When I wrote part I of this post, I naively assumed this would only be a two-part series. However, so many great questions and comments emerged from the discussion that I realize it’s worth spending much more time on this important and misunderstood topic. In terms of setting expectations, I suspect this series will require at least four parts.
So, back to the topic at hand…. (You may want to read or maybe reread part I for a biochemistry refresher before diving into part II.)
Is there a “metabolic advantage” to being in ketosis?
Few topics in the nutrition blogosphere generate so much vitriolic rhetoric as this one, and for reasons I can’t understand. I do suspect part of the issue is that folks don’t understand the actual question. I’ve used the term “metabolic advantage” because that’s so often what folks write, but I’m not sure it has a uniform meaning, which may be part of the debate. I think what folks mean when they argue about this topic is fat partitioning, but that’s my guess. To clarify the macro question, I’ve broken the question down into more well-defined chunks.
Does ketosis increase energy expenditure?
I am pretty sure when the average person argues for or against ketosis having a “metabolic advantage” what they are really arguing is whether or not, calorie-for-calorie, a person in ketosis has a higher resting energy expenditure. In other words, does a person in ketosis expend more energy than a person not in ketosis because of the caloric composition of what they consume/ingest?
Let me save you a lot of time and concern by offering you the answer: The question has not been addressed sufficiently in a properly controlled trial and, at best, we can look to lesser controlled trials and clinical observations to a make a best guess. Believe me, I’ve read every one of the studies on both sides of the argument, especially on the ‘no’ side, including this one by Barry Sears from which everyone in the ‘no’ camp likes to quote. This particular study sought to compare a non-ketogenic low carb (NLC) diet to a ketogenic low carb (KLC) diet (yes, saying ‘ketogenic’ and ‘low carb’ is a tautology in this context). Table 3 in this paper tells you all you need to know. Despite the study participants having food provided, the KLC group was not actually in ketosis as evidenced by their B-OHB levels. At 2-weeks (of a 6-week study) they were flirting with ketosis (B-OHB levels were 0.722 mM), but by the end of the study they were at 0.333 mM. While the difference between the two groups along this metric was statistically significant, it was clinically insignificant. That said, both groups did experience an increase in REE: about 86 kcal/day in the NLC group and about 139 kcal/day in the KCL group (this is calculated using the data in Table 3 and Table 2). These changes represented a significant increase from baseline but not from each other. In other words, this study only showed that reducing carbohydrate intake increased TEE but did not settle the ‘dose-response’ question.
This study by Sears et al. is a representative study and underscores the biggest problems with addressing this question:
- Dietary prescription (or adherence), and
- Ability to accurately measure differences in REE (or TEE).
Recall from a previous post, where I discuss the recent JAMA paper by David Ludwig and colleagues, I explain in detail that TEE = REE + TEF + AEE.
Measuring TEE is ideally done using doubly-labeled water or using a metabolic chamber, and the metabolic chamber is by far the more accurate way. A metabolic chamber is a room, typically about 30,000 liters in volume, with very sensitive devices to measure VO2 and VCO2 (oxygen consumed and carbon dioxide produced) to allow for what is known as indirect calorimetry. The reason this method is indirect is that it calculates energy expenditure indirectly from oxygen consumption and carbon dioxide production rather than directly via heat production. By comparison, when scientists need to calculate the energy content of food (which they do for such studies), the food is combusted in a bomb calorimeter and heat production is measured. This is referred to as direct calorimetry.
Subjects being evaluated in such studies will typically be housed in a metabolic ward (don’t confuse a metabolic ward with a metabolic chamber; the ward is simply a fancy hospital unit; the chamber is where the measurements are made) under strict supervision and every few days will spend an entire 24 hour period in one such chamber in complete isolation (so no other consumption of oxygen or production of carbon dioxide will interfere with the measurement). This is the ‘gold standard’ for measuring TEE, and shy of doing this it’s very difficult to measure differences within about 300 kcal/day.
Not surprisingly, virtually no studies use metabolic chambers and instead rely on short-term measurement of REE as a proxy. In fact, there are only about 14 metabolic chambers in the United States.
A broader question, which overlays this one, is whether any change in macronutrients impacts TEE.
Despite the limitations we allude to in the summary of this review, there is a growing body of recent literature (for example this study, this study, and this study) that do suggest a thermogenic effect, specifically, of a ketogenic diet, possibly through fibroblast growth factor-21 (FGF21) which increases with B-OHB production by the liver.
These mice studies (of course, what is true in mice isn’t necessarily true in humans, but it’s much easier to measure in mice) show that FGF21 expression in the liver is under the control of the transcription factor peroxisome proliferator-activated receptor a (PPARa), which is activated during starvation. Increased FGF21 promotes lipolysis in adipose tissue and the release of fatty acids into the circulation. Fatty acids are then taken up by the liver and converted into ketone bodies. FGF21 expression in liver and adipose tissue is increased not only by fasting but also by a high fat diet as well as in genetic obesity which, according to these studies, may indicate that increased FGF21 expression may be protective. Hence, ketosis may increase TEE either by increasing REE (thermogenic) or AEE (the ketogenic mice move more). Of course, this does not say why. Is the ketogenic diet, by maximally reducing insulin levels, maximally increasing lipolysis (which dissipates energy via thermogenic and/or activity ‘sinks’) or is the ketogenic diet via some other mechanism increasing thermogenesis and activity, and the increased lipolysis is simply the result? We don’t actually know yet.
Bottom line: There is sufficient clinical evidence to suggest that carbohydrate restriction may increase TEE in subjects, though there is great variability across studies (likely due the morass of poorly designed and executed studies which dilute the pool of studies coupled with the technical difficulties in measuring such changes) andwithin subjects (look at the energy expenditure charts in this post). The bigger question is if ketosis does so to a greater extent than would be expected/predicted based on just the further reduction in carbohydrate content. In other words, is there something “special” about ketosis that increases TEE beyond the dose effect of carbohydrate removal? That study has not been done properly, yet. However, I have it on very good authority that such a study is in the works, and we should have an answer in a few years (yes, it takes that long to do these studies properly).
Does ketosis offer a physical performance advantage?
Like the previous question this one needs to be defined correctly if we’re going to have any chance at addressing it. Many frameworks exist to define physical performance which center around speed, strength, agility, and endurance. For clarity, let’s consider the following metrics which are easy to define and measure
- Aerobic capacity
- Anaerobic power
- Muscular strength
- Muscular endurance
There are certainly other metrics against which to evaluate physical performance (e.g., flexibility, coordination, speed), but I haven’t seen much debate around these metrics.
To cut to the chase, the answers to these questions are probably as follows:
- Does ketosis enhance aerobic capacity? Likely
- Does ketosis enhance anaerobic power? No
- Does ketosis enhance muscular strength? Unlikely
- Does ketosis enhance muscular endurance? Likely
Why? Like the previous question about energy expenditure, addressing this question requires defining it correctly. The cleanest way to define this question, in my mind, is through the lens of substrate use, oxygen consumption, and mechanical work.
But this is tough to do! In fact, to do so cleanly requires a model where the relationship between these variables is clearly defined. Fortunately, one such model does exist: animal hearts. (Human hearts would work too, but we’re not about to subject humans to these experiments.) Several studies, such as this, this, and this, have described these techniques in all of their glorious complexities. To fully explain the mathematics is beyond the scope of this post, and not really necessary to understand the point. To illustrate this body of literature, I’ll use this article by Yashihiro Kashiwaya et al.
The heart is studied because the work action is (relatively) simple to measure: cardiac output, which is the product of stroke volume (how much blood the heart pumps out per beat) and heart rate (how many times the heart beats per minute). One can also measure oxygen consumption, all intermediate metabolites, and then calculate cardiac efficiency. Efficiency increases as work increases relative to oxygen consumption.
Before we jump into the data, you’ll need to recall two important pieces of physiology to “get” this concept: the acute (vs. chronic) metabolic effect of insulin, and the way ketone bodies enter the Krebs Cycle.
The acute metabolic effects of insulin are as follows:
- Insulin promotes translocation (movement from inside the cell to the cell membrane) of GLUT4 transporters, which facilitate the flux of glucose from the plasma into the inside of the cell.
- Insulin drives the accumulation of glycogen in muscle and liver cells, when there is capacity to do so.
- Least known by most, insulin stimulates the activity of pyruvate dehydrogenase (PDH) inside the mitochondria, thereby increasing the conversion of pyruvate to acetyl CoA (see figure below).
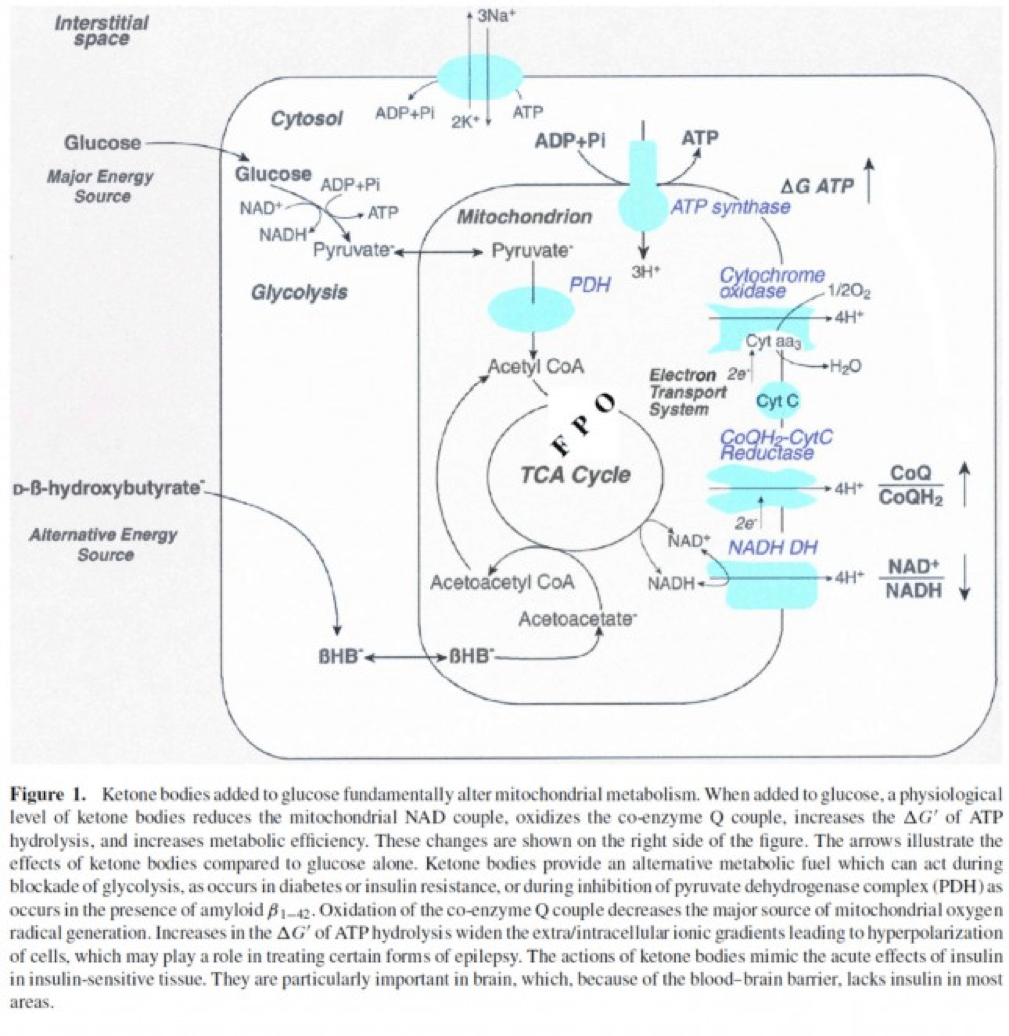
The second important point to recall is that ketone bodies bypass this process (i.e., glucose to pyruvate to acetyl CoA), as B-OHB enters the mitochondria, converts into acetoacetate, and enters the Krebs Cycle directly (between succinyl CoA and succinate, for any biochem wonks out there). I keep alluding to this distinction for a reason that will become clear shortly.
An elegant way to test the relative impact of glucose, insulin, and B-OHB on muscular efficiency is to “treat” a perfused rat heart under the following four conditions:
- Glucose alone (G)
- Glucose + insulin (GI)
- Glucose + B-OHB (GK)
- Glucose + insulin + B-OHB (GIK)
In fact, that’s exactly what this paper did. Look at what they found:
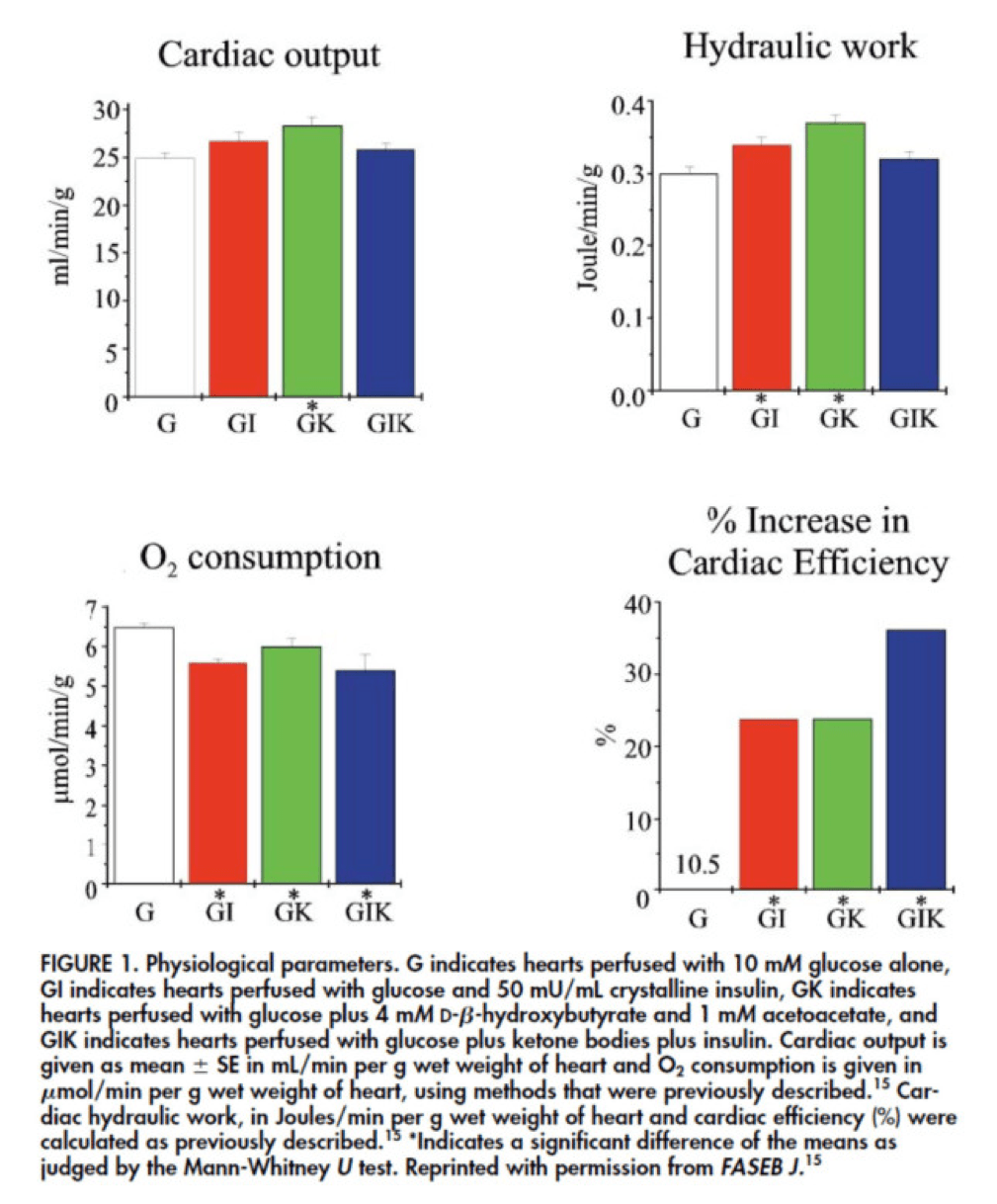
The upper two graphs in this figure show similar information, namely the response of cardiac output and hydraulic work to each treatment. (Cardiac output is pure measurement, as I described above, of volume of blood displaced per unit time. Hydraulic work is a bit more nuanced; it measures the mechanical work being done by the fluid.)
Adding insulin to a fixed glucose (GI) load increases both cardiac output and hydraulic work, but it’s only significant in the case of hydraulic work. Conversely, adding B-OHB to glucose (GK) increases both cardiac output and hydraulic work significantly. Interestingly, combining insulin and B-OHB with glucose (GIK) increases neither.
Oxygen consumption was significantly reduced in all arms relative to glucose alone, so we expect the cardiac efficiency to be much higher in all states. (Why? Because for less oxygen consumption, the hearts were able to deliver greater cardiac output and accomplish greater hydraulic work.)
The figure on the bottom right shows this exactly. If you’re wondering why the gain in efficiency is so great (24-37%), the answer is not evident from this figure. To understand exactly how and why adding high amounts of insulin (50 uU/mL) or B-OHB (4 mM) to glucose (10 mM) could cause such a step-function increase in cardiac efficiency, you need to look specifically at how the concentration of metabolic intermediates (e.g., ATP, ADP, lactate) varied in the rat heart cells.
This is where this post goes from “kind of technical” to “really technical.”
The figure below presents the results from this analysis. The height of the bar shows the fold-increase for each of the three treatments relative to glucose alone. To orient you, let’s look at a few examples. In the upper left of the figure you’ll note that GI and GIK both significantly increase glucose concentration in the cell, while GK does not. Why? The GI and GIK treatments both increase the number of GLUT4 transporters translocated to the cell surface so more glucose can flux in. GK does increase glucose concentration, but not significantly (in the statistical sense).
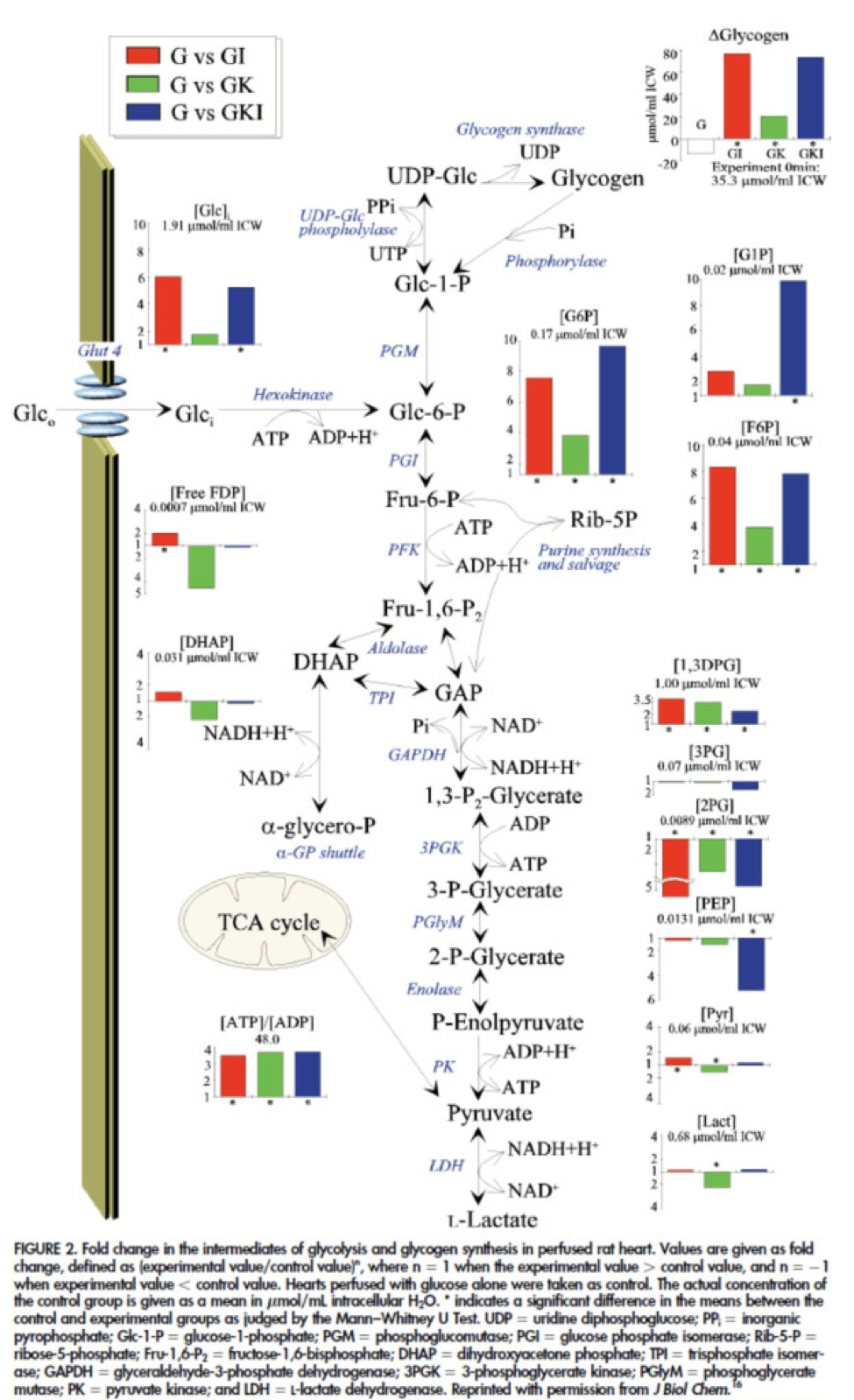
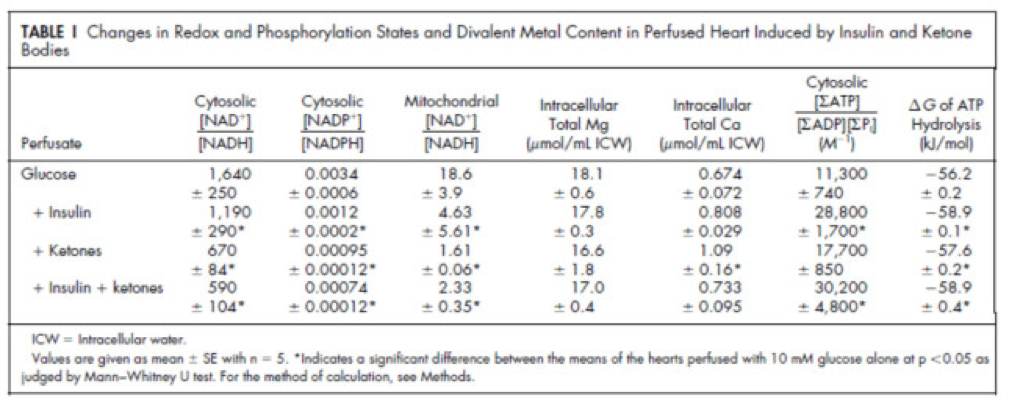
Table 1 from this paper, below, summarizes the important changes from this analysis. In particular, look at the last column, the Delta G of ATP hydrolysis.
I was really hoping to write this post without ever having to explain Delta G, but alas, I’ve decided to do it for two reasons:
- To really “get” this concept, we can’t avoid it, and;
- The readers of this blog are smart enough to handle this concept.
Delta G, or Gibbs free energy, is the “free” (though a better term is probably “available” or “potential”) energy of a system.
Delta G = Delta H – Temperature * Delta S, where H is enthalpy and S is entropy. The more negative Delta G is, the more available (or potential or “free”) energy exists in the system (e.g., a Delta G of -1000 kcal/mol has more available energy than one of -500 kcal/mol). To help with the point I really want to make I refer to you this video which does a good job explaining Gibbs free energy in the context of a biologic system. Take a moment to watch this video, if you’re not already intimately familiar with this concept.
Now that you understand Delta G, you will appreciate the significance of the table above. The Gibbs free energy of the GI, GK, and GIK states are all more negative than that of just glucose. In other words, these interventions offer more potential energy (with less oxygen consumption, don’t forget, which is the really amazing part).
To see what the substrate-by-substrate changes look like across the mitochondria and ETC, look at this figure:
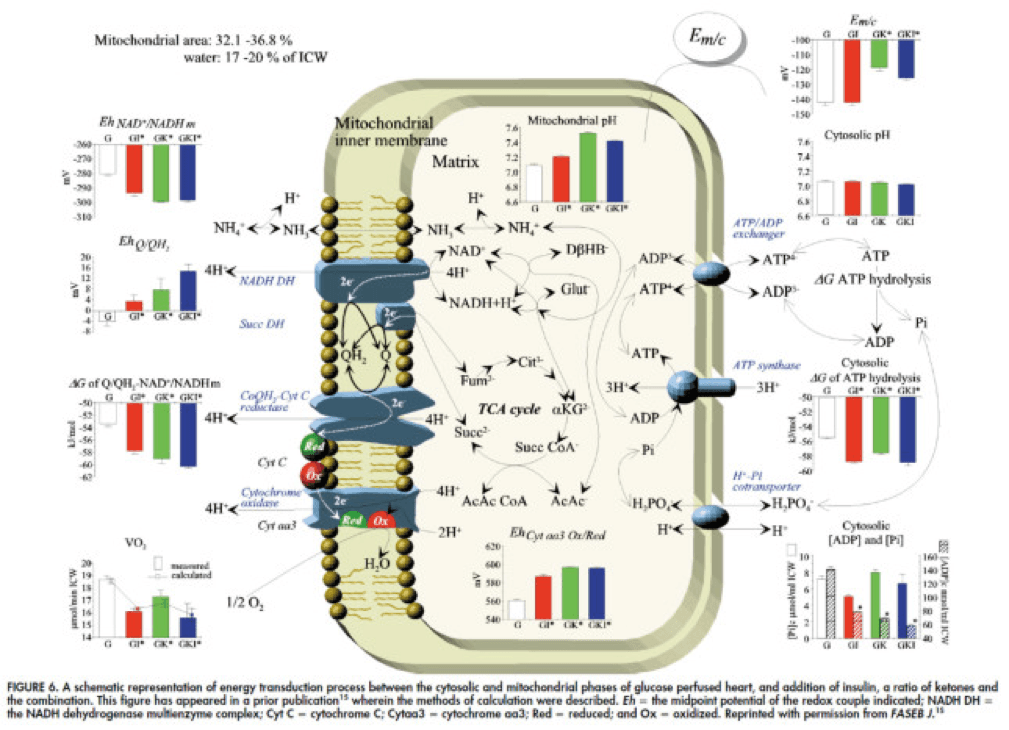
Though it is by no means remotely obvious, what is happening above boils down to two major shifts in substrate utilization:
- In one step the reactants NADH/NAD+ become more reduced (in the chemical sense), and;
- In another step the reactants CoQ/CoQH2 become more oxidized (in the chemical sense).
These changes, taken together, widen the energetic gap between the states and, in turn, translates to a higher (i.e., more negative) Delta G which translates to greater ATP production per unit of carbon.
Additional work, which you’ll be delighted to know I will not detail here, in fact shows that on a per carbon basis, B-OHB generates more ATP per 2-carbon moiety than glucose or pyruvate. As an aside, this phenomenon was first described in 1945 by the late Henry Lardy, who observed that sperm motility increased in the presence of B-OHB (relative to glucose) while oxygen consumption decreased!
Is there a reason to prefer GK over GI?
Yes. Recall that ketones make their way onto the metabolic playing field without going through PDH. Adding more insulin to the equation forces more pyruvate towards PDH into acetyl CoA. While B-OHB “mimics” the effect of additional insulin, it does so in a much cleaner fashion without the complex cascade of events brought on by additional insulin (e.g., decreased lipolysis) and, perhaps most importantly, avoids the logjam of impaired PDH due to insulin resistance (I’ll come back to this point in a future post when I address Alzheimer’s disease and Parkinson’s disease). In essence, B-OHB “hijacks” the Krebs Cycle via a slick trick that lets it bypass the bottleneck, PDH. All the glucose and insulin in the world can’t overcome this bottleneck. It’s truly a privileged state and a remarkable evolutionary trick that we can utilize B-OHB.
Back to the original question…
Clearly, in the highly controlled setting of a perfused rat heart, ketones offer an enormous thermodynamic advantage (28%!). But what about in aggregate human performance? There is no reason to believe that therapeutic levels of B-OHB (either through nutritional ketosis or by ingesting ketone esters) would increase anaerobic power, since the anaerobic system does not leverage the Delta G improvement I’ve outlined here. Same is true for muscular strength. However, there is reason to believe that aerobic capacity and muscular endurance could be improved with sufficient B-OHB present to compliment glucose.
It turns out this has been demonstrated repeatedly in subjects ingesting ketone esters, developed by Dr. Richard Veech (NIH) and Dr. Kieran Clarke (Oxford). Because the results of their work have not yet been published, I can’t comment much or share the data I have, which they shared with me. I can say the ingestion of B-OHB in the D-isoform (the physiologic isoform), resulting in serum levels between 4 and 6 mM, did lead to significant increases in aerobic power and efficiency in several groups of elite athletes (e.g., Olympians) across multiple physical tasks maximally stressing the aerobic system.
Once published, I believe these studies will be a real shot across the bow of how we view athletic performance. It is very important to point out, however, that these studies don’t exactly address the most relevant question, which has to do with nutritional ketosis. In other words, ingesting ketone esters to a level of 4 to 6 mM might not be the same as de novo producing B-OHB to those levels. But, such trials should be forthcoming in the next few years. Personally, I am most eager to see the results of a ketone ester alone versus nutritional ketosis versus combination treatment, all to the same serum level of B-OHB.
The Hall Paradox
For the really astute readers, you may be saying, “Waaaaaaaait a minute, Peter…if ketones increase Gibbs free energy while reducing oxygen consumption, should this imply TEE goes down?” You’re right to ask this question. It was the first question I asked when I fully digested this material. If each molecule of B-OHB gives your muscles more ATP for less oxygen, you should expend less not more energy at the same caloric intake, right?
I was discussing this with Kevin Hall at NIH, an expert in metabolism and endocrinology. Kevin pointed out the error in my logic. I failed (in my question) to account for the energetic cost of making the ketones out of fat. Remember, in the experiments described above, the B-OHB is being provided for “free.” But physiologically (i.e., in nutritional ketosis or even starvation), we have to make the B-OHB out of fat. The net energy cost of doing this is actually great. According to Kevin, it is not generally appreciated how making ketones from fatty acids affects overall energy efficiency. Nevertheless, this can be examined by comparing the enthalpy of combustion of 4.5 moles of B-OHB, which is about -2,192 kcal, with the enthalpy of combustion of 1 mole of stearic acid (about -2,710 kcal) that was used to produce the 4.5 moles of ketones. Thus, there is about 20% energy loss in this process. Hence, the energy gain provided by the ketones is actually less than the energy cost of making them, at least in theory.
This suggests that being in nutritional ketosis may require more overall system energy, while still increasing work potential. In other words, a person in nutritional ketosis may increase their overall energy expenditure, while at the same time increasing their muscular efficiency. In honor of Kevin, I refer to this as the Hall Paradox.
Parting shot
Ok, if you’re still reading this, give yourself a pat on the back. This was a bit of chemistry tour de force. Why did I do it? Well, frankly, I’m tired of reading so much nonsense on this topic. Everybody with a WordPress account (and countless people without) feels entitled to spew their opinions about ketosis without even the slightest clue of what they are talking about. As I said in part I of this series, there is no bumper sticker way to address this question, so to say ketosis is “good” or “bad” without getting into the details is as useful as a warm bucket of hamster vomit (unless you’re Daniel Tosh, in which case I bet you can find a great use for it).
Next time, I’ll try to back it out of the weeds and get to more clinically interesting stuff. But we had to do this and we’re better for it.
Chemistry by Marcin Wichary is licensed under CC by 2.0



I just made the suggestion that a ketogenic diet might plausibly enhance muscular growth as well as recovery (https://www.ketotic.org/2012/12/bcaas-and-keto-diets.html). I’d be interested in your thoughts about that.
I’ve seen data to suggest (and have experienced personally and with clients) that one can gain lean mass on a KD. The question is if there is an advantage over a non-KD. I would need to see more data on BCAA-B-OHB interaction to have an opinion.
I’ve heard many criticisms of ketosis as of late…probably because you’ve popularized it to a certain extent. What really annoys me, personally, is people referring to a state of ketosis as being in a state of starvation. Even when I present my own experiences of satiety, muscle maintenance, and high energy levels (not a result of starvation) when in nutritional ketosis, I get told that I must not have been in ketosis over a long period of time, if at all. In short, I don’t know what I’m doing or what I’m talking about.
Shortly after reading your blog posts last spring, I decided to give NK a try. I did this along with IF. I had planned to do IF all along, and I decided to both together for maximum results. I would eat my first meal at 11 or 12 and my last one at 8-9 at night. I did short fasts. Because I didn’t want to put too much stress on my body at once, I didn’t exercise for the first two weeks (I went 13 days). I do sprints on the regular basis, and when I did my first sprint on Ketosis I noticed that I was a lot slower. I’d read that you could lose a little power, but I had lost a considerable amount of top end speed. But after a few sprints I realized that I was hardly even breathing hard. I never run long distance, but I got the urge to start running. I ran about 2 miles, averaging just over 6 minutes per mile, not lighting fast, but not a jog. I was amazed that I didn’t even really have to catch my breath afterward. This continued for the 8 weeks I was in ketosis. Not to mention that I went from about 12% body fat down to 9%.
My evidence is merely anecdotal, but for me, ketosis definitely increased my aerobic capacity. And towards the end, I was actually regaining some top end speed.
Nathan, I think I can actually say I’ve also regained most of what I lost at the very top end. But my comfort level at 60-70% VO2 max is getting greater and greater each month.
My experience has been exactly the same. I’m starting to regain speed and muscle strength after an initial drop.
Did you supplement with magnesium? After I’ve started sprinting a couple of times per week again I’m often getting cramps in my calfs even though I’m supplementing with magnesium 3-4 times per week. Did you ever experience that?
Hemming,
I did not supplement with magnesium. The cramps may have been due to a lack of potassium. Potassium actually works within the cells, and if it is absent it can cause cramping. Ironically, a lack of sodium can cause ones lack of potassium, as the body will often ditch potassium to hold on to sodium. If the cramps occurred during your sprints, I’d up your potassium intake a bit the next time. Also, make sure you get enough sodium, your kidneys don’t hold on to sodium as well when you go low carb, and NK is as low as it gets. I ate a lot of spinach when I was in NK for extra potassium. I’d also eat blueberries and raspberries directly after workouts, about a cup. Cheese and nuts were my other ubiquitous sources of potassium. I did drink about a gram of bullion most days, and two or three on days when I lifted weights to avoid hypotension (light headedness). I also salted my foods quite a bit.
Did the cramps occur during running, or after?
Hi Nathan,
Thank you for sharing your experiences.
My cramps happen at night. A few times I’ve woken up at night to go to the bathroom (i.e. not because of the cramps) but my calfs were cramped to a point where I could almost not walk. My main problem is that it feels that my calfs are sore or cramping all the time. It has been like this for a prolonged period and to an extent where I often feel ‘discouraged’ to get and walk because of the feeling in my legs. I’ve tried supplementing with magnesium and recently cold showers, both seem to help but not enough. I haven’t had bad running-incuded cramps but I’ve felt it from the cramps/soreness that was already there. Sometimes I also experience cramps in my fingers which may be another indication that I’m deficient in the minerals.
I add a salt consisting of 50% sodium, 40% potassium and 10% magnesium to all my meals. I have not had problems with hypotension symptoms although my blood pressure is very low (outside the recommended range).
I might add that I’m sort of recovering from a longer period of a lot of cardio (not in NK) where I came to a point where I could not continue and my blood platelets had dropped to levels far below normal. This has most likely also caused my mineral levels to go way too low.
Maybe I just simply need to add even more salt to my food even though I think I add quite a bit.
I forgot to mention:
I’m contemplating it could also be related to that I’m not eating enough fat (while keeping both protein and carbs low) as I’ve lost weight (I’m currently 178cm and 110-114lbs/50-52kg) after going NK. Do you have any experience with fat intake and correlation of your performance/feeling in general? I’ve had some serious mood swings and for me there seems to a positive correlation between my mood and how much I eat. The problem is just that I don’t really have a big appetie in ketosis.
Hemming,
I couldn’t run or sprint until I started wearing Vibrams, I always had a lot of pressure in the front of the legs whenever I ran… shin splint like pressure. After my first sprinting session in my Vibrams, my calves were so sore that I was walking straight legged the next day, and I couldn’t runs sprints for quite a few days. It took a few months for me to be able to sprint with not calve pain. It seems that you just need to let your calves heal up. Give yourself some time off.
Also, you may be putting too many stressors on your body at once. Adapting to Ketosis while also trying to adapt to new forms of exercise may be too much for your body to handle. Not to mention the former stress your body was in from chronic cardio. I’d lay off the exercising for a few weeks and let your body heal. You’d probably gain a few pounds as well.
At this point, your body is more than likely adapted to your old life style. Weighing 115 at 168cm and having troubles adapting to low carb are signs that your body is under a lot of stress. You may end up needing to take it slower and pack on a few pounds before resuming NK. However, there are some things to try first. One, as I said, take a break from exercise. I’ve found that this can especially important during ketosis. You will heal and be stronger for it. 2 weeks should be sufficient. The problems with your mood and such are more than likely a result of your transition to a low carb diet, which is only exacerbated by the moderate protein and low carb intake of NK. You should up your protein intake. It may lower ketone levels a bit, but it will help you transition. Shot for about 200 grams per day for 2 or 3 weeks. Doing this and resting for the next few weeks should yield you significant improvements. While your not exercising your body will replenish its glycogen stores and lay off the signaling for carbs. The extra protein will help heal your muscles and give your body some extra glucose without having to take in carbs. Adding protein can sound counter intuitive, and if you were fat adapted it would very likely hamper your progress, but it seems to work well for carbavores kicking the habit.
Putting extra salt on your food is probably a good idea. The kidneys just don’t hold on to sodium as well when you’re low carb. So far as your BP is concerned, I don’t have a lot of answers, if you think it’s a problem I’d get it checked out. My guess would be that if you put on about 20 pounds, you’d see a slight rise in blood pressure.
Hi Nathan,
Ironically, I did a sprint session yesterday which went far above expectations, only around 10% below my peak when I was not in ketosis. This is a major improvement compared to earlier sessions in ketosis.
The other things you mention regarding shoes, reducing exercise, fat adaption etc. is already in order. Even before I started cutting carbs way down I would argue that I was metabolically flexible always running fasted in the morning. The ‘interesting’ thing about this that even after I stopped running >60km/week I continued to lose weight.
I’ve started to keep a food log to see how much I actually eat. I think this has made me realise that I’m simply not eating enough fat to fuel my body. The problem for me is that I simply dont have the hunger to consume enough food. I know some will say keeping a log is a bad idea for someone trying to gain weight but for me it helps me in making sure I get enough food. The first couple of days I was surprised to see how little I actually eat (especially given that I’m more active than most people, not just exercise but in general). I’ll continue experimenting with my food intake, I think that’s the real issue in this. A low carb, low to medium fat diet is a way to failure.
By the way, I’m having my blood work done with regular intervals and have a continuous dialogue with my doctor about it. Even though I’ve been off the chronic cardio for several there is no doubt that my body is still recovering – I was feeling more than awful on several accounts when I stopped that regime.
Thank you for sharing your thoughts!
This was worth reading Peter especially the Gibbs Free Energy youtube vid. I will also chew on a lot of the other information until I don’t have to think much to understand it. I can now join others in saying thanks. I now understand you’re not just on a quacky trend receiving blog-cheers by many who probably don’t see your deeper disciplines in making science connect us to a world-view that we can apply daily in Ketogenics and in enduring lifestyles.
Thanks again for your generous email replies as well. —Geo
Thanks, Geo.
Many of us are glad you did not name this the Hall Effect or the Spin Hall Effect or even the Anomalous Hall Effect – tho’ I guess Anomalous and Paradoxical have quite a similar meaning . . . .
Thanks for writing this post, Peter. I really appreciate the amount of researching, reading, and writing time a post such as this would take.
I am really interested in your thoughts on the application of NK to different types of endurance athletes. As you probably well appreciate, the term “endurance athlete” is used as a bit of a cookie-cutter term, when in actual fact there is a huge variability in the types of endurance athletes. Compare a track cyclist to a Pro-tour rider, for example.
I recently wrote and I’m of the opinion that NK might be more suited to endurance athletes who tend to sit on a fairly sustained pace – like IM/triathletes. In those keto-adapted, they are able to sit at a high aerobic pace for a lot less oxygen cost, as you described here. I’m less convinced that NK is suitable for any endurance athlete with a considerable “sprint” component to their race. Stage racers in cycling for example need to be able to throw down multiple attacks, bridges, hill crests, and still have plenty of top-end for a potential sprint finish. The reference slips my mind at present, but I have seen a breakdown of the likes of TdF stages that show athletes spend a good portion of time “aerobic” but the decisive moves within the race are very much lactate threshold and then some.
I have seen your previous writing on how you have lost a bit off your top end, and it is interesting to see you have gained MOST of it back. Most isn’t all, and whilst the oxygen cost during the quiet sections of a race might not now be as taxing on you, I wonder how well you could compete with a rider who has a top-end which hasn’t been partially blunted by NK?
Do you have any thoughts around the types of endurance athletes you feel are best suited to using this “tool”. Again, my feelings are that IM competitors might do well, but that track cyclists, criterium racers, and even Crossfitters doing multiple 20-30 minute “WODs” per week, are not that well-suited to using NK (though certainly with the latter group, the promise of shaving a couple of percentage body fat points off may be too tempting for them not to give it a go anyway).
Cheers,
Jamie
These are great questions, Jamie. Consider, as you suggest, a rider in the TdF (minus the usual chemistry and pharmacopia). They need to be able to do it all. TT for an hour. Ride hard for 6, then finish a climb at >400 watts. You name it. There is not doubt that ketosis would enhance parts of this, but what I don’t know (assuming they make the ketones de novo — i.e., NK) is if that gains offsets any loss carb reduction elsewhere? Based on the data I have seen, exogenous ketosis (i.e., athletes ingesting ketone esters to high levels, like 6-7 mM), is a win-win. They get the benefits of ketosis without needing to sacrifice anything on the anaerobic side. So much work needs to be done here. I hate to even speculate on this.
Peter,
I visit your site regularly as I try to reaffirm my diet choices. I have been on a diet that would be similar to your 2009 to 2010/11 before you went total ketosis. I am scheduling cholesterol panels while getting blood work for hypothyroid issues that I have. These will be my control as I venture down trying your path.
The diet that I have been on to this point has yielded a total weight loss of abt. 80lbs, give or take depending on the day, and holiday if appropriate.
I am a former Marine, and I have a very large frame, 22″ biceps type/football dream type. I am only 6.07′, so it is surprising when I tell people that I weighed in at 310lbs. They know I have lost weight but they are mystified when I tell them what my total weight was once was.
My family has a history of cholesterol build up in our main arterial tracks. So 6egg Yolks and 3egg whites scares me a little bit. That being said, I truly believe you, Gary Taube, Mary Enig etc. are on the correct path. In other words I have taken the Red Pill. This happened in 2007-2008 when I decided to research the financial system because it pertained to my own personal business.
I saw the new blog post, and all I really wanted to say is…. Keep it up. I understand exactly what you are going through. As I said, I own my own personal business that is very successful, and I hold down a W2 job doing engineering. I spend hours responding to posts on forums blogs etc. . I respect your level of dedication, and from a personal stand point I know what kind of time this takes….. I don’t care how fast you can type (despite the fact that you’re a rocket scientist:-)(NOTE: personal business is AVIONICS related), it still takes time and thought.
I just wanted to say Thank you!
KC
Thanks, KC. It does take more time than I’d like to spend, especially on posts like this. Luckily my wife is profoundly understanding and supportive, without which I’m pretty sure this blog would have shut down a year ago.
Hey have you read the book we want to live? Do you have any of your saturated fats raw such as raw milk?
Nope
Wow. I was actually able to comprehend this. Nutritional ketosis seems appealing. I’ve tried, but it is very difficult to adhere to such a strict diet. Even after a moderate LCHF-diet for about a year I find it very difficult to stick to the ketogenic diet for a long enough time do really enjoy the benefits.
Are you planning a mini guide on how to actually do it, or know of a resource where I can find meal plans etc?
Yes, but you’ve hit on a great point. For many folks, it’s not easy…which is exactly why I want folks to understand it well enough to make an informed decision. Life is about optimizations and trade-offs.
Not sure why everyone says this is very hard to do, unless you are doing the ultramarathon champion thing like Jonas Colting. 🙂
I mean this most seriously. If you toss open Louis Diat’s classic “French Cooking for Americans,” which is noted for having easier recipes than Julia Child, and plug any of the classic recipes into an online system, you’ll see where they all fall on the fat scale. 😉 Just replace the potatoes with kohlrabi, turnips, or cauliflower and you’re done.
For example, his Farmer’s Ragout made with pork neck – a very old French country recipe. This contains 2 pounds fat pork neck meat with bones, water, 1 c cream, 3 T lard, a medium onion, a leek, substitute 1 c kohlrabi or turnips for the potatoes, garlic, 1-1/2 c celery, parsley to garnish, bay leaf, 1 small carrot, salt, pepper. Stew until delicious & thicken with the cream. Serves 6. And you’re looking at 8 total g carbs per serving with 70% fat.
It’s true some folks have to eat as much as 85% fat overall per day (think Jimmy Moore) but most people can get their blood ketones up to 1.5 easily at 70-75%, as long as they do some exercise as well (by which I don’t mean swimming to Catalina isn’t necessary, but a normal exercise class 2 or 3x a week.)
So I continue to contend that ketosis is easily achievable by normal people who just have to “force” themselves to somehow swallow that horrible weird stuff known as “classic french country cooking.” It’s tough I know. People make this seem harder than it has to be. I don’t know why – just cook like Julia, Louis Diat or Elizabeth David. (Btw the last I measured, my blood ketones came out to 2.4. Just saying.) It’s all normal, delicious, easy peasant food that everyone loves to eat. 🙂
Yes yes, I second Preben’s comment, a mini guide to achieve NK would be nice 🙂
Where I live, I cannot find a blood ketone meter in the market. Last week, I just had a lab check my fasting blood ketone along with my routine check up (an additional 20 dollars just for the blood ketone test), and it was a mere dissapointing 0.3 mM.
Even though I have abolished all kind of carbs except for a very small portion of green veggies daily, I suspect that my fat intake is still not optimal, still too much protein.
So I think that’s the problem for me. Not about adherence. But being in a third world country (Indonesia), it is hard to find food materials that are high in fat. I’m still fortunate that I can still increase my consumption of pork and bacon (even bacon here is not as fatty). But my fellow moslems will find it even harder to up their fat intake.
So yes, a mini guide to achieve NK would be very nice indeed 🙂
I’m pretty sure at the rate I’m going at least one part to this series will need to be entirely devoted to the “ins and outs” of NK.
Well, have you read the Low-carb Diet for Athletes by Phinney and Volek? NK is their child 🙂 and they explain both theory and practice very well.
Hi Ivan:
In Indonesia ketosis is soooo easy for you. It’s call coconut oil. Cook with fat lamb or fat beef and use plenty of palm or coconut oil for everything. If you struggle with knowing, start eating 75-80% of your daily calories as fat, 15% as protein, and the rest as carbs. Unless you are heavily insulin resistant, prediabetic, or massively overweight (think Jimmy Moore), you shold be successful at 75% fat if you exercise in a normal way 3x a week as well.
But should you have struggles similar to Jimmy, then go ahead and adopt his 85% fat, 12% protein, 3% carbs. You will soon be extremely successful that way, but not everyone has to be so high end in the fat. 😀 It’s really not difficult if you look at your recipes and follow Volk’s advice: “When in doubt, eat fat.” Best wishes!
@Peter: Yaaay, thanks Peter 🙂 Really looking forward to it.
@Martin: No I have not. I guess I have to order the book from Amazon. Thanks for the input.
@greensleeves: Coconut Oil hmmm? Thanks for the input, I have not really look into coconut oil. I use olive oil and butter for cooking. What do you think about coconut milk?
I’m a 36yo with DM Type 2, so yeah, I’m aiming for more into Jimmy’s percentage.
I’m not worried about my carb intake. I’ve abolished them altogether. Now for the remaining fat and protein macro. The thing is not about the percentage, but how to achieve that percentage with the raw materials available here.
Even grain-fed, meats are rarely fatty and tend to be on the leaner side compared to what available in first world countries. Grass-fed meat I bet will even be leaner but also impossible to find. Bacons have more red area than white. I can’t find heavy cream anywhere either. All grocery stores are selling low fat products *sigh* since nobody wants to buy high fat product, there’re simply no demands.
I guess I have to revert to what Indonesians do best. Cooking internal organs LOL 🙂
I’ve been in NK since September, 15 pound loss, feel pretty good, and re-starting a running program.
Sticking to anything new requires some mental judo. There is a new book called The Willpower Instinct by Kelly McGonigal out of Stanford. There are some important thoughts in it.
How you frame the changes is vital. If you say “don’t think about carbs, I won’t have carbs, keep me away from carbs” sooner or later you will probably crack. I see some hint of that in your “such a strict diet” comment.
But if you say, “I want to be healthy and vigorous. Therefore I will eat bacon and eggs for breakfast, have a nice complex salad with lots of olive oil for lunch, and a steak with stir fried vegies for dinner” it really doesn’t sound so bad, does it?
Another idea in the book is to precommit to the plan so it doesn’t take much energy to carry it out. I just know I’m going to pull out the skillet, chop up some sweet peppers and spinach, stir fry them in butter, then stir in two eggs scrambled with a tablespoon or two of cream for breakfast. The thought of pancakes or cereal just doesn’t enter my mind. I eat a big salad at the hospital cafeteria for lunch.
Try to turn your change from an “I won’t eat carbs” to an “I will eat moderate protein, fat, and vegies.” it will be much more effective for you.
Great advice, Jim.
Outstanding explanation thank you.
Thank you, Danny. And thanks very much for the kind mention on your blog.
Hey Peter
Another epic blog post, I need to set aside a lot of time to go through your posts, but the time is definitely worth it.
As well as experiencing a fairly euphoric state in ketosis, I also find that I can perform endurance type activities better. I haven’t done any distance running for ages, concentrating on sprints more these days, but the other day, as a warmup for the sprint, I ran a little further than usual. I had more lightness in my step, I didn’t puff the way one usually does at the start of a warmup, and decided yto extend the run.
It was great, felt light and fast, not the plodder I was. This is not just down to a KD, but I feel much steadier and up for a challenge eating this way. I also run some group kettlebell classes each week, and do fairly high intensity work on a ketogenic diet.
So it works well for me.
Interesting to hear, Steve. I wish we had data to know why some, like you, respond well, while others do not. Are there genetic differences? Are there differences in implementation? Is it all about allowing for enough time to adapt?
I too have unlimited energy on my long daily bike rides, am faster, and even push harder for longer. I go out and want to push to a heart rate of 150-172 or a speed of 20-23 miles an hour (I’m 56 years old) and stay there indefinitely. Now that I’ve been keto for 4 months I have my anaerobic push back too and can hang on in the sprints better than two months ago. Before I was tired all the time and had to work to get into a 130 heart range. This diet has freed me from fatigue completely.
Is it the reduction in glycogen usage so it goes further and a higher percentage at all efforts is fat?
Is it hopping off the insulin roller coaster? I had fasting glucose levels of around 100 on several annual physicals (of course with no discussion about it not being ok).
I have hypothyroidism and feel great on this diet. My energy is perfect so I don’t think my T3 has tanked. And of course my mind is clear and mood so much more stable.
I’ve researched Stevia though and only read it having a positive effect on blood glucose (pure extract). My glucose levels tend to be 100-115 after eating. Could stevia be affecting BG?
What is a normal 1 and 2 hour post prandial BG level?
These posts are great! It’s so nice to see detailed analysis instead of hand-waving rhetoric. And it’s refreshing to see an honest account of what we do and do not know, and how certain or uncertain it is. Science is murky at the edges of discovery, and I like to get a feel for where we are in the fog.
Thanks, Philip. Before this series is over I hope to debunk a few other myths and, for those interested in pursing NK, try to pass on all I’ve learned on the practice.
Hi Peter:
Please thank Dr. Phinney for the quick reply! So kind of him.
“many young adult female subjects in metabolic ward studies who uniformly maintained nutritional ketosis”
And that’s the rub, isn’t it? Most women on this diet are peri- or post-menopausal; some may be younger, but have PCOS. It’s interesting that altho’ most people who low-carb are middle-aged females, there is almost no research on them.
What’s the bias here Peter? Do you know? Why no studies on PCOS or peri-menopausal women? Anyway, thanks for asking Dr. Phinney and thanks for the update.
Peter –
I am still trying to grasp all the biology behind ketosis. So, I hope this question won’t seem ridiculous in light of what you have written. Most of what I see addressed with regards to ketosis is aimed primarily at men. I seem to slip more easily in and out of ketosis – despite a generally consistent extremely low carb and moderate protein intake, during certain times in my monthly cycle. I was hoping you might be able to address any differential impact of male vs. female sex hormones on ketosis. Moreover, I wonder if prolonged metabolic derangement (as a result of a very low-fat/high carb lifestyle accompanied by obesity for many many years), might also impact the ability to sustain ketosis differently for men and women. Thank you for your work in this area and the support you offer so many of us.
Risa, not a silly question at all. I must admit my ignorance, though. I have heard this before from women in ketosis, but I have not seen literature on it. I guess the question I’d have is why? Certainly catecholamines impact ketosis, but I’m less clear on the role of sex hormones. I’ll try to look into this.
Hi Peter,
“have not seen literature on it”
Ask Dr. Phinney. He’s actually quite expert in this part of women’s health. It’s my understanding he’s researched this for a company, but has yet to publish about it. I was stunned by for example when he said that menopause is an inflammatory process and that your state of inflammation determines when it hits. This may also explain why some cultures, like the Japanese, don’t/didn’t used to experience menopause (very low inflammation diet).
Yes, I sent Steve and Jeff (Volek) an email immediately after receiving this comment. Look forward to hearing his thoughts. If anyone knows, it will be Steve.
UPDATE: Here is what I heard back from Steve:
Peter –
To my knowledge, there is nothing in the peer-reviewed literature that answers this question.
That said, I have had many young adult female subjects in metabolic ward studies who uniformly maintained nutritional ketosis as long as their diet was strictly controlled in an “extremely low carb and moderate protein” range (aka less than 30 grams of carb and no more than 100 grams of protein per day).
In addition, we have done weekly ketone analyses on over 6000 clients in outpatient low carb clinics and did not stumble upon an a priori connection between low ketones and late luteal phase.
What we did observe is that women with marginal ketones seemed to be more susceptible to pre-menstrual cravings (which of course nuked their ketones).
Perhaps your blog reader might want to objectively test her ketones as you did. It might be instructive to see if her daily average blood ketones through her follicular phase is maintained above 1.0 mM but then falls below this threshold in the luteal phase despite maintaining the same diet.
Risa,
I’m having the same issues regarding ketosis during
the luteal phase of my cycle, and so frustrated at the
lack of information out their:( I function beautifully
on low carb all month and like clock work, as soon as my
hormones shift & serotonin drops….theres a breaking point
in which my body becomes desperate for a carb fix…if I give in
PMS symptoms increase exponentially (besides the immediate gratification of
the serotonin fixes) If I don’t give in and stay on low carb I become very irritable
and anxious (though overall pms is not that bad)…Peter I’d love your insight in the correlation between ketosis
and serotonin production …does ketosis possible lower the need for serotonin? Or is the lack of insulin (to shuttle tryptophan ) a sign that females may need to temporarily shift out of ketosis when serotonin levels drop
due to hormonal cycle?
Best Regards!
Risa, Lila,
I am having the exact same issues.
Thank you for bringing this up. I too am having issues with going in and out of ketosis with a very consistent low carb/moderate protein and fat diet. My husband is eating the exact same things and has always had a high ketone count, whereas I have always remained on the border, fluctuating relatively with my cycle it seems. I would love an explanation why.
And thank YOU Peter for all of your research and reiteration of material in a way that us less rigid people can understand. I am most certainly not a biology or chemistry expert (total opposite actually), and though I have a tough time with understanding some of the terminology, I was able to get the gist of the process far better than any other explanations. You’ve really made an impact on many lives, I’m sure. Again, Thanks! 🙂
Glad it’s helpful, Janet.
Thank you most kindly for the two huge posts on ketosis. Despite both my degrees saying science on them, this reminds me why I dropped biochem at the first opportunity!! I’m nowhere near the limits of anything in terms of output nor endurance – rather I’m using a state of ketosis for managing a medium rate of weight loss (123 pounds in 18 months). In peak summer season it allows me to do 2+ hours of biking/swimming per day without extra bullets of sugar or carb loading or any of the other ‘proper’ geek routines.
My question / suspicion is around the long term effects of ketotic states. Assuming that one has kept the plane of nutrition at or above adequate in macro/micro nutrients, AND, given the seamless entry point into the Krebs cycle, I see no issues why long term ketotic states should cause issues unto themselves. YES – if you’re limiting carbs or calories or whatever to the point where micro’s start to fall off the table — but that’s a problem with the ration balance as opposed to the energy cycle. Truth or Dare?
Many thanks. Enjoy reading your posts. LOVE the summary points in the earlier posts!
Meghann
Wow, Meghann, that is some profound weight loss and impressive physical activity.
Loving the detail you put into these!
So, something I’m seeing some LCHF detractors start to bring up is how a high-fat diet will also make you fat through some mechanism I know too little about…acylation stimulation protein, or ASP. Do you have some information somewhere on your site regarding ASP? I don’t have enough understanding of ASP to give a retort and unfortunately, ASP is the acronym for “Active Server Pages” so searching on that is pretty useless. Plus I don’t yet know who’s analysis to trust.
Anyway, what these people seem to be trying to say is that “well, sure LCHF has certain effects on the body, but really, they’re just switching one fat-building mechanism (insulin) for another (ASP) which also stimulates VLDL creation which is unhealthy”. Just wondering how to respond?
This issues has been addressed by the folks who studied it for a living, including Alan Sniderman at McGill (who I know personally, and who sits on NuSI’s scientific advisory board), Katherine Cianflone at Laval, and Keith Frayne at Oxford. The following link explains part of the story:
https://slowburnfitness.com/fat-regulation-insulin-or-asp/
Peter, your diet seems to be high in fat and cholesterol. I am 37 y old physician an have IIA type hypercholesterolemia with baseline LDL 300 and low HDL. I’m on lipitor 80 and zetia 10. My BMI is 28. I do not exercise much and eat what I want. I eat pita bread daily. Bad genes as both parents with CAD with dad’s first MI at age 39 (still alive at 66 now) Do you think your diet will be good idea for someone like me? I appreciate any help.
Doesn’t sound like what you’re eating now is optimal.
Peter
An excellent if somewhat disconcerting trip down memory lane (it is amazing how much of Physiology 101/202 you forget) I can only echo the sentiments of others in hoping that this series of articles settles down much of the chatter of internet warriors and other pervayors of broscience. It really should be compulsory reading for anyone who either professionally or recreationally has an interest in nutrition and its role in health.
I have been flirting with NK for awhile now and all the usal caveats of N=1 apply. But as a lifter I have my top end power has dropped off by a bit. As you would expect my capacity for work has improved but that vital bit of grunt at around 1RM has slipped.
I dont have enough experience to know whether this is courtesy of a period of accommodation that will pass or whether other lifters who take the NK road have found something similar.
Thanks again for the does of nutritional sanity…..
PS: I am have no doubt you are aware of this in the recent JAMA – https://jama.jamanetwork.com/article.aspx?articleid=1555133
Interesting point. Have you tried supplementing with creatine to bridge the gap? 1RM is largely driven by this system, so I wonder if that would make a difference? I have seen the JAMA paper, but have not read it yet.
I was very interested in reading the comment about ketosis in women. When I first started I could stay in ketosis as long as I was under 50 grams of carbs/day. Now, 9 months later it seems to be closer to 25 grams. During the last 6 months I was only able to reduce my H A1c from 5.9 to 5.8 and my body fat stayed the same at 23%. I exercise at least one hour/day, often 2 hours. What’s my chance at this point to improve my insulin sensitivity and reduce body fat. My protein levels are rarely over 80 grams/day.
Well, darn. I was hoping for smoking gun saying stating that NK would expend more energy. I’m competitive amateur cyclist at 14 percent (water dunk) body fat with 3 kids and a full time job, so I was hoping NK would help me to the holy grail of a sub 10%. After 4 weeks of LCHF and the latter 1.5 weeks at solid NK I have not dropped a single pound. I think I’ve gained 2 or three pound. Of course, so many variables: new winter activities such as weight lifting, XC sking during the same time. Bottom line for me though is that it does not seem to affect fat loss or overall weight loss. I probably need to go longer with NK, correct? I do have a better spread of energy throughout the days on NK, and I really enjoy the much reduced hunger at meal times too. I also dig not needing the gels on long endurance rides and skis.
Talyor, don’t give up on NK yet. At least wait until I finish this series before you make your decision. We’re barely half way there, and there’s lots more to discuss.
I have been keto-adapted for the past 12 weeks and I will say that it was quite tricky to get there. It wasn’t a simple matter of just not eating carbs. I really had to up the fat and tone down the protein. Using a blood ketone monitor was essential (yes, it is expensive). I also find it is easy to temporarily drop out of ketosis, but not so hard to find your way back. When I am keto-adapted, I note a very distinct difference in how I feel. It is a sort of a mellow feeling and my energy level seems to be much more consistent and stable throughout the day. Then, at around 10, I crash and sleep very well. I don’t know if this is how it is with others, but, for me, this is a big benefit.
This sounds pretty typical, Sam, at least for the folks I know well.
Peter, your work is so fantastic and you and Phinny/Volek and others have transformed my approach to fitness (cyclist) and health. I can not follow all the science but get the idea of what you are talking about when you re-cap the essence of the post. I have been low carb for awhile and am now going keto to loose weight for spring road rides…
I have more energy…my head and CNS are less anxious and my sympathetic nervous system is no longer on fire…
Can you give some symptoms of keto adaptation ( do not have the meter to read this) so people can have some idea without the meter/science to verify?
Thanks
Hmmm, hard to talk about symptoms of adaptation other than to note the absence of symptoms from not being there (e.g., lethargy). At very high levels of ketosis (typically over 4 or 5 mM), some people report euphoria and loss of appetite.