demonstrate that in fact there is no ethical argument for eating meat. There are nutritional arguments, of course, and therein may lie the only “ethical” argument because studies have shown that when you supplement the mostly plant-based diets of kids in developing countries with a little bit of meat, they are much healthier. But for Americans with a wealth of food choices available, the crux of the question boils down to “is it ethical to take the life of an animal (one that is clearly capable of feeling pain and fear) for food when alternatives are readily available?” Peter Singer, one of the judges of the essay contest, has spent 30 years studying all the counter-arguments to his position of vegetarianism, and he studies them very deeply; he’s a gifted logician. I’m willing to bet that he will have already heard all of the arguments submitted by participants in the contest, and he will be able to demonstrate that none of them stand up to logical scrutiny.
I say all of this as an omnivore who ate beef stew last night. I don’t think our model of industrial livestock production treats animals ethically and I try to avoid eating that kind of meat as much as possible. I think the ethical line is less clear when it comes to wild game, or to livestock raised under more humane conditions, but it still boils down to the ethics of killing animals for food when we can meet our nutritional needs through plants and supplements.
My guess is that the Times contest will either produce no winners, or perhaps a winning essay that comes closest to making a convincing case, but the real purpose of the contest is to demonstrate that it is impossible to make a logical ethical case for eating meat.
I scanned the comments section, and was amazed to read – I think – that they’re mostly pro-meat. Very few hard core eating meat is murder comments. Very encouraging, especially considering this is the Times, and it’s cool to be vegan – at least in New York.
I think the ethical issue actually detracts from the scientific issue. The two issues are separate. Hope the discussion doesn’t confuse these points.
Peter,
The Ornish, Esselyn, Campbell, Willets & cohorts may be idealistic and have good intentions, but their dogma has led to this:
Today’s NY Times headline blared
‘For Diabetes, Surgery a Better Option than Standard Treatment.’
Oh, maybe it’s about treating gangrene. No, it’s bariatric stomach stapling to cure T2D, costing between $11K to $25K per operation. Has our medical establishment gone insane?
I think desperate is the better term than insane. As you say, these are not “bad” people telling us not to eat fat. They are just misled by their failure to understand what constitutes good science, and how to best interpret the bit of data out there.
Yes.
Peter, another brilliant post! Reading this renews my faith in humanity and reason. 🙂
Thanks so much, Adam. Always appreciate your support.
Peter,
This is an absolutely fascinating point of view I’ve only recently been aware of.
Recently, I was introduced to paleo.reddit.com, which today led me to the documentary “Fat Head.” Humorous documentary explaining these things you post about.
Now I’m obsessed. Researching as much as I can and posting information to social sites, bringing the danger of carbs to light.
Just wanted to thank you for what you do and I will be reading your posts as much as I can.
Jimmy Moore and I discussed your site yesterday. I think it is great and so does he, keep up the good work and let us know how to help with the Nutrition Science project
Thank you so much. Hope we can meet up at some point.
The article “Eat More Chocolate, Weigh Less?” on the WebMD site,
the (OBSERVATIONA) study in “Archives of Internal Medicine” that it’s based on,
and our tastes suggest the following question:
Is there a way to eat chocolate in an appealing way without stimulating a spike in insulin levels?
Dave, I’m glad you’re getting the hang of spotting an OBSERVATIONAL STUDY from a mile away… A very dark chocolate with little to no sugar would have a minimum insulin response. In fact, I’ve started experimenting with chocolate ice cream (zero sugar, a touch of xylitol).
Hi, Peter — I have been following (and loving) a low-carb diet after reading “Good Calories”, your blog, and Richard K. Bernstein’s books. I just saw a study posted on a calorie-restriction mail list I follow that seems to say that animal fats (SFAs) are much worse for you than PUFAs. I’d appreciate your thoughts on this if you get a chance: https://www.ncbi.nlm.nih.gov/pubmed?term=22338035
I can’t seem to get this paper for free, which I normally can with this journal. Impossible for me to comment on an abstract. Need all the details.
Rubey, I just got a copy of the paper and have skimmed it quickly (mostly because it interests me — please don’t let me set a precedent. I can’t read every paper I get sent). No time for great details, but here it is in short order: 1) All subjects consumed about 35% of their calories from carbohydrates. With carbohydrate content this high (which is obviously lower than “normal,” but not so low to even approach ketosis), the body is not yet efficiently able to prioritize fat oxidation. 2) The test meal (an all-liquid fat ingestion) still consisted of 33% carbohydrate, so whatever impact was observed, was done in the presence of at least moderate, if not high, insulin levels. 3) Virtually all of the differences (to my quick reading, at least; I have not studied this paper in my usual level of detail) seem to vanish after 2-4 hours, so it’s not clear the effect was even observed outside of that window. 4) The PUFA meal was 50% EPA and DHA, which is not even remotely a reflection of how Americans eat PUFA. Americans consume 30-50x more omega-6 than omega-3, not 1:1. I suspect much of the benefit this study saw with the PUFA meal had more to do with this feature. It would have been interesting if the PUFA meal was 95% n-6 and 5% n-6. Wonder if the result would be been the same?
Interesting study, nevertheless, despite the above limitations.
Re your comments on the SFA/PUFA study — yes, I thought the ratio of omega 3 vs. 6 for the PUFA feeding was rather odd. I wonder what they could have been thinking that led them to propose that to test.
Thanks for taking the time to look at the study and analyze.