If I held a crystal ball 10 years ago, I’m not sure I would’ve believed it if it showed me the increased interest in the ketogenic diet would look like the figure below. That’s 2 logs, folks.
Admittedly, I started my journey on this path in 2009, with a deep dive into ketosis in the Spring of 2011, but it seemed so obscure! (For a timeline of what I did, I think I covered it somewhere in this talk…yes I’m too lazy to actually confirm this by skimming through it.) All told I spent approximately 3 years in the strictest state of nutritional ketosis (NK) with one very memorable deviation when I had 6 or 7 full-sized and upsettingly decadent desserts circa September 2013. I believe the diet helped me transition from metabolic syndrome to metabolic health and I certainly thought it could benefit other people. This nutritional state could gain some steam, I thought.
I was well aware of the dearth of mainstream knowledge of NK, and particularly the conflation of NK with diabetic ketoacidosis (DKA), a pathologic state that results from the complete or near absence of insulin, which is what prompted my writing and desire to share my journey. And I was once in the wanker category of folks who spoke with “authority” about ketosis, despite knowing somewhere between zero and nothing on the topic. I remember exactly where I was sitting in a clinic at Johns Hopkins in 2002 during my residency explaining to (admonishing, really) a patient who was on the Atkins diet how harmful it was because of DKA. Not only that, the ketogenic diet could be seen as the antithesis of a “healthy” diet by conventional standards. I could see how this was a difficult proposition for many to acknowledge.
The beautiful part of good science is its self-correcting nature. The ugly part is this self-correcting nature often moves at a glacial pace—and it’s not linear. We often view history century-by-century and see what amounts to continual progress in medicine. But we live our lives—and consume information—day-by-day, exposed to the peaks and valleys of medical wisdom.
Looking back on my earlier posts on ketosis—and explaining what I eat, for example—makes me both chuckle and cringe. I remember how bizarre the diet seemed to many readers and the general public at the time. I also remember digging into the literature and learning, for example, that my alma mater, Johns Hopkins had been using the ketogenic diet to treat pediatric epilepsy for almost a century…and being so embarrassed about admonishing that patient I saw in my residency.
Since then, it’s safe to say I dove down the rabbit hole. The more I learned, the more I grew tired of reading so much misinformation on the topic. While there are more thoughtful people and articles on the subject of ketosis these days (e.g., here’s a thoughtful video on ketosis and ketogenic diets from one of my most important ketosis mentors, Steve Phinney, a co-founder of Virta Health1Disclosure: I’m an investor in, and advisor to, Virta Health.), there are still pieces like the one Vox published this month, that doesn’t exactly do the topic justice.
Like many variables in diet, health, and disease, it behooves us to look beyond the bumper sticker explanation. I want to highlight a couple of posts I wrote, to attempt to provide a little more nuance and understanding to the subject: “Ketosis — advantaged or misunderstood state?” Parts I and II. Part I follows below. I’m hoping to write more on the topic in the not-too-distant future since there’s been a number of intriguing papers published recently (certainly since 2012). But I also wanted to bring these back into focus in light of the information I’m seeing more of on the interwebz. (You can also visit the Ketosis section of the site to view more articles on the subject.)
Because I know people will ask, I have not been on a ketogenic diet “regularly” since about mid- to late-2014. The reasons are too nuanced to describe here, but my deviation is not because I lost confidence in its efficacy. With nearly a decade of clinical experience, I can safely say I was an outlier (in the best sense) with respect to my physiology and response. I was leaner, and more mentally and physically fit during this three year period than during any other period of time as an adult, and my biomarkers were as good as they had ever been. I’ve also seen the benefit of ketogenic diets first-hand on my patients and my own sister, a remarkable story I hope to share one day. But I’ve also been humbled by my inability to explain why some people have suboptimal or even negative responses to NK. I would say, all things considered, my knowledge of ketosis is greater today than when I was writing about it voraciously, but my confidence in my understanding of it, might actually be lower. As the saying goes, the further one goes from shore, the deeper the water gets.
—P.A., April 2018
§
(Part I: originally posted November 26, 2012)
In part I of this post I will see to it (assuming you read it) that you’ll know more about ketosis than just about anyone, including your doctor or the majority of “experts” out there writing about this topic.
Before we begin, a disclaimer in order: If you want to actually understand this topic, you must invest the time and mental energy to do so. You really have to get into the details. Obviously, I love the details and probably read 5 or 6 scientific papers every week on this topic (and others). I don’t expect the casual reader to want to do this, and I view it as my role to synthesize this information and present it to you. But this is not a bumper-sticker issue. I know it’s trendy to make blanket statements – ketosis is “unnatural,” for example, or ketosis is “superior” – but such statements mean nothing if you don’t understand the biochemistry and evolution of our species. So, let’s agree to let the unsubstantiated statements and bumper stickers reside in the world of political debates and opinion-based discussions. For this reason, I’ve deliberately broken this post down and only included this content (i.e., background) for Part I.
What is ketosis?
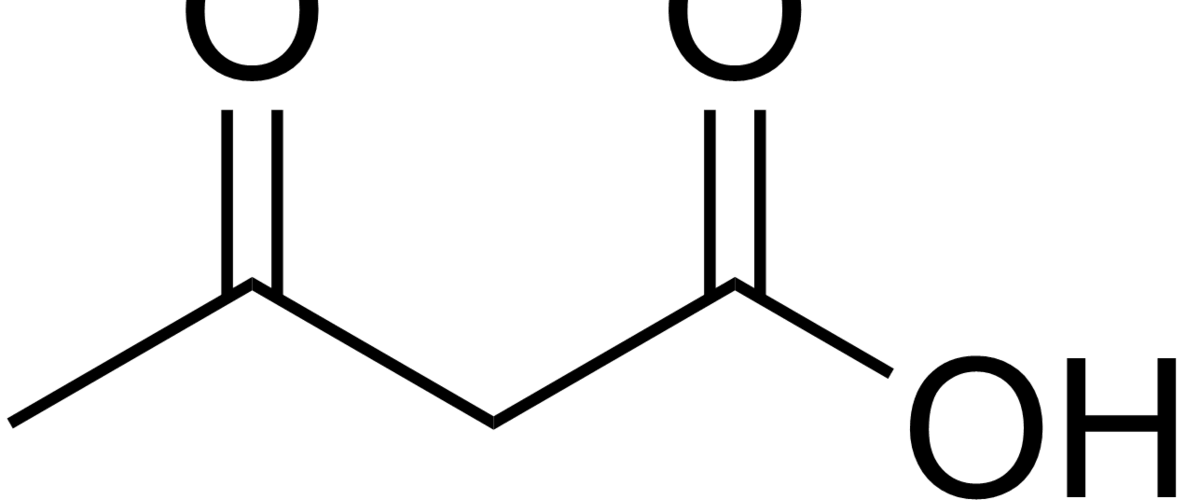
Ketosis is a metabolic state in which the liver produces small organic molecules called ketone bodies at “sufficient” levels, which I’ll expand upon later. First, let’s get the semantics correct. The first confusing thing about ketosis is that ketone bodies are not all – technically — ketones, whose structure is shown below. Technically, the term ketone denotes an organic molecule where a carbon atom, sandwiched between 2 other carbon atoms (denoted by R and R’), is double-bonded to an oxygen atom.

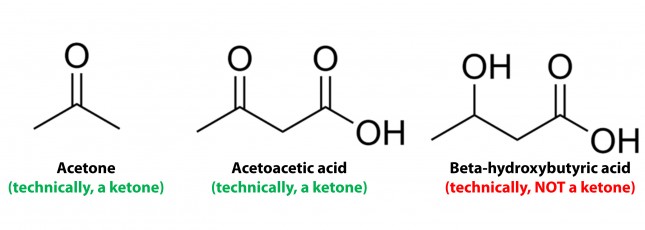
Conversely, the term “ketone bodies” refers to 3 very specific molecules: acetone, acetoacetone (or acetoacetic acid), and beta-hydroxybutyrate (or beta-hydroxybutyric acid), shown below, of which only 2 are technically ketones. (The reason beta-hydroxybutyrate, or B-OHB, is not technically a ketone is that the carbon double-bonded to the oxygen is bonded to an –OH group on one side, technically making B-OHB a carboxylic acid for anyone keeping score.)
Now, back to the real question at hand. Why would our body make these substances? To understand why or when the body would do this requires some understanding of how the body converts stored energy (the food we eat or the energy we store in our body, i.e., fat or glycogen) into phosphate donors. For a refresher on this process, please refer to the video in this post, specifically the section from 2:15 to 13:30.
The ATP issue
As you may recall, about 60% of the energy we expend, say 1,800 kcal/day for someone consuming 3,000 kcal/day in weight balance, is purely devoted to keeping us alive by generating enough ATP (“energy currency”) to do 2 things: allow ion gradients to function and allow muscular relaxation. So, obviously, we can’t tolerate – literally even for one minute – insufficient ATP production. In fact, one of the most potent toxins known to man (cyanide) exerts its effect on this process by inhibiting the electron transport chain which generates the bulk of the ATP our body produces. Even the most transient interruption of this process is fatal.
Take home message #1: No ATP, even for 1 minute, equals no life.
The brain issue
The brain is a particularly greedy organ when it comes to energy requirement. To put this comment in perspective consider the following: though our brain represents only about 2% of our body mass, it accounts for about 20% of our energy expenditure. (In children, by the way, this may be closer to 40-50% of basal metabolic demand.) So, beyond the ATP issue, above, there is a substrate issue with the brain as neurons derive most of their energy from glucose. While there is emerging evidence that neurons can also oxidize fatty acids directly in small amounts and may even prefer lactate (over glucose), these two substrates do not approach the levels of consumption by neurons that glucose does. So, for the purpose of this discussion, let’s just focus on the need of the body to provide glucose to the brain.
You’ll recall, from the point I made above, that my brain requires about 400 to 500 kcal of glucose per day (100 to 120 gm). You’ll also recall (from the video, above) that I can store about 100 to 120 gm of glucose in my liver. While I can store much more in my muscles, (on the order of about 300 to 350 gm), because muscles lack the enzyme glucose-6-phosphatase, glucose stored in muscle as glycogen is unable to re-enter the bloodstream and is meant for the muscle and the muscle alone to use. In other words, muscle glycogen is a stranded asset of glucose in the body to be used only by the muscle.
So, if I’m deprived of a dietary source of glucose, I depend solely on my liver to release glycogen (a process known as hepatic glucose output, or HGO). How long can HGO supply my brain with sufficient glucose? It depends on a few things that impact both the “source” and the “sink” of glucose. Other competing sinks for glucose (e.g., activity level, thermogenic needs) and sources (e.g., glycerol and gluconeogenic amino acid availability) can make a difference for a while. But, in a state of starvation we’ve only got about one to three days before we’re in trouble. If our brain doesn’t get a hold of something else, besides glucose, we will die quite unceremoniously.
Take home message #2: No glucose for 24-72 hours equals the need for something else the brain can use instead (that is not fat or protein, since neurons can’t oxidize fat and the last thing we want to do is start muscle wasting at a geometric rate).
The Krebs Cycle
This poses a real evolutionary dilemma. We need an enormous amount of energy just to not die, but the single most important organ in our body (also quite energy hungry in its own right) can’t access the most abundant source of energy in our body (i.e., fat) and is, instead, almost solely dependent on the one macronutrient we can’t store beyond a trivial amount (i.e., glucose). Obviously our species wouldn’t be here today if this were the end of the story. But, to understand how we survived requires one more trip down biochemistry memory lane. In the figure below (also included and described in the video) I gloss over a pretty important detail.
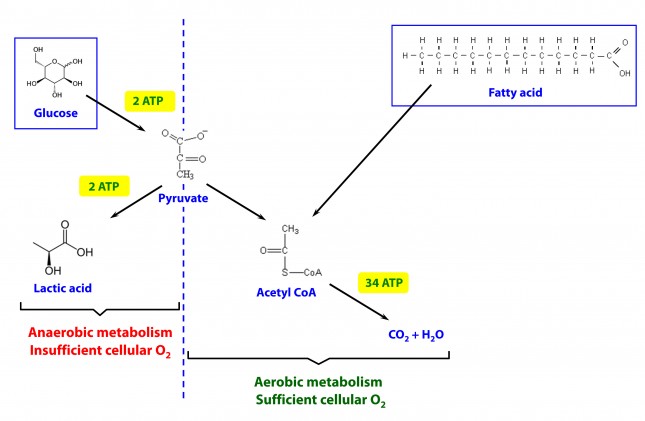
How, exactly, does our body take pyruvate (from glucose) or acetyl CoA (from fat) and generate so much ATP? The answer lies in the beauty of the Krebs Cycle, which feeds into a process called the electron transport chain (or ETC), I alluded to above. Since the adage ‘you can’t get something for nothing’ is as true in biochemistry as it appears to be in life, to get all that ATP (i.e., stored energy in the form of the phosphate bond), we need to give up something. What the ETC does give up, as its name suggests, is electrons. Through a series of redox reactions the ETC trades the stored energy held by electrons going from higher to lower energy states in exchange for the chemical energy stored in the bonds of the third phosphate group on an ATP molecule.
To think of it another way, if you start with stored energy – glucose or fat, for example, which if burned in calorimeter will give off varying amounts of heat – and you’re willing to convert their carbon, hydrogen, and oxygen molecules into another form with less energy – water and carbon dioxide which, if burned, produce very little heat – it’s a fair trade! The ETC is simply the vehicle that allows our body to make the switch.
In a car, by contrast, it’s much simpler. The engine combusts the hydrocarbon (e.g., gasoline) directly and in one flash liberates the heat contained within the hydrogen-carbon and carbon-carbon bonds in exchange for carbon dioxide, water vapor, and a few other things.
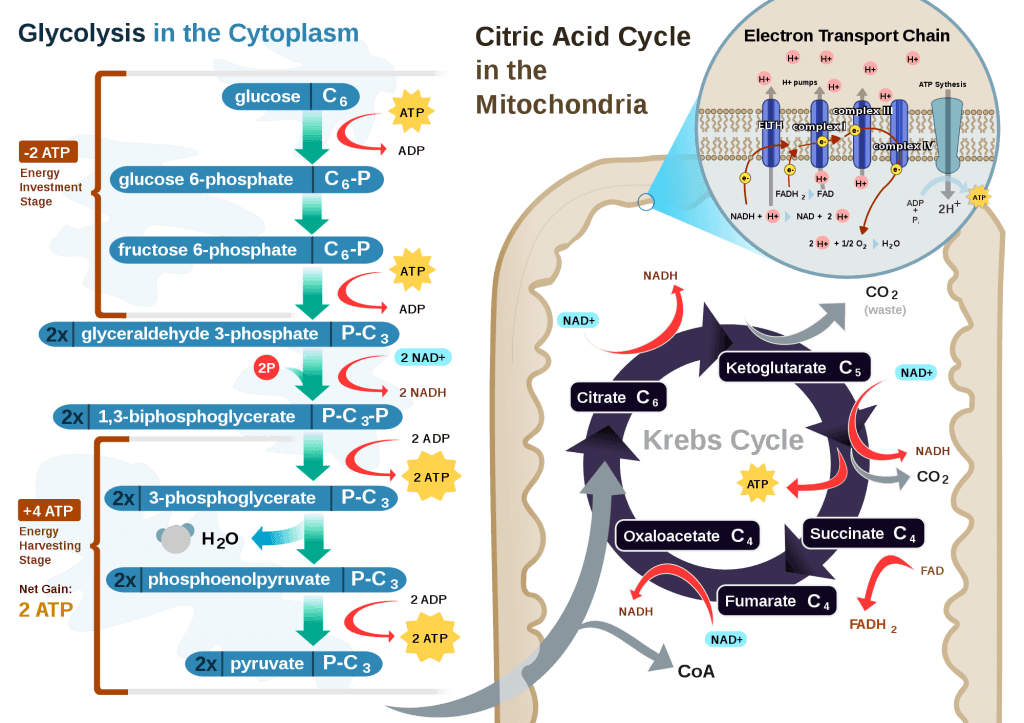
If you take a look at the figure, below, you’ll get a sense of the moving pieces involved in this cyclic transfer process. Molecules shuffle back and forth, around the cycle, and kick off spent carbon (carbon dioxide, termed “waste”) and reducing agents (e.g., conversion from NAD+ to NADH) for the ETC.
Where do the ketones come in?
In the absence of acetyl CoA (several ways this can happen, including substrate shortage, as I’m describing here) we evolved a cool trick. Our liver can make – out of fat or protein, though we much prefer to use fat so we can spare our protein and prevent severe muscle wasting – something called beta-hydroxybutyrate, one of the 3 ketone bodies I described above.
B-OHB and acetoacetate (see figure below from this paper by Cahill and Veech, 2003) are produced by the liver from long and medium chain fatty acids and released into the bloodstream.
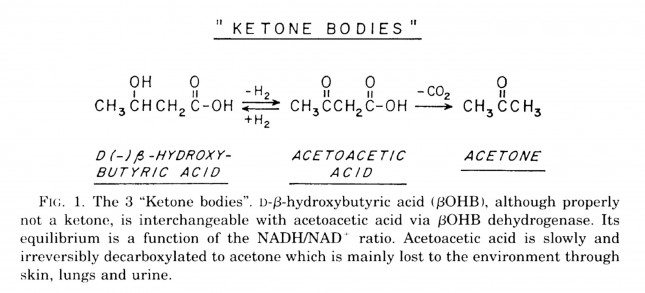
Acetoacetic acid and B-OHB live in reversible equilibrium (on the left), but once acetoacetate is converted to acetone (on the right) there’s no going back.
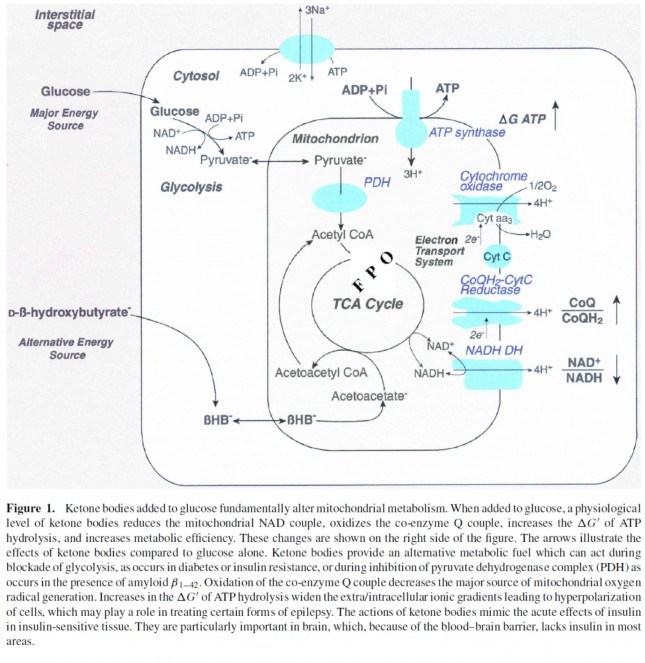
Now take a look at the figure below, from this 2001 paper. This is another rendition of the figure above showing the Krebs Cycle, but here you can see where B-OHB and acetoacetate enter the picture.
The reason a starving person can live for 40-60 days is precisely because we can turn fat into ketones and convert ketones into substrate for the Krebs Cycle in the mitochondria of our neurons. In fact, the more fat you have on your body, the longer you can survive. As an example of this, you may want to read this remarkable case report of a 382 day medically supervised fast (with only water and electrolytes)! If we had to rely on glucose, we’d die in a few days. If we could only rely on protein, we’d live a few more days but become completely debilitated with muscle wasting.
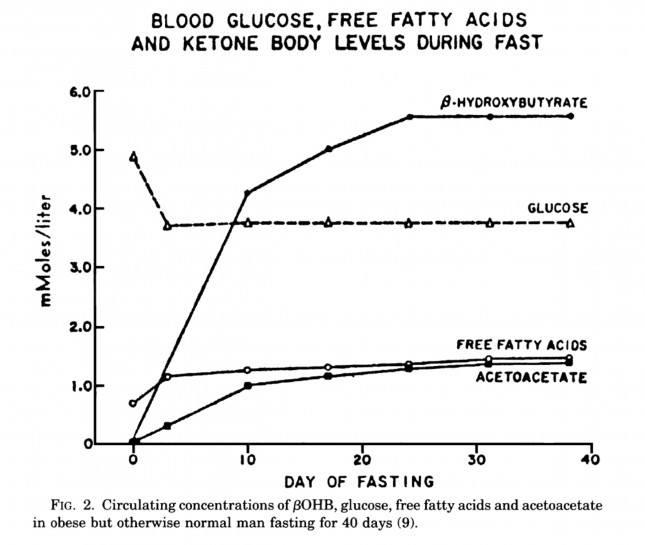
The graph below, also from the Cahill and Veech paper, shows the blood chemistry of a person starving for 40 days. Within about 3 days, a starving person’s level of glucose stops falling. Within about 10 days they reach a steady-state equilibrium with B-OHB levels exceeding glucose levels and offsetting most of the brain’s need for glucose. In fact, the late George Cahill did an experiment many years ago (probably would never get IRB approval to do such an experiment today) to demonstrate how ketones can offset glucose in the brain. Subjects with very high levels of B-OHB (about 5-7 mM) were injected with insulin until glucose levels reached 1 mM (about 19 mg/dL)! A normal person would fall into a coma at glucose levels below about 40 mg/dL and die by the time blood glucose reached 1 mM. These subjects were completely asymptomatic and 100% neurologically functional.
The last point I’ll make on the starving patient is that, as you can see in the figure below, the glucose level normalizes at about 65-70 mg/dL (about 3.7 mM) within days of fasting, despite no sources of exogenous glucose. Why? Because with so much fat being converted into B-OHB and acetoacetic acid by the liver, a significant amount of glycerol (the 3-carbon backbone of triglycerides) is liberated and converted by the liver into glycogen. As an aside, this is why someone in nutritional ketosis – even if eating zero carbohydrates – still has about 50-70% of a normal glycogen level, as demonstrated by muscle biopsies in such subjects.
Take home message #3: We evolved to produce ketone bodies so we could not only tolerate but also thrive in the absence of glucose for prolonged periods of time. No ability to produce ketone bodies = no human species.
Last point of background: Everything I’ve just presented is based on data from starving subjects. If one restricts carbohydrate intake, typically to less than about 20-50 gm/day (dependent on timing and carbohydrate composition), and maintains modest but not high protein intake (because protein is gluconeogenic – i.e., protein in excess will be converted to glycogen by the liver), one can induce a state referred to as “nutritional ketosis” with similar physiology to what I’ve just presented without resorting to starvation. Why you’d do this is something I will discuss later.
One other housekeeping issue: Ketosis versus DKA?
In a separate post, I explained the difference between nutritional ketosis (NK) and diabetic ketoacidosis (DKA). If this distinction is not clear, I’d suggest giving this separate post a quick skim for a refresher. DKA is a pathologic (i.e., harmful) state that results from the complete or near absence of insulin. This occurs in the setting of type 1 diabetes or very end-stage type 2 diabetes, and often as the result of a physiologic insult (e.g., an infection) where the patient is not receiving sufficient insulin to bring glucose into his cells. A person with a normal pancreas, regardless of how long he fasts (including the fellow I reference above who fasted for 382 days!) or how much he restricts carbohydrates, can not enter DKA because even a trace amount of insulin will keep B-OHB levels below about 7 or 8 mM, well below the threshold to develop the pathologic acid-base abnormalities associated with DKA. Let me reiterate, it is physiologically impossible to induce DKA in anyone that does not have T1D or very, very, very late-stage T2D with pancreatic “burnout.”
Embarrassing admission: I remember exactly where I was sitting in a clinic at Johns Hopkins in 2002 explaining to (admonishing, really) a patient who was on the Atkins diet how harmful it was because of DKA. I am so embarrassed by my complete stupidity and utter failure to pick up a single scientific article to fact check this dogma I was spewing to this poor patient. If you’re reading this, sir, please forgive me. You deserved a smarter doctor.
In Part II of this post I’ll tackle the questions I know folks still have on their mind (below). Until then, re-read this post to make sure you really understand this physiology. You’re already 10 steps ahead of the next person.
- Is there a “metabolic advantage” to being in ketosis?
- Are there dangers of being in ketosis?
- What are the most important things you need to know about getting into (or staying in) ketosis?

{kind=link}
I came to this article via your article on exogenous ketones. As a T2 diabetic long-distance cyclist a few months short of 70, I find the implications fascinating, specifically:
– might metformin, with its action of inhibiting glycogen release from the liver, starve the brain of fuel?
– might exogenous ketones (made palatable) become a regular part of treatment for all T2 diabetics, not just superannuated kids on bikes?
Thank you for sharing this valuable article I recently experienced ketosis and acetone taste in my mouth and I must admit it was a bit of a health care for me because there’s diabetes in our family my figure maybe I was diabetic however after going to the doctor and testing for diabetes I found out I was OK and just experiencing ketosis thank you for this enlightening article as it’s really helped me understand and further improve my journey to self empowered health I can’t thank you enough cheers!
the “Low cab Limbo” is true? if i stick to a 15% carbs, 20% protein and 65% fat i wouldn’t be in ketosis, but how bad is compared to full keto? some people say that follow a LC diet of 15%-20% carbs is actually worse than a +30% carbs,
A talk on ketosis mentioned that ketosis increases resting heart rate and that underlying causes of this are unknown. I am very curious to learn more about this. Have you seen cases of this sort? What are your thoughts on the matter?
I am new to this blog, so if my question is answered elsewhere, please refer me there.
Ketosis is often cited as a possible way to kill cancer cells. The theory is that cancer cell consume only glucose. However, in your graph, glucose level drops only slightly (from 5 to 3.7). Is that enough of a drop to produce the desired effect?
Great question! I wish I knew the answer, but I think the answer is “no” if the effect is all glucose-mediated.
I just read this post again, with great benefit, and this time actually read the Cahill and Veech 2003 paper. In the paper, the authors keep harping on how difficult the ketogenic diet is to maintain, and how only a small minority actually stay on it. Judging from my own experience, while it certainly requires commitment to obtain the understanding behind the metabolic details and thus the motivation to keep on plugging away till the housekeeping and logistic details of the diet become automatic and routine, even second nature, the diet itself is by no means “difficult”. Extrapolating from the large number of commenters on this post who appear also to be successfully maintaining a ketogenic diet, my experience is widely shared.
Am I missing something, and are the authors referring to some other iteration of the diet that we readers (athletes and metabolic improvers alike) seem to be finessing successfully? Or are the authors merely commenting on a larger population of perhaps less intensely educated and thus less successfully motivated subjects?
I think 1) it is difficult to consume a KD for long periods of time, and 2) the authors know little about them; when I ask them they had never tried it.
It is definitely not difficult to maintain a ketogenic diet for long periods of time – unless you are either very poor or your eating habits are strongly dictated by social norms (ie – let’s be obese, diabetic and die from a heart attack or cancer). I’ve been on a ketogenic diet for 5 years and can’t imagine a better or more enjoyable diet – once the dependence on carbs and the addiction to wheat have gone away there is zero attraction there. I have no illnesses – and didn’t have to start with – but I like being able to compete in endurance sport without having to constantly feed my face with sugar.
It would seem logical that supplementing with Ketogenic amino acids would increase ketones: Leucine and Lysine. Do you agree? Do you know of any studies that look at this?
Hi All,
I’m a personal trainer and I don’t think I,m too bad on Nutrition. I do bodybuilders body fats and diet plans as well as normal peopl!!! lol if you know what I mean.
One of the things I would like to know more about is at what stage does the body go into the ketosis state?
I know that when you are on a low carb diet that your glycogen in the muscles and liver start to get low. I understand that glucogan harmone kicks in and starts to convert glucose from fat cells.
So if a body builder has a body fat of 9% and goes to bed say at 10pm and gets up at 8am the next day. Has his metabolism been in a catabolic state at any of that time?
The way I see it is that the only time you would get into ketosis is if you run short on glycogen through calorie deficit or exercise and you are trying to do High intensity running ( Anarobic threshold) or heavy resistance weights?
I tell people that when they are in a calorie deficit they should take BCAA’s during their training expecially if they have not eaten any carbs or protein for a few hours.
Can someone please tell me if it is worth buying a ketone blood test monitor so I can tell if one of my bodybuilders is in a ketosis state. I need them to keep their muscle size and strength as much as they can whilst they are trying to lower their fat %.
Regards,
Roy Evans
[email protected]
The keytone meter isn’t that expensive – it is a one time cost. The strips can be a bit pricey. It is worth it. There is a ton of great info in Dr. Phinney’s book. I think on Amazon it is under $10.
I liked using a blood monitor when I first started Ketosis, as it told no lies, I could also contrast how I felt at 0.5mmol/l and 1.0mmol/l, and it was a noticeable feeling. I think feedback is very important especially adjusting to the diet. I used test strip religiously for the first year of nutritional ketosis. I think it depends on the client though, I’m sure some people are happy without it.
Question: how does someone that doesn’t have gallbladder, go on a keto diet?
Is it possible?
Is it recommendable?
thx,
J
I had my gallbladder removed 15 years ago. My experience with Keto diet is that it is both very do-able and effective.
Thanks. Should be fixed now.
My limited experience (cycling between 10,000 and 14,000 feet) suggested that lower RQ in NK allowed for less O2 consumption per unit ATP produced.
Take a look at The interplay between exercise and Ketosis posts.
I have been in ketosis for 90% of the time for the past two and a half years. My blood beta-hydroxybutyrate ranges from .60 to 1.90 mmol/l. I am not too concerned about the ketone level because the level will fluctuate given the balance between ketogenesis and ketolysis. Stephen D. Phinney, MD, Ph.D., co-author of “The Art and Science of Low Carbohydrate Performance” uses .50 mmol/l as the minimum.
My workouts are no impaired since I have been on the keto diet. I still get a pump with high rep exercises which indicates glycogen storage not detrimentally reduced. I’m 185 lbs with body fat at 9.7% measured by DXA scan. In fact, my lean mass has increased between the ten months period between two DXA scans. My diet is about 70% fats, 20% proteins, and 10% carbohydrates. I eat lots of green leafy vegetables which are low in carbs, high in fiber and they are sources of nitrates for the body to produce nitric oxide. The satiety state in spite of not eating for hours and mental clarity have been benefiting from the diet. I try to maintain an intake of protein sufficient for muscle protein synthesis and to avoid more than necessary which may result in breaking me out of nutritional ketosis.
Your YouTube video “Peter Attia – An Advantaged Metabolic State: Human Performance, Resilience & Health” has been a great source of information.
Dr Attia, thanks for the refresher – looking forward to the subsequent articles. Something that I think is fascinating is the role of protein in a ketogenic diet. For example, how much protein will get converted to glucose and under what circumstances? I watched a fascinating video from Dr Benjamin Bikman that explains the opposing roles of insulin and glucagon and he shows that what happens to protein on a ketogenic diet depends ultimately on the underlying metabolic state. From my experience with a ketogenic diet over the past year or so, there seem to be roughly “two camps” of thinking – the (1) “protein is bad for you/too much will kick you out of ketosis” and the (2) “eat protein to build/maintain lean muscle and limit fats depending on your body composition goals”. Both approaches can maintain ketosis obviously, but I think the role of protein is one that could be better understood in general. In weight loss circles, it is commonly seen advice to “lower your protein” if you are stalled, however, I think this “catch all” advice is not correct for everyone. I am posting a link to Dr Bikman’s video, I hope you don’t mind but I think it has been one of the clearest look at this issue that I have personally seen to date. https://www.youtube.com/watch?v=z3fO5aTD6JUWould be very interested for you to cover this aspect of ketosis as well.
Thanks for posting that video. It was very informative.
So its better to jog rather than train with weights to go into ketosis faster?
Or maybe gym can work here some indirect way, e.g. when you empty your muscle storage it can be filled from a liver one?
I’m glad I’ve gotten to the point that I understand most of this now. However, one beef I still have with the Ketogenic diet is how most implementations of it are going to be terrible for the environment, and how our meat production chain relies on antibiotic use putting us on collision course with superbugs. If you want to whip around the pre med textbook graphics, how about pathogenicity islands and how bacteria don’t have to be closely related to exchange resistance strategies? I do eat some meat because of Vitamin B-12, and now I eat more meat because I had ferritin deficiency (relying on greek yogurt for protein may have contributed). Rather than advantaged, I’d call ketogenic diet privileged.
Yes. I’m guessing a lot of people doing a ’16:8′ are in that ballpark.
Adding a little sodium usually solves the issue.
I suggest you look at Dom D’Agostino’s publications.