John Kastelein is a renowned expert in lipoprotein metabolism and atherosclerotic cardiovascular disease (ASCVD) research. In this discussion, John delves deep into familial hypercholesterolemia (FH), a genetic disorder characterized by high levels of LDL cholesterol in the blood that increases the risk of developing heart disease. He covers its definition, genetic underpinnings, and clinical identification. He then explores the therapeutic options available for the prevention and treatment of cardiovascular disease, including the captivating history of CETP inhibitors. He explains the past shortcomings of previous CETP inhibitors before underscoring the compelling potential of the latest iterations, not only for cardiovascular disease but also for conditions like Alzheimer’s disease and type 2 diabetes. Moreover, he unveils the intricate role of APOE, shedding light on why the APOE4 isoform codes for a protein that significantly increases the risk of Alzheimer’s disease and cardiovascular disease. Concluding the discussion, John shares a profound sense of optimism, envisioning the possibility of targeted therapeutic interventions for high-risk patients in the near future.
Subscribe on: APPLE PODCASTS | RSS | GOOGLE | OVERCAST | STITCHER
We discuss:
- Familial hypercholesterolemia (FH): a genetic condition [4:30];
- Differentiating between phenotype and genotype when it comes to FH [9:45];
- The pathophysiology related to mutations of FH [15:30];
- Clinical presentations, physical manifestations, and diagnosis of FH [22:00];
- Criteria used to make a formal diagnosis of FH [30:15];
- Why a small fraction of people with FH do not develop premature ASCVD [34:15];
- Treatment and prevention for those with FH [39:45];
- Addressing the assertion by some that elevated LDL is not casual in cardiovascular disease [52:45];
- The history of CETP inhibitors and the role of the CETP protein [55:45];
- The thrifty gene hypothesis and why genes underlying FH may have been preserved [1:09:00];
- The compelling potential of the latest CETP inhibitor (obicetrapib) [1:13:00];
- Promising results from phase 3 trials exploring obicetrapib [1:27:45];
- Why the APOE4 allele increases the risk of Alzheimer’s disease, and the connection to blood lipids [1:41:30];
- The role of APOE in cardiovascular disease [1:51:45];
- Takeaways and looking ahead [1:57:00]; and
- More.
Familial hypercholesterolemia (FH): a genetic condition [4:30]
- This podcast came across Peter’s radar courtesy of one of his mentors, Tom Dayspring
- Cardiovascular disease is the leading cause of death globally, and Peter doesn’t think you can state the stats enough
- Last time he looked, 19 million people died in the world due to ASCVD
- The second place killer was cancer with around 12-13 million deaths (not even close)
- For this reason, Peter thinks we need to take every opportunity to educate people about this
The genetic condition familial hypercholesterolemia (FH)
- This is probably more prevalent that people realize
- Thousands of people listening to this podcast are probably affected by it
- John was the first in the Netherlands who had a large scale organization to find people with FH
- John trained in Vancouver
- He was a Visiting Professor in Vancouver by Michael Hayden
- John had his Canadian exam
- He worked in a lipid clinic in Vancouver in a time when there were hardly no lipid clinics in Europe
- When he got back to Europe and started the lipid clinic in Amsterdam, about 60% of all of his referrals were FH
- He wondered why this was so
- Holland is about the size of Rhode Island and it has 18 million people, but these people have not really moved in the past
- So there are large provinces with consanguinity, though not as much as with the French Canadians or the South Africans
- He got a huge 30 million euro grant from the Dutch government to actively find people with FH
- At the time, there was severe anterior MIs (myocardial infarction) in men between the ages of 20-30
- John can almost remember all of them
- These were people who were fit and didn’t know they had an LDL of 300 mg/dL from birth onwards
- They would be playing tennis and get a massive anterior MI
- In those days there was not much stenting yet, and you could only do vague, superficial things
- FH is a true autosomal dominant disease, meaning it’s not sex-linked
- You only need to get the gene from one parent
- It’s almost 100% penetrant meaning that if you have a robust mutation in one of the genes that cause FH, you’re almost certain to get the phenotype
- And that phenotype starts very early
- His clinic in Amsterdam is the largest pediatric lipid clinic in the world
- They have seen over 2,000 children with heterozygous FH
- This disease starts very early in life
- It becomes symptomatic in the teenage years in the sense that the cholesterol that is elevated in the circulation starts depositing on the tendons, especially the extensor tendons on the dorsum of the hand and in the achilles tendon
- Then you start very slowly seeing the arcus in the eye, and sometimes the deposits of cholesterol on the eyelids, the xanthelasma (shown below)
Cholesterol deposition in the tendons and eye/ eyelids are the two first physical manifestations of FH
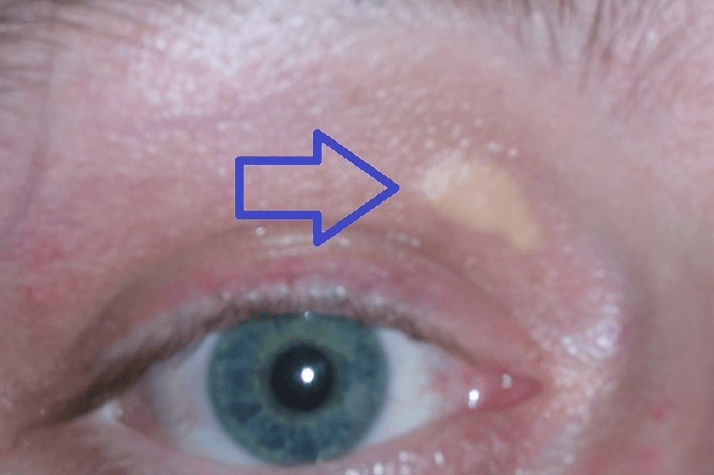
Figure 1a. Xanthelasma palpebrarum, deposits of cholesterol. Image credit: Wikipedia, FH and xanthelasma

Figure 1b. Xanthelasma palpebrarum, deposits of cholesterol. Image credit: Wikipedia, FH and xanthelasma
- Often the first really serious manifestation of FH is angina or heart attack
“One of the things that is so dangerous about this disorder is that the plaque that you get in FH is a soft plaque”‒ John Kastelein
- FH patients develop dangerous soft plaque
- It’s a cholesterol-rich large plaque that is often proximal in the arteries
- If a plaque like this bursts, you either have an occlusion of your entire LAD or you have a mainstem occlusion which kills you right on the spot
- Peter adds these are referred to as “the widow maker”
Differentiating between phenotype and genotype when it comes to FH [9:45]
Differentiate when you use the word phenotype and genotype. Explain how one defines the phenotype of FH
{end of show notes preview}
John Kastelein, M.D., Ph.D.
John Kastelein earned his doctorate in medicine (with honors) from the University of Amsterdam. He trained in internal medicine at the Academic Medical Center of the University of Amsterdam. He completed his training in lipidology and molecular biology at the University of British Columbia in Vancouver.
Dr. Kastelein is a Professor of ACS – Atherosclerosis & Ischemic Syndromes, ACS – Pulmonary Hypertension & Thrombosis, and Vascular Medicine at Amsterdam University Medical Centers where he held the Strategic Chair of Genetics of Cardiovascular disease. His research focuses on pathogenesis of atherosclerosis, lipoprotein metabolism, and treatment treatment to lower cardiovascular risk. Dr. Kastelein has published over 800 research papers in peer-reviewed journals, including Nature Genetics, Lancet, New England Journal of Medicine, JAMA, and Circulation. He has a discipline H-index of 159.
Dr. Kastelein founded the Lipid Research Clinic in 1989, which is currently serving as a tertiary referral center for over 5000 patients each year. Dr. Kastelein has served as President of the Dutch Atherosclerosis Society (DAS) and chair of the National Scientific Committee on Familial Hypercholesterolemia (EHC). He also is a member of the Royal Dutch Society for Medicine & Physics, the Council for Basic Science of the American Heart Association, the European Atherosclerosis Society, and a Fellow of the European Society of Cardiology. He is a board member of the International Task Force for CHD Prevention and served on the Executive Board of the International Atherosclerosis Society (IAS). Additionally, Dr. Kastelein has served on a number of executive and steering committees of large cardiovascular intervention studies, including the SPIRE, ORION, GLAGOV, REALIZE, IDEAL, TNT, CAPTIVATE, ENHANCE, ILLUMINATE, JUPITER, and RADIANCE. In 2010 he was awarded the prestigious Dutch Heart Association prize of 1 million euros. He was the 2014 recipient of the Anitschkow Prize by the European Atherosclerosis Society.
Dr. Kastelein is the founder and CSO of NewAmsterdam Pharma, a company developing the CETP inhibitor Obicetrapib. He is also a key advisor to a number of biotech and pharmaceutical companies, and is a member of the steering committees of numerous lipid-lowering and cardiovascular intervention trials. [NewAmsterdam Pharma]
Twitter: @JohnKastelein



Thank you for this information. I am E4/E4 and find this work fascinating and applicable! I hope you will follow up as Dr. Kastelein gathers additional data from the current trial underway. As we wait for it to unfold, is there anything in the way of diet/lifestyle or interventions of any kind that can be done to increase the circulating apoA-1? Or will this strictly be a drug intervention if results are favorable?
Thank you for this informative episode. What tests would you recommend for a male, 60-years of age, LDL Cholesterol-149mg/dL, apoe-3/4?
Best regards,
Jim
Dr. Attia and Team – I am loving all of what I am learning from your podcasts. I’m now a member, best money I’ve spent in years. Like Robyn above, I would appreciate more information on how to increase circulating apoA-1. I am an E3/E4 and until these podcasts I had been so puzzled how my healthy active father’s life was cut short by Alzheimers. I’m now eager to do what I can to support my own lifestyle and promote longevity in my family.
You always mention cardiac CTA as an important test to evaluate CAD. I cannot get my PCP or cardiologist to order this test despite having life long LDL-C of 160-200 and calcium score of 0. All say it’s not indicated without symptoms, which is so frustrating. Seems like it is such an important piece of the puzzle.
Better pictures and full scientific article on:
Why is hypercholesterolaemia so prevalent? A view from evolutionary medicine
https://academic.oup.com/eurheartj/article/40/33/2825/5086122