If I held a crystal ball 10 years ago, I’m not sure I would’ve believed it if it showed me the increased interest in the ketogenic diet would look like the figure below. That’s 2 logs, folks.
Admittedly, I started my journey on this path in 2009, with a deep dive into ketosis in the Spring of 2011, but it seemed so obscure! (For a timeline of what I did, I think I covered it somewhere in this talk…yes I’m too lazy to actually confirm this by skimming through it.) All told I spent approximately 3 years in the strictest state of nutritional ketosis (NK) with one very memorable deviation when I had 6 or 7 full-sized and upsettingly decadent desserts circa September 2013. I believe the diet helped me transition from metabolic syndrome to metabolic health and I certainly thought it could benefit other people. This nutritional state could gain some steam, I thought.
I was well aware of the dearth of mainstream knowledge of NK, and particularly the conflation of NK with diabetic ketoacidosis (DKA), a pathologic state that results from the complete or near absence of insulin, which is what prompted my writing and desire to share my journey. And I was once in the wanker category of folks who spoke with “authority” about ketosis, despite knowing somewhere between zero and nothing on the topic. I remember exactly where I was sitting in a clinic at Johns Hopkins in 2002 during my residency explaining to (admonishing, really) a patient who was on the Atkins diet how harmful it was because of DKA. Not only that, the ketogenic diet could be seen as the antithesis of a “healthy” diet by conventional standards. I could see how this was a difficult proposition for many to acknowledge.
The beautiful part of good science is its self-correcting nature. The ugly part is this self-correcting nature often moves at a glacial pace—and it’s not linear. We often view history century-by-century and see what amounts to continual progress in medicine. But we live our lives—and consume information—day-by-day, exposed to the peaks and valleys of medical wisdom.
Looking back on my earlier posts on ketosis—and explaining what I eat, for example—makes me both chuckle and cringe. I remember how bizarre the diet seemed to many readers and the general public at the time. I also remember digging into the literature and learning, for example, that my alma mater, Johns Hopkins had been using the ketogenic diet to treat pediatric epilepsy for almost a century…and being so embarrassed about admonishing that patient I saw in my residency.
Since then, it’s safe to say I dove down the rabbit hole. The more I learned, the more I grew tired of reading so much misinformation on the topic. While there are more thoughtful people and articles on the subject of ketosis these days (e.g., here’s a thoughtful video on ketosis and ketogenic diets from one of my most important ketosis mentors, Steve Phinney, a co-founder of Virta Health1Disclosure: I’m an investor in, and advisor to, Virta Health.), there are still pieces like the one Vox published this month, that doesn’t exactly do the topic justice.
Like many variables in diet, health, and disease, it behooves us to look beyond the bumper sticker explanation. I want to highlight a couple of posts I wrote, to attempt to provide a little more nuance and understanding to the subject: “Ketosis — advantaged or misunderstood state?” Parts I and II. Part I follows below. I’m hoping to write more on the topic in the not-too-distant future since there’s been a number of intriguing papers published recently (certainly since 2012). But I also wanted to bring these back into focus in light of the information I’m seeing more of on the interwebz. (You can also visit the Ketosis section of the site to view more articles on the subject.)
Because I know people will ask, I have not been on a ketogenic diet “regularly” since about mid- to late-2014. The reasons are too nuanced to describe here, but my deviation is not because I lost confidence in its efficacy. With nearly a decade of clinical experience, I can safely say I was an outlier (in the best sense) with respect to my physiology and response. I was leaner, and more mentally and physically fit during this three year period than during any other period of time as an adult, and my biomarkers were as good as they had ever been. I’ve also seen the benefit of ketogenic diets first-hand on my patients and my own sister, a remarkable story I hope to share one day. But I’ve also been humbled by my inability to explain why some people have suboptimal or even negative responses to NK. I would say, all things considered, my knowledge of ketosis is greater today than when I was writing about it voraciously, but my confidence in my understanding of it, might actually be lower. As the saying goes, the further one goes from shore, the deeper the water gets.
—P.A., April 2018
§
(Part I: originally posted November 26, 2012)
In part I of this post I will see to it (assuming you read it) that you’ll know more about ketosis than just about anyone, including your doctor or the majority of “experts” out there writing about this topic.
Before we begin, a disclaimer in order: If you want to actually understand this topic, you must invest the time and mental energy to do so. You really have to get into the details. Obviously, I love the details and probably read 5 or 6 scientific papers every week on this topic (and others). I don’t expect the casual reader to want to do this, and I view it as my role to synthesize this information and present it to you. But this is not a bumper-sticker issue. I know it’s trendy to make blanket statements – ketosis is “unnatural,” for example, or ketosis is “superior” – but such statements mean nothing if you don’t understand the biochemistry and evolution of our species. So, let’s agree to let the unsubstantiated statements and bumper stickers reside in the world of political debates and opinion-based discussions. For this reason, I’ve deliberately broken this post down and only included this content (i.e., background) for Part I.
What is ketosis?
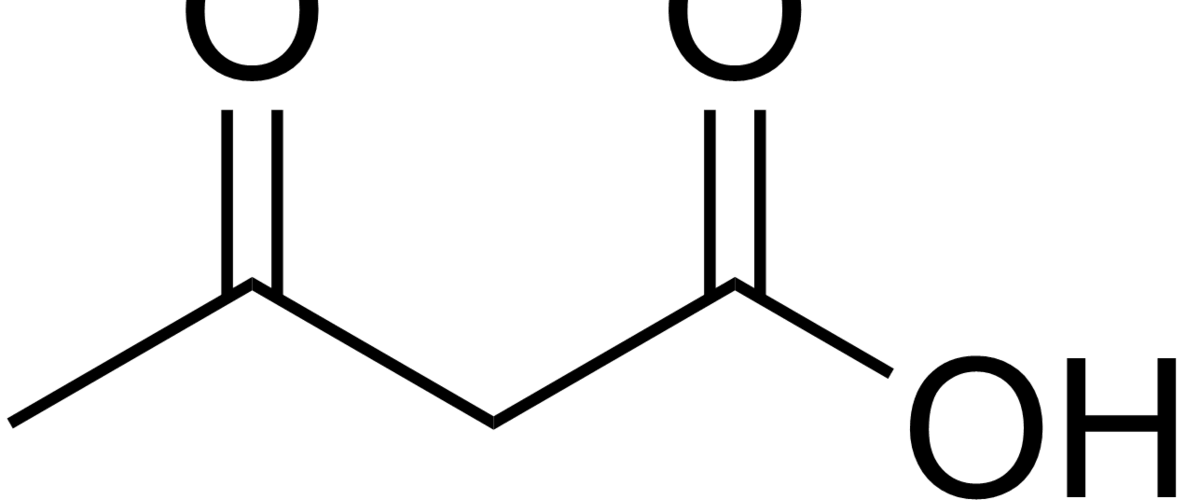
Ketosis is a metabolic state in which the liver produces small organic molecules called ketone bodies at “sufficient” levels, which I’ll expand upon later. First, let’s get the semantics correct. The first confusing thing about ketosis is that ketone bodies are not all – technically — ketones, whose structure is shown below. Technically, the term ketone denotes an organic molecule where a carbon atom, sandwiched between 2 other carbon atoms (denoted by R and R’), is double-bonded to an oxygen atom.

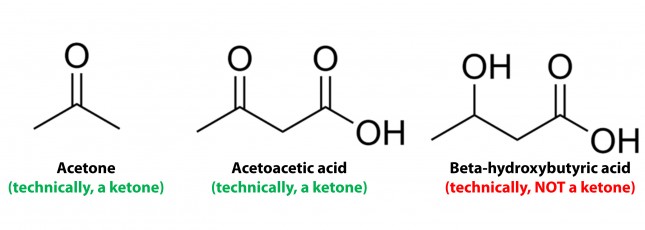
Conversely, the term “ketone bodies” refers to 3 very specific molecules: acetone, acetoacetone (or acetoacetic acid), and beta-hydroxybutyrate (or beta-hydroxybutyric acid), shown below, of which only 2 are technically ketones. (The reason beta-hydroxybutyrate, or B-OHB, is not technically a ketone is that the carbon double-bonded to the oxygen is bonded to an –OH group on one side, technically making B-OHB a carboxylic acid for anyone keeping score.)
Now, back to the real question at hand. Why would our body make these substances? To understand why or when the body would do this requires some understanding of how the body converts stored energy (the food we eat or the energy we store in our body, i.e., fat or glycogen) into phosphate donors. For a refresher on this process, please refer to the video in this post, specifically the section from 2:15 to 13:30.
The ATP issue
As you may recall, about 60% of the energy we expend, say 1,800 kcal/day for someone consuming 3,000 kcal/day in weight balance, is purely devoted to keeping us alive by generating enough ATP (“energy currency”) to do 2 things: allow ion gradients to function and allow muscular relaxation. So, obviously, we can’t tolerate – literally even for one minute – insufficient ATP production. In fact, one of the most potent toxins known to man (cyanide) exerts its effect on this process by inhibiting the electron transport chain which generates the bulk of the ATP our body produces. Even the most transient interruption of this process is fatal.
Take home message #1: No ATP, even for 1 minute, equals no life.
The brain issue
The brain is a particularly greedy organ when it comes to energy requirement. To put this comment in perspective consider the following: though our brain represents only about 2% of our body mass, it accounts for about 20% of our energy expenditure. (In children, by the way, this may be closer to 40-50% of basal metabolic demand.) So, beyond the ATP issue, above, there is a substrate issue with the brain as neurons derive most of their energy from glucose. While there is emerging evidence that neurons can also oxidize fatty acids directly in small amounts and may even prefer lactate (over glucose), these two substrates do not approach the levels of consumption by neurons that glucose does. So, for the purpose of this discussion, let’s just focus on the need of the body to provide glucose to the brain.
You’ll recall, from the point I made above, that my brain requires about 400 to 500 kcal of glucose per day (100 to 120 gm). You’ll also recall (from the video, above) that I can store about 100 to 120 gm of glucose in my liver. While I can store much more in my muscles, (on the order of about 300 to 350 gm), because muscles lack the enzyme glucose-6-phosphatase, glucose stored in muscle as glycogen is unable to re-enter the bloodstream and is meant for the muscle and the muscle alone to use. In other words, muscle glycogen is a stranded asset of glucose in the body to be used only by the muscle.
So, if I’m deprived of a dietary source of glucose, I depend solely on my liver to release glycogen (a process known as hepatic glucose output, or HGO). How long can HGO supply my brain with sufficient glucose? It depends on a few things that impact both the “source” and the “sink” of glucose. Other competing sinks for glucose (e.g., activity level, thermogenic needs) and sources (e.g., glycerol and gluconeogenic amino acid availability) can make a difference for a while. But, in a state of starvation we’ve only got about one to three days before we’re in trouble. If our brain doesn’t get a hold of something else, besides glucose, we will die quite unceremoniously.
Take home message #2: No glucose for 24-72 hours equals the need for something else the brain can use instead (that is not fat or protein, since neurons can’t oxidize fat and the last thing we want to do is start muscle wasting at a geometric rate).
The Krebs Cycle
This poses a real evolutionary dilemma. We need an enormous amount of energy just to not die, but the single most important organ in our body (also quite energy hungry in its own right) can’t access the most abundant source of energy in our body (i.e., fat) and is, instead, almost solely dependent on the one macronutrient we can’t store beyond a trivial amount (i.e., glucose). Obviously our species wouldn’t be here today if this were the end of the story. But, to understand how we survived requires one more trip down biochemistry memory lane. In the figure below (also included and described in the video) I gloss over a pretty important detail.
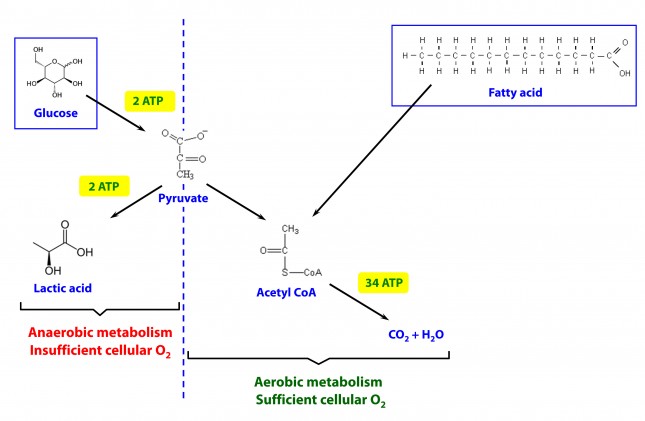
How, exactly, does our body take pyruvate (from glucose) or acetyl CoA (from fat) and generate so much ATP? The answer lies in the beauty of the Krebs Cycle, which feeds into a process called the electron transport chain (or ETC), I alluded to above. Since the adage ‘you can’t get something for nothing’ is as true in biochemistry as it appears to be in life, to get all that ATP (i.e., stored energy in the form of the phosphate bond), we need to give up something. What the ETC does give up, as its name suggests, is electrons. Through a series of redox reactions the ETC trades the stored energy held by electrons going from higher to lower energy states in exchange for the chemical energy stored in the bonds of the third phosphate group on an ATP molecule.
To think of it another way, if you start with stored energy – glucose or fat, for example, which if burned in calorimeter will give off varying amounts of heat – and you’re willing to convert their carbon, hydrogen, and oxygen molecules into another form with less energy – water and carbon dioxide which, if burned, produce very little heat – it’s a fair trade! The ETC is simply the vehicle that allows our body to make the switch.
In a car, by contrast, it’s much simpler. The engine combusts the hydrocarbon (e.g., gasoline) directly and in one flash liberates the heat contained within the hydrogen-carbon and carbon-carbon bonds in exchange for carbon dioxide, water vapor, and a few other things.
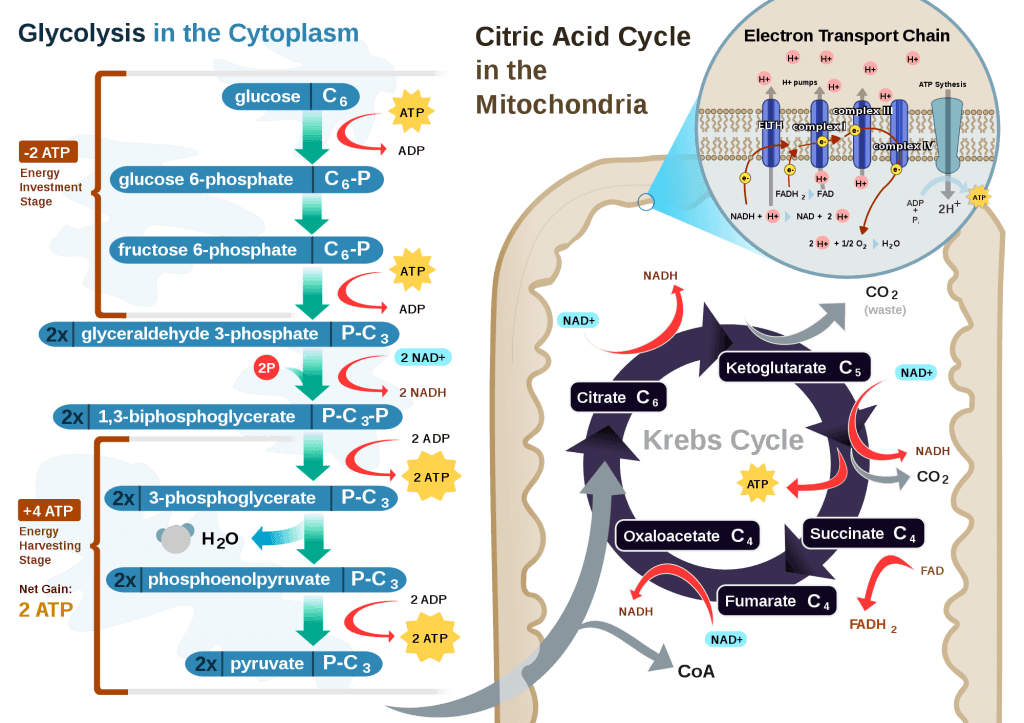
If you take a look at the figure, below, you’ll get a sense of the moving pieces involved in this cyclic transfer process. Molecules shuffle back and forth, around the cycle, and kick off spent carbon (carbon dioxide, termed “waste”) and reducing agents (e.g., conversion from NAD+ to NADH) for the ETC.
Where do the ketones come in?
In the absence of acetyl CoA (several ways this can happen, including substrate shortage, as I’m describing here) we evolved a cool trick. Our liver can make – out of fat or protein, though we much prefer to use fat so we can spare our protein and prevent severe muscle wasting – something called beta-hydroxybutyrate, one of the 3 ketone bodies I described above.
B-OHB and acetoacetate (see figure below from this paper by Cahill and Veech, 2003) are produced by the liver from long and medium chain fatty acids and released into the bloodstream.
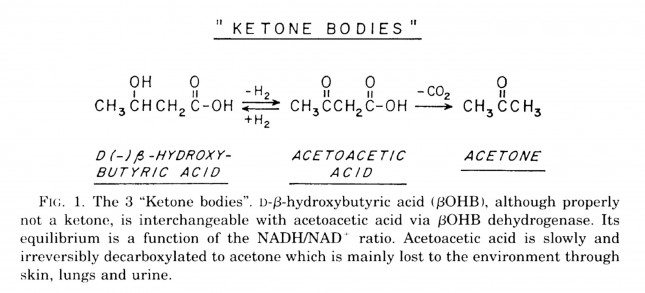
Acetoacetic acid and B-OHB live in reversible equilibrium (on the left), but once acetoacetate is converted to acetone (on the right) there’s no going back.
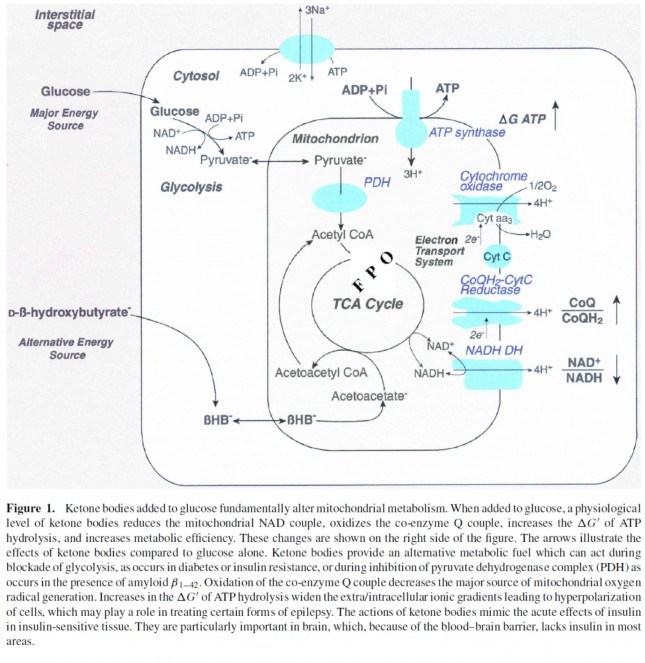
Now take a look at the figure below, from this 2001 paper. This is another rendition of the figure above showing the Krebs Cycle, but here you can see where B-OHB and acetoacetate enter the picture.
The reason a starving person can live for 40-60 days is precisely because we can turn fat into ketones and convert ketones into substrate for the Krebs Cycle in the mitochondria of our neurons. In fact, the more fat you have on your body, the longer you can survive. As an example of this, you may want to read this remarkable case report of a 382 day medically supervised fast (with only water and electrolytes)! If we had to rely on glucose, we’d die in a few days. If we could only rely on protein, we’d live a few more days but become completely debilitated with muscle wasting.
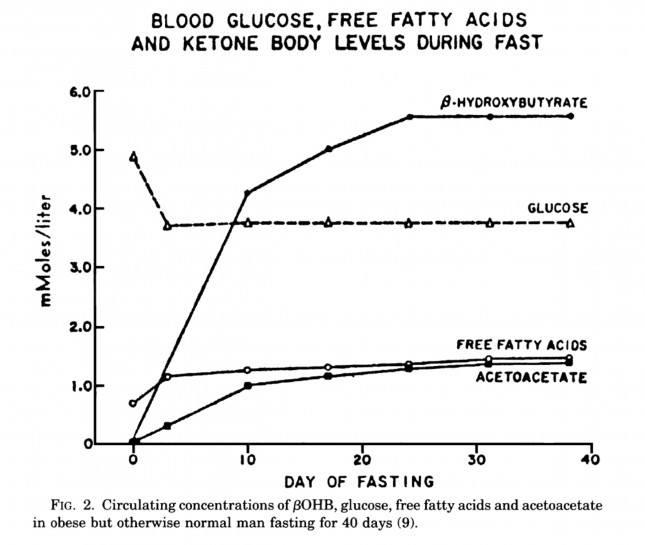
The graph below, also from the Cahill and Veech paper, shows the blood chemistry of a person starving for 40 days. Within about 3 days, a starving person’s level of glucose stops falling. Within about 10 days they reach a steady-state equilibrium with B-OHB levels exceeding glucose levels and offsetting most of the brain’s need for glucose. In fact, the late George Cahill did an experiment many years ago (probably would never get IRB approval to do such an experiment today) to demonstrate how ketones can offset glucose in the brain. Subjects with very high levels of B-OHB (about 5-7 mM) were injected with insulin until glucose levels reached 1 mM (about 19 mg/dL)! A normal person would fall into a coma at glucose levels below about 40 mg/dL and die by the time blood glucose reached 1 mM. These subjects were completely asymptomatic and 100% neurologically functional.
The last point I’ll make on the starving patient is that, as you can see in the figure below, the glucose level normalizes at about 65-70 mg/dL (about 3.7 mM) within days of fasting, despite no sources of exogenous glucose. Why? Because with so much fat being converted into B-OHB and acetoacetic acid by the liver, a significant amount of glycerol (the 3-carbon backbone of triglycerides) is liberated and converted by the liver into glycogen. As an aside, this is why someone in nutritional ketosis – even if eating zero carbohydrates – still has about 50-70% of a normal glycogen level, as demonstrated by muscle biopsies in such subjects.
Take home message #3: We evolved to produce ketone bodies so we could not only tolerate but also thrive in the absence of glucose for prolonged periods of time. No ability to produce ketone bodies = no human species.
Last point of background: Everything I’ve just presented is based on data from starving subjects. If one restricts carbohydrate intake, typically to less than about 20-50 gm/day (dependent on timing and carbohydrate composition), and maintains modest but not high protein intake (because protein is gluconeogenic – i.e., protein in excess will be converted to glycogen by the liver), one can induce a state referred to as “nutritional ketosis” with similar physiology to what I’ve just presented without resorting to starvation. Why you’d do this is something I will discuss later.
One other housekeeping issue: Ketosis versus DKA?
In a separate post, I explained the difference between nutritional ketosis (NK) and diabetic ketoacidosis (DKA). If this distinction is not clear, I’d suggest giving this separate post a quick skim for a refresher. DKA is a pathologic (i.e., harmful) state that results from the complete or near absence of insulin. This occurs in the setting of type 1 diabetes or very end-stage type 2 diabetes, and often as the result of a physiologic insult (e.g., an infection) where the patient is not receiving sufficient insulin to bring glucose into his cells. A person with a normal pancreas, regardless of how long he fasts (including the fellow I reference above who fasted for 382 days!) or how much he restricts carbohydrates, can not enter DKA because even a trace amount of insulin will keep B-OHB levels below about 7 or 8 mM, well below the threshold to develop the pathologic acid-base abnormalities associated with DKA. Let me reiterate, it is physiologically impossible to induce DKA in anyone that does not have T1D or very, very, very late-stage T2D with pancreatic “burnout.”
Embarrassing admission: I remember exactly where I was sitting in a clinic at Johns Hopkins in 2002 explaining to (admonishing, really) a patient who was on the Atkins diet how harmful it was because of DKA. I am so embarrassed by my complete stupidity and utter failure to pick up a single scientific article to fact check this dogma I was spewing to this poor patient. If you’re reading this, sir, please forgive me. You deserved a smarter doctor.
In Part II of this post I’ll tackle the questions I know folks still have on their mind (below). Until then, re-read this post to make sure you really understand this physiology. You’re already 10 steps ahead of the next person.
- Is there a “metabolic advantage” to being in ketosis?
- Are there dangers of being in ketosis?
- What are the most important things you need to know about getting into (or staying in) ketosis?

{kind=link}
Peter,
Thank you for this posting. I wish I had your clarity of thinking and writing as you always seem to manage to make dense topics more accessible.
Over the past year (a year? wow) I have learned more from you, rereading Gary’s book, and devouring the Art and Science of Low Carbohydrate living than in all the years I studied nutrition to the point I could have passed the exams to be a registered dietitian.
One of the best things I like about your blog is the fact that in your writing you don’t force a certain way of eating. You said you were amazed that ‘what I eat’ is the most read blog. That does not surprise me as so many of us act like ‘educated lemmings’ (I include myself in that since I can just imagine I just insulted many people including myself) and want someone to tell us what to eat. You refuse to do that. You ask that we devise an eating pattern that works for our individual bodies based on current understanding of nutrition not blindly follow someone else’s meal plan.
I hope someday that the kind of testing you have discussed in many of your replies and postings becomes the norm. Right now I cannot have many of the tests you describe because my doctor sees no need for them and refuses to sign the form for them. He once told me that one test I asked for had no valid use yet I read here that it can be useful. I do not have the funds to get testing done privately. Furthermore, he does not understand nutritional issues and falls back on the standard low fat, eat miniscule diet rules. And no, I cannot change doctors. The current health plan I am under makes that difficult. So I fall back on my current studies and hope that I am doing the right thing for my body.
Again, Peter, thank you for this posting and for all your hard work as you come up on your anniversary. And a thank you to your wife for allowing you to spend so much time with all of us.
Understood. Hang in there.
Dr. Attia, Thank you for the explanation of ketosis and the ketogenic diet.
Ketogenic dieting is effective because it reduces circulating glucose while reducing glycation. These are effects of a widespread western problem, insulin resistance. Ketogenic dieting, however, does little to address insulin resistance, the cause of circulating glucose and glycation. Insulin resistance is caused by insulin mimetic proteins, like WGA in wheat and concavalin A in legumes. These proteins enter the circulatory system because they set up an innate immune reaction in the small intestine. The reaction causes the intestinal walls to become porous.
Limiting sugars helps treat the problem, but eliminating harmful carb-related proteins cures the problem.
Interesting. But on the topic of WGA, I believe practically all of it is destroyed by heating, is it not? Certainly other proteins survive the heating process, but not that one (if i recall correctly). So if some proteins cause the porousness (like zonulin release due to gluten, etc.), what proteins are the actual insulin mimetics? Could the cause be LPS activity by gram-negative bacteria causing the porousness/immune reaction, or is that secondary to the types of proteins you mention?
Actually my post was overly simplistic for a rigorous analysis. The food peptides which mimic insulin in the bloodstream are not necessarily the peptides which cause the zonulin dump in the small intestine. They come from other associated peptide sequences, such as the sequences in hyphal wall protein 1 (HWP1), from the same foods. And yes, there is evidence that, for many people, the bacteria and fungi which colonize around these proteins can initiate the zonulin dump. They would probably be associated with interim steps using oligosaccharides and glutamates to prepare the intestinal epithelium.
There is experimental evidence that in a vacuum WGA is degraded by heat. There is also experimental evidence that it is not degraded in vivo …..in real world situations. There is strong evidence associating ingested WGA with other non-insulin mimetic bloodstream effects, like cartilage degradation and red blood cell clumping. So I’m saying no, in vivo a huge amount of WGA gets into the bloodstream when we ingest wheat.
Excellent information, as always! I’ll look forward to part II of the series. This should be a valuable resource to pass along to all of the people that give me a “You’re on a what kind of diet?”.
Great post again Peter. Ketosis content aside I particularly enjoy the humbleness of your “embarrasing admission”. We’ll very likely make more mistakes and instead of hiding them let’s be transparent.
Thanks again and regards from Norway!
I am experimenting with ketosis myself and find it an interesting journey. How do you find it feels mentally?
Also today I see that some contrary points have been posted by Arthur Devaney saying that fat in the diet encourages inflammation. https://artdevanyonline.com/1/post/2012/12/those-high-fat-paleo-diets.html
This has me wondering about it all. Is the overall “loading” of the liver from fat or carbohydrates going to have an effect on us over time?
peter,
Diagnosed with T2 DM in 2010, and on low carb diet since then, T2 completely reversed. But every time I got into ketosis (less than 30 carbs), I got heart palpitation, especially after a meal. Any idea how to work around the problem ?
Thanks!
Kang
A number of things are possible, but you should certainly have your doctor confirm that you are not low in potassium, which is a common side effect of ketogenic diets if not supplementing sodium and magnesium.
Thank you Dr. Attia. Very informative. My wife is a PhD in neuroscience and she is enjoying the reading a lot! Looking forward to read part 2, particularly for the aspect of the cori cycle.
Thanks again!
Sam
@melancholy aeon
“Why not talk to any of the several women we all know who in fact have done this?”
“There are some quite prominent low-carb moms around and I suggest you talk to them. Best wishes.”
Did I miss a low-carb parent meet n’ greet or something? I was recently put in contact with Dr. Wortman but I don’t know any others. Feel free to introduce me. 🙂
Dave
Hi Dr. Attia,
After reading your blog I changed my diet and feel great. I am not in ketosis. I thought many times if I should try to get into it by further lowering my carb intake. One thing bothers me a little is I remember somewhere I read that ketonbody is produced by the liver and can be used by all organs except the liver. I wonder where does the liver get its nutrient if one is in ketosis for the long term. Will it have any negative impact on the liver at all? Thanks.
B-OHB production by the liver does not harm it.
I’ve read through quite a few pages on this site but one question I have is;
How much daily fat is too much for the heart? I have a high metabolism and I’m struggling to maintain my current weight. I realize most people go on keto to lose weight, but I went on because sugar-free improves my skin condition (rosacea)
I’m not sure what dietary fat has to do with the heart.
Hi Peter, would you have any input on the standard recommendation (HDL Labs) for a person with Apo 3/4 to go on a very low fat diet? Thank you very much, maryann
It’s not clear to me that is based on great data. If anything, it may be polymorphisms in apoA-II that could (?) determine dietary fat sensitivity. The defect with apoE 4 (3/4 or 4/4) is one of the LDL receptor. Such patients, to varying degrees, have more difficulty clearing LDL-P from circulation.
Peter, I’m glad you’re doing this series, and am looking forward to future posts. One thing that seems unclear to me is the frequently-expressed idea of “going in and out of ketosis” — kind of like turning a switch on and off, or going through a swinging door. Is it really like that; or is it a more gradual shifting of things? What exactly happens in that transition?
It’s actually pretty quick, assuming you ingest a food that results in much insulin secretion.
Love this blog Dr. Attia, very interesting, and extremely informative even for those not previously educated in these areas (albeit I do find some of the biochemistry a bit confusing haha). I am very interested in nutrition and biology, as well as fitness, even more so because my girlfriend has PCOS, and a family member was recently diagnosed with type 2 diabetes. I believe myself to be someone genetically predisposed to insulin sensitivity or having a higher portion of LPL on muscle tissue, like you have described your wife. Similarly no matter what or how much I eat, I just don’t seem to gain much weight at all (very slight subcutaneous fat is all), albeit I am only 22 and I assume I could still develop an insulin resistance if I ate in a certain manner (I don’t know).
You say you have cured your insulin resistance from your dietary changes based on the tests you took. Strictly out of curiosity, I wonder what would happen (hypothetically speaking) if you changed back to your diet before making any changes, given the fact that you are very insulin sensitive now. I assume your insulin resistance developed over time based on the fact that you were in such great shape in high school. How long do you think it would take to get back to the insulin resistance you had before beginning your journey? I assume a can of soda would be far less detrimental to you now, as opposed to before?
Professional fitness models have a methodical practice when preparing for a competition or photo shoot, and over time they develop a vast knowledge for what affects their body composition. One thing they always do is perform a significant amount of cardio through low-moderate intensity aerobic exercise, in the belief that they are burning fat. Given your hypothesis and personal experience, you believe this is actually having little to no beneficial effect on their body’s fat content? They do carb-restrict also of course, so you believe that the only real fat loss they are seeing is through their carbohydrate restriction?
Great question. The recent blog post of Mike Eades suggests I may even gain back more weight than I lost with enough time…
very cool of you to admit that you didn’t give your patient the right advice way back when. Congratulations on being an open minded clinician!!! We need more people like you to take care of patients. It is not easy to admit that you could have been wrong. 🙂
Cool, but sad… If you make as many mistakes I have do/have, you have lots of practice admitting it.
My doctor was horrified when I told him about my low carb/high fat diet and along with the usual arguements against it, he said it exacerbated Panic Disorder, a complicated biological condition. He was mum when I asked him how, but have you heard this previously?
Also, after being practically chased out of a Health Food store after asking if they had a low-carb section, I went to my local Trader Joe’s, where I feasted on their wonderful Almond Butter. At checkout, they had a dark chocolate bar which had 0g of Sugars listed, but had 13g of carbs listed. Then it said that it only had 2g of “effective carbs”, but it had only 1g fiber content. What are effective carbs, and should I buy this next time?
TIA
EC is the difference between total carb, sugar, and alcohol sugar (where present). TJ’s AB is great.
Hi Stephen,
From my own personal experience I’ve tried the panic disorder. My own explanation to this is mineral deficiency (especially magnesium). I don’t know if you have actually had attacks of panic disorder but I can assure that what I’ve tried is something you want to avoid. I would assume your doctor’s concern goes back to that he knows that a low carb/high fat diet could potentially leave you deficient in those minerals.
Hi Peter ,
For me it is all about the potassium entering the muscle cells by insulin.
Once the potassium is in there the faulty channels do not repolarize and my muscles paralyse.
The condition is hypo kaleamic periodic paralysis.
It is genetic.Treatment is with acetazolamide and potassium supplements and avoidance of triggers.
Triggers can be exercise, environmental temperatures, hormones ,sodium and many things but mostly it is to do with carbohydrates or long gaps between meals.
The liver releasing glycogen stimulates insulin ,right?
I have found I get fewer attacks on approx 15 g of carbs / 24 hrs. I have been doing this for about 18 months.my BMI is at a steady 20, similar to what it used to be when I ate carbs.However,my exercise tolerance is still very limited,peior to this condition kicking in I used to run marathons.
Does having too much protein cause glycogen and thus insulin to be released?
What is your vie on the insulin index, scares me that beef is so high and considering cutting out dairy altogether
My husband eats Paleo and although I like peanut butter now that I know about the omega3 vs omega6 ratios I may limit my intake.We use coconut oil,great stuff.
Do you think being ketogenic should help prevent the potassium influx into the muscles?
Thank you for your thoughts.
Malin
peter, will you take on this challenge?
https://www.youtube.com/watch?v=AfgRQzArvb0
I have absolutely nothing against the high fruit eaters in this world. In my view, the diet that works for you, makes you happy and perform the way you like is fine with me. However, am I the only one that realizes a low fat, high fruit diet is indirectly a high fat, low protein diet?
Correct me if I’m wrong, but my understanding is that excess fructose beyond what is stored as glycogen is converted by the liver into triglyceride. Since fructose doesn’t have a dramatic insulin response and high fruit eaters aren’t eating many sugars or aminos acids that directly stimulate insulin secretion, these triglycerides are readily available to be used for energy should the need be present. So in other words, providing that they adhere strictly to their diet, they maintain access to their fat stores in a similar fashion as would a low carb, high fat individual. But, they are forced to keep protein low, dietary fat low and make sure they don’t add in much glucose because any one of these could bring about the adverse effects of excess fructose ie. fatty liver and everything that follows
I personally follow a low carb, high fat diet because its just flat out easier to live with, and in my view (possibly others as well) a more efficient means of reaching a similar (dare I say superior) metabolic flexibility, while allowing the inclusion of more protein to support muscle growth.
There is a tremendous misunderstanding of the metabolism of fructose vs. fructose + glucose. The topic was done no favors by the “famous” Hellerstein paper from ’98 or ’99 looking at de novo lipogensis (DNL). Flawed methodology grossly underestimated DNL. The revised version of this paper (“A Dual Sugar Challenge Test for Lipogenic Sensitivity to Dietary Fructose” — J Clin Endocrinol Metab 96: 861–868, 2011) is actually the correct one. For those interested in this topic, who can’t wait until I write about in detail, get the paper and go straight to figure 5). Simply astonishing.
Hey Peter
Great article.
I am big fan of the Danish version of rye bread, being that I am Danish 🙂
I bake my own version of this bread with the following ingredients, it`s delicious.
Sunflower seeds, Pumpkin Seeds, Sesame seeds, Flax seed, Almonds, Walnuts, Eggs, Olive oil, Salt
This bread is really high in fat but also contains some carbs, so my question is. Will this bread eaten in moderation effect ketosis?
One way to find out.
Dr. Attia,
Just found this paper from 2010 online: Diet-dependent acid load, Paleolithic nutrition, and evolutionary health promotion (https://ajcn.nutrition.org/content/91/2/295.full) and here is an interesting paragraph:
“The striking prevalence of osteoporosis in Inuit skeletal remains from the early contact period (8) is especially pertinent to the observations of Ströhle et al (1) because plant foods are necessarily scarce in circumpolar environments. In East Africa, late Paleolithic plant-to-animal energy intake ratios would have approximated 50:50, and diet-dependent net endogenous acid production (NEAP) would have been alkaline—the norm for human biochemistry, physiology, and bone health. In contrast, for traditional Inuit HGs, whose subsistence derived overwhelmingly from aquatic and animal sources, NEAP would have been acidic, contributing to their osteoporosis.”
It seems that while ketosis might be man’s natural state, plant base food have to be more abundant (close to a 50:50 ration) which would also reduce the need for suplementation.
Sam
Interesting, but probably worthy of more comment than I can provide at the moment.
Dr. Attia,
I sent my comments to a friend of mine who is in med school and reads your blogs and here is his take on it:
“As for the article, I’m gonna play devil’s advocate here: I definitely think eating enough vegetables is necessary. However, the article does make a jump in assuming that it was the NEAP that caused the osteoporosis. There are too many variables to do so, and it seems to be a bit oversimplified.. It could also be that there food supply variety is quite limited compared to someone from say east Africa where they had access to necessary vitamins found in the the wider array of foods consumed, both plant and animal sources alike (not to mention fungi). Besides this what about effects on the bones from living in limited light while usually completed covered and the subsequent possible effects from vitamin D depletion (although they could find ample supplies in foods like cod liver)? A person in Africa would have no problem with synthesizing endogenous vitamin D, while that of someone in polar latitudes would have to supplement through diet.
Now in terms of the diet… the protein consumption of someone going low carb should not be more than that the typical diet. Fat should replace the carbs. Not protein. Increased protein intake has been associated with an array of metabolic issues and has even been implicated in longevity studies. One study set out to test the hypothesis that reduced caloric intake correlated with increased longevity. Turned out that there was no correlation (although people still claim this). What they did find was that was an inverse relationship between protein intake and longevity, assuming one was consuming baseline protein levels.
Lastly, ketosis does not actually change the blood pH by any significant level. This is not to be confused with diabetic ketoacidosis which will result in a drop. The blood of someone in dietary ketosis stays very much in alkaline range. If levels fall too low in a non-diabetic individual, insulin is released and will then prevent any more fat mobilization. Fat will not longer be burned (instead stored) and pH will return within physiological limits. So all of that said, a keto diet should not result in significant drop in blood pH. The body will be sure to maintain homeostasis within proper pH range, assuming one’s pancreas functions normally.
There are probably other factors at work in regards to northern latitude osteoporosis. Today we know better. Anyone living north of Virginia should be taking ~2000IU of Vit D a day. Some say that even this is too low. There are also other factors that could be at play such as manganese intake, genetic predisposition, the methods of sampling used by the researchers quoted in the study (done back in 1966), work conditions, etc. Point being, there are just too many other variables at work for the other of the paper to state that is a result of NEAP.
Regardless, I would be sure to get adequate intake of veggies while keeping protein intake within normal ranges. Excessive protein could lead to a slew of problems along with increasing your insulin levels which could kick you out of ketosis. ”
Sounds like an Attia Jr., doesn’t he? 🙂
By the way, he told me that he learned more from your blogs on cholesterol than in his med school lipids class!!
Final question, after 3 weeks I am still going through the keto flu and want to get out of this limbo asap. Is there any of your blogs that adresses this particular issue of keto adaptation?
Thank you!!!
Sammy
Sammy, in case of “flu” I usually do the following:
1. Document I’m actually “in” ketosis (B-OHB consistently over 0.5 mM, and ideally over about 1.0 mM)
2. If the above is true, protein levels are usually not excessive
3. Ensure adequate sodium (easy via bouillon) and magnesium.
See other comments for details on the above.
Thank you for finding this! Exactly! 50/50 ratio (or a tad more carbo to prevent ketosis). See my comments on Dr. Sears and Zone above.
This is the best health related blog out there by far! What’s the ETA on part II? I’m chomping at the bit for more info
Hopefully within 2 weeks. It takes about 20 hours to write one of these posts.
Cool, I will wait patiently. I hope you know that your efforts are not only greatly appreciated, but noble. We need more people like you in this world to save us from the havoc created by the last fifty years of junk nutritional advice.