
Paul Offit is a pediatrician specializing in infectious diseases and an expert in virology and vaccine development. He currently serves on the FDA committee evaluating COVID-19 vaccines. In this episode, Paul’s second appearance on The Drive, he provides an update on all the SARS-CoV-2 vaccines currently deployed, explains why the concerns raised around the mRNA vaccines are not legitimate, and offers his view on the prospects and timeframe of reaching herd immunity. He also takes a deep dive into immunology, explaining the short-term and long-term immune response to both natural infection and vaccination and how these two can function together to provide durable immunity. Additionally, they discuss the theories on the origins of this virus, what impact the new COVID-19 variants might have, and the recent pausing of the J&J vaccine. Finally, they discuss how we can be better prepared for an inevitable future outbreak of a novel virus. This episode was originally recorded on April 14, 2021.
Subscribe on: APPLE PODCASTS | RSS | GOOGLE | OVERCAST | STITCHER
We discuss:
- Overview and current status of the SARS-CoV-2 vaccine strategies [4:10];
- Addressing concerns about mRNA vaccines [9:00];
- How the failure to make an effective HIV vaccine aided the development of a COVID-19 vaccine [16:45];
- Where SARS-CoV-2 falls on the spectrum of its ability to mutate and what that means for immunity and vaccination [21:30];
- How the combination of short-term and long-term immune response to SARS-CoV-2 work together to provide durable immunity [28:00];
- Importance of understanding relative vs. absolute risk reduction [38:15];
- Implications of pausing the J&J vaccine due to reports of blood clotting in the brain [42:45];
- What constitutes herd immunity and the concerns of rising vaccine hesitancy [47:45];
- When we might reach herd immunity, future vaccines for children, and long-term outlook for maintaining population immunity [58:45];
- Theories about the origins of SARS-CoV-2 [1:07:00];
- Preparing for the possibility of a future pandemic and how we can learn from our mistakes [1:10:40]; and
- More.
Overview and current status of the SARS-CoV-2 vaccine strategies [4:10]
This interview includes a discussion of several different kinds of vaccines. Here is an overview of the various types of vaccines:
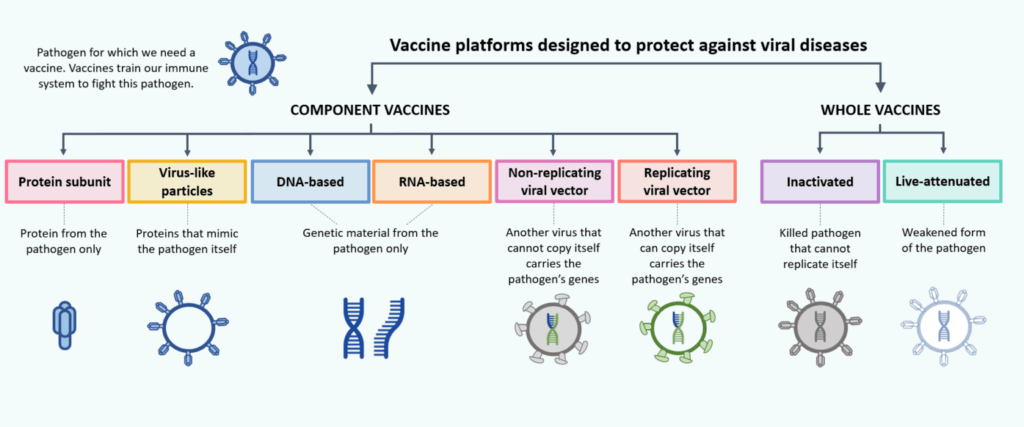
Figure 1. Overview of vaccine types. Image credit: McGill University COVID19 Vaccine Tracker
- Tens of millions of people have now been vaccinated against SARS-CoV-2
Specific types of SARS-CoV-2 vaccines
- Messenger RNA (mRNA) vaccine
- Adenovirus vaccine
- Purified protein vaccine
- Live attenuated virus vaccine
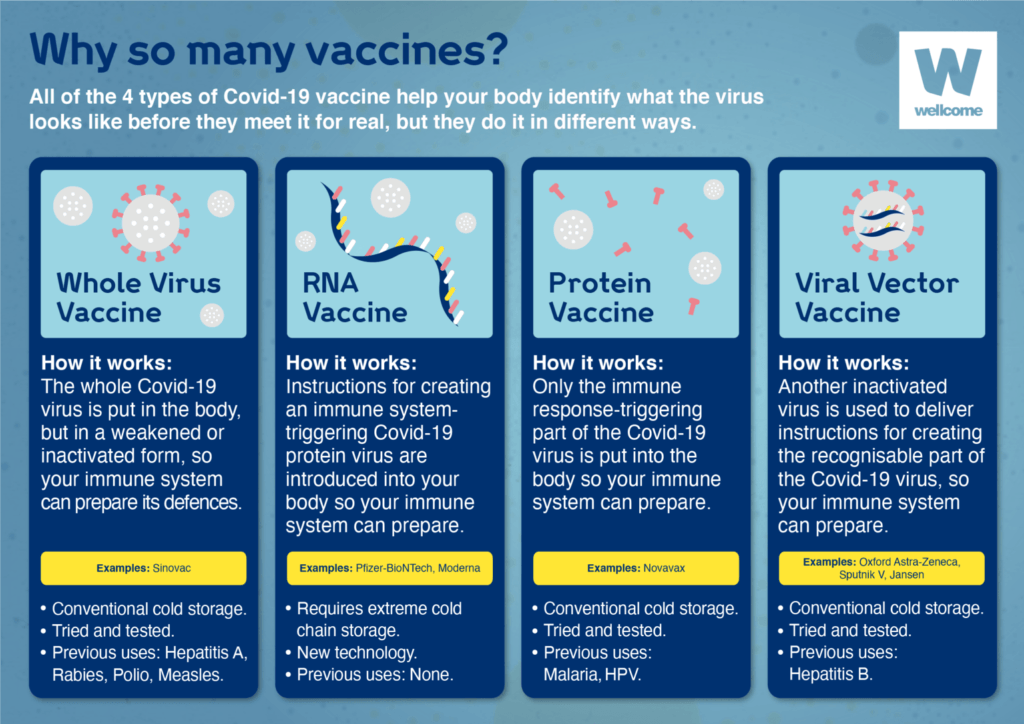
Figure 2. Types of COVID-19 vaccines. Image credit: Wellcome
- 1) mRNA is the farthest along in the US
- FDA granted EUA to Pfizer on Dec 10 and Moderna on Dec 17
- 120 million have received at least one dose of one of these
- 2) Adenovirus
- Uses adenovirus as a vector to deliver viral DNA
- Jenner Institute/Astra Zeneca (AZ): replication-defective adenovirus vector
- Tens of millions of AZ in UK and Europe
- Janssen / Johnson & Johnson (J&J): replication-defective adenovirus type 26
- 200K in west Africa for Ebola
- more than 6 million in US for SARS-CoV-2
- 20 million + doses of these vaccines
- Russian vaccine is also a replication-defective adenovirus vaccine (human Ad26 followed by human Ad5)
- 3) Purified protein
- Made by Novavax
- insert gene for spike protein into baculovirus
- grown in Spodoptera frugiperda cells (same way we make Flublok)
- Novavax has been slow to get approval
- 4) Live attenuated
- still in the works
- Paul doesn’t think one has been approved anywhere
- 5) Whole killed viral vaccine
- Used in China on 10+ million people
- Similar to how we make vaccines for polio, rabies, Hep A, etc.
- some question how well it works against SARS-CoV-2
- Whole killed virus was first used in late 1800s by Louis Pasteur against rabies
- The first vaccines were live non-human viruses
- Used cowpox in late 1700s
- The virus was close enough to human smallpox that produced immune response
- but they didn’t understand the science behind it back then
Addressing concerns about mRNA vaccines [9:00]
- People say mRNA is experimental and like science fiction
- Peter has tried to point out it’s not as experimental as people think and has been around for decades
- See Peter’s newsletter: mRNA vaccine technology
- Now is just the first time we did the final step of sequencing and putting it into clinical practice
- Peter has tried to point out it’s not as experimental as people think and has been around for decades
{end of show notes preview}

Paul Offit, M.D.
Dr. Paul Offit is a pediatrician specializing in infectious diseases and an expert on vaccines, immunology, and virology. He is the co-inventor of a rotavirus vaccine that has been credited with saving hundreds of lives every day. Offit is the Maurice R. Hilleman professor of vaccinology, professor of pediatrics at the Perelman School of Medicine at the University of Pennsylvania and director of The Vaccine Education Center at Children’s Hospital of Philadelphia (CHOP). Dr. Offit is currently a member of the National Institutes of Health (NIH) working group on vaccines, a subgroup of the Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV) project that is planning a strategy to combat COVID-19. He is also a member of the FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC). Previously, he was a member of the Centers for Disease Control and Prevention’s (CDC) Advisory Committee on Immunization Practices. Dr. Offit is a board member of Vaccinate Your Family and Autism Science Foundation and the author of eleven books.
Website: paul-offit.com
Twitter: @DrPaulOffit
Facebook: Paul Offit




Amazing vaccine content recently, I’ve really appreciated these. It helps when I need to answer questions for my friends who don’t dig into this stuff. Thank you Peter for doing these, you are a tremendous host! I look forward to your fantastic show every Monday!
Dr. Attia,
My wife and I just finished listening to this very interesting and informative podcast. Thank you for producing such clear and helpful material!
I do have a question regarding the risk of harm from the AstraZeneca vaccine vs. the virus. Let’s take the numbers as used during the podcast for the risk of developing a blood clot from the COVID-19 virus vs the COVID-19 vaccine:
Risk of dying from a COVID-19 virus infection: 1,850 in 1 million (case fatality rate)
Risk of suffering a fatal blood clot from the AstraZeneca COVID-19 vaccine: 1 in 1 million. (case and crude fatality rate)
From those two numbers, it is clearly overwhelmingly safer to be vaccinated. However, whereas 100% of the vaccinated population is vaccinated, less than 100% of the unvaccinated population will be infected by COVID-19, causing a difference between the case and crude fatality rates. Or, is COVID-19 so contagious that it is correct to stipulate that 100% of an unvaccinated population will eventually contract the virus?
However, even given that, it seems that it would require only 1/1,850 of the unvaccinated population (540 individuals of 1 million) to be infected by COVID-19 in order to equalize the risks.
I find this type of discussion both fascinating and confusing, and so appreciate the time you and others spend to educate the public.
Sincerely,
Dan.
Thanks for all the excellent content Dr. Attia. I’m curious if you could expound on your cancer screening MRI protocol. Specifically, how often is “every once in a while?”
Best,
Chris
Really, another one-sided Offit interview. Certainly would have appreciated a discussion of the censorship that is ongoing if one dares to question this narrative. So much of this entire year reeks of fear-mongering and shaming. How many whoopies have you seen from FDA-approved, supposedly unbiased researched medications and devices? How can you purport to hold unvaccinated individuals responsible and accountable for the spread of this disease when a manufacturer makes millions for the company and shareholders and is 100% financially harmless for the “few” who have side effects. Grand experiment sanctioned by the government seems to be supported by many who will gain more of the wealth. Are facts, cold hard, cold-hearted facts being openly debated in this grand experiment? Draconian lockdown, medical freedom denial, inability to travel freely, and censorship have my common sense radar focused on something that just does not feel right…
Agreed. And I am under the impression that you can still spread the virus even if your vaccinated?? Paul discusses Michigan having 65-70%of the population vaccinated and had a surge of covid cases….paul states the vaccine seems to be working due to the death rate but clearly its spreading with vaccinated people…..so if your going to promote vaccinations to stop the spread, you have failed to deliver a vaccine that does that….please correct me if I’m wrong….
I believe the biggest question people have regarding mRNA, which you don’t seem to cover, is can the immune response to the proteins (i.e. the spike protein) made by the mRNA create an autoimmune response to a similar series of proteins in the future that are non-virus proteins.
To win hearts and minds, it would be good to address the main concerns that people have about these vaccines. For example Antibody Dependent Enhancement, a potentially longer-term effect for which the FDA has acknowledged the risk “remains unknown” and which people in the clinical trials and the public are not being informed about. Or the systematic de-prioritization and suppression of a long list of very low-cost prophylactics with established safety profiles that might have saved many lives and brought the emergency to an end a long time ago, without the fragility to new variants that the vaccines may have; see for example Dr Kory’s recent review of ivermectin in the American Journal of Therapeutics reporting spectacular results in those regions of various Latin American countries that distributed it https://journals.lww.com/americantherapeutics/Fulltext/2021/00000/Review_of_the_Emerging_Evidence_Demonstrating_the.4.aspx Likewise the Oxford University RCT that found that the steroid budesonide reduced hospital admissions by 90% https://www.thelancet.com/journals/lanres/article/PIIS2213-2600(21)00160-0/fulltext Another concern that people have, is that these vaccines often have relatively severe short-term side effects and they have a large number needed to treat to prevent even one mild symptomatic case. Given that, you might hope to see an RCT of all-cause mortality in frail elderly people from date of vaccination, to confirm that the vaccine is on balance beneficial for that group; this something that as far as I know has never been done.
My thoughts exactly! It is heartbreaking that there is such obstruction of therapies that work when a person is already ill with covid, and that from prestigious organizations. They have done nothing but lose my confidence in them. I listened to this podcast even though Dr Offit is associated with the FDA. Not his fault that I lost confidence in these institutions by the way they treated physicians like Dr Kory who are DOCTORING and see with their own eyes therapies that WORK.
Wow! I was listening to this podcast as I like to hear all sides of an argument, but then you went full Dr Mengele fascist on us. Segregation of society – really?! And nothing will make people more suspicious than mandates and going after children – it’s not like there isn’t a long history of drug companies, doctors ( diet heart hypothesis) and governments getting things wrong, is there?
The NNT will be different for different age groups and those with or without comorbidities – I thought you were a proponent of individualised medicine?
Who’s to say this virus isn’t going to be bad for a couple of years and then settle down to be endemic like the 4 common coronaviruses that we have – there’s a theory one of them was the ‘Russian flu’ of 1890 ( not sure about the year).
We have never blamed, or dreamt of holding accountable, people with flu ( or any other respiratory infection) for incidentally infecting others around them in their daily life. If I was immune compromised I would keep myself away from others as best as possible, but I wouldn’t expect the world to stop for me. Life is full of risks and for living to the most every day. Some people choose to go sky-diving, I don’t- we all choose what level of risk we’re prepared to accept.
‘Long’ disease ( children or adults) is unfortunate with this infection, but it is not unique and I have not seen evidence that it is more common. Perhaps we would do better to investigate why some people suffer such adverse outcomes and what in their environment ( food etc) may be affecting this. In that way we would make everyone healthier and less likely to suffer from other modern diseases as well as from any future infections that come along.
The asymptomatic transmission idea has been all but disproven ( presymptomatic is possible though not as common as suggested), masks in the population have no effect on any country/ state graph and there was 20 – 40 years worth of papers proving this up until 2020 when a lot of the ‘science’ was removed from easily findable sources on the internet. Social distancing has just been disproven – ventilation indoors is important.
The worst thing for me has been discovering how many Milgram experiment and Asch experiment people there are in the world. Integrity, respect and compassion are principles that led me to a career in medicine, but it seems that’s not true of a lot of doctors.
are you an Anti-vaxer maybe? against MMR requirement???
re “We have never blamed, or dreamt of holding accountable, people with flu ( or any other respiratory infection) for incidentally infecting others around them in their daily life. If I was immune compromised I would keep myself away from others as best as possible, but I wouldn’t expect the world to stop for me. Life is full of risks and for living to the most every day. Some people choose to go sky-diving, I don’t- we all choose what level of risk we’re prepared to accept.”
so, your kind of (selfish rights) people are also against every state requiring you have a certain amount of minimum car accident liability policy coverage? doesn’t that infringe of you God given human right to drive like Mad Max on public roads and make someone else pay for it?
I still want to keep my freedom for medical choice. I am retired Med Tech and researcher. Our freedoms are gradually being taken away. By the way I did get vaccinated.
Why no talk about this, one of the most major concerns? Cherry picking as always sends us further back
These papers discuss the science of Antibody Dependent Enhancement & Viral Interference.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7311339/
https://pubmed.ncbi.nlm.nih.gov/33113270/
https://www.nature.com/articles/s41564-020-00789-5
https://pubmed.ncbi.nlm.nih.gov/31607599/
https://peerj.com/articles/10112/
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0035421
https://insight.jci.org/articles/view/123158
https://pubmed.ncbi.nlm.nih.gov/18941225/
https://pubmed.ncbi.nlm.nih.gov/17194199/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7142689/
…Possible serious adverse effects from the covid vaccine which may not be seen for a few years…
The British Medical Journal …..as an example…
‘… The mRNA might even reach delicate cells or places that we don’t want them to, such as neurons in the brain or spinal cord.’
‘… As a result, brain cells that express the spike protein might be marked as foreign by the immune system. For example, cytotoxic T-cells, which kill virus-infected and cancerous cells, might see the spike protein-expressing brain cells as a threat. Unlike muscle cells and many other cell types, neurons in the brain rarely regenerate.’
‘… Jacob Wes Ulm, MD, Ph.D., a geneticist, explained this concern in detail in a letter to the British Medical Journal, as well as in a public comment to an article about mRNA vaccines on January 2021:
…it seems that they [mRNA vaccines] can enter a much broader tissue range compared to even attenuated virus vaccines…And since the mRNA vaccines would induce SARS-CoV-2 viral spike protein expression, that seems to mean that people who get the mRNA vaccines are going to have a much greater range of cells and tissues vulnerable to cytotoxic [T-cell] attack…with side effects that may not manifest for years (with cumulative damage and chronic inflammation).’
https://www.bmj.com/content/372/bmj.n627
Thanks for this informative comment. Given the current status of the vaccine debate and the fact that COVID vaccines were the main focus of this podcast, I was also very surprised that Attia did not get into these topics with Offit. Instead we got debunking of the most scientifically illiterate objections (that the mRNA will permanently alter your genome). Probably not that useful for listeners of this podcast. The cherry-picking left a bad taste in my mouth.
Goes to show that you really need to find the smartest advocate for the other side you can if you really want to give undecided audience members the best possible scrutiny of the issue.
Peter, please bring on someone who doesn’t already agree with you 95%.
The technical discussion with regard to the virus was excellent however at the end the podcast it started to sound like it was a religious discussion and you were both priests!
To win hearts and minds all that was needed was to provide a deactivated virus vaccine along with the new technology. The Chinese we able to manage it. Even if it is lower efficacy (due to it’s lower mucus response, as people will no doubt need to argue) it would have been widely trusted by the community even if it took multiple doses.
Current vaccines are held in suspicion by the community through the absence of a deactivated, or attenuated, virus vaccine choice. Remember the only reason there has not been a deactivated coronavirus vaccine approved in the past (MERS and SARS1) is because there was no animal model testing that could be practically completed (smaller animals that were severely impacted by coronavirus and could be used for testing the vaccine). That is also, supposedly, why Iowa State University and others funded the “Mouse-adapted MERS coronavirus” trials that succeeded in mutating MERS up to 22 times in humanised (hDPP4 knockin) mice to create a MERS that was capable of producing lethal lung disease hosted by knockin mice, in 2017. However after producing such a dangerous, cruel and irresponsible virus, in my view, for testing the deactivated vaccine, the animal models were completely bypassed in 2020. Now we still have no approved deactivated coronavirus vaccine but we have a virus that can be hosted by mice and causes lethal lung disease in mammals with human exons.
As an aside; if I am to be responsible for other people’s health then can I have a say about how they should be responsible for their own health? It appears that the lives of the misfortunate and their access to medicine are being burdened by people making avoidable severe unhealthy choices.
As usual, very much enjoyed the information. One thing that seems to be missing, though is why can’t I take off my mask once I have been vaccinated? (Actually, I had COVID in November, and then got vaccinated in March). From all that I have read, once vaccinated, risk of infection AND transmission to others is ridiculously low. So, why can I not return to 100% normal life after vaccination? Since there is no such thing as 100% protection/risk elimination (for anything), why do I have to continue living as if I never got vaccinated?
From day one, in a very crafted, polarizing narrative—you have pushed the vaccine. Now , you are inadvertently pushing for mandates thus crossing my line in the sand. Intrinsic , universal values are sacred!
Because of the irresponsible campaign, I watched my young nephews line up for the jab, unnecessarily, not knowing the long term consequences.
My daughter and grandson have had covid , mildly. More less they will be forced to get an experimental vaccine that’s killed hundreds which you don’t talk about. And Memphis probably lost a young surgeon to the vaccine. And I understand that it potentially could save millions of lives:
But a blanket roll out of an experimental vaccine for a virus that kills less than 1 percent?
And making light of the gain of function research?
Not providing the pertinent data ( animal studies) for pregnant women?
The excessive transgressions of the for- profit pharmaceutical corporations? Their censorship? Their tyrannical control?
And their corrupting $$$$…
Caution and skepticism and time have been thrown to the wind for an ideological crusade.
100% agree
Great podcast like always and I agree with a lot of what is said, but seems to be an echo chamber at this point. Bring RFK Jr or someone like that for a counter point of view. If he is so wrong, then you shouldn’t have any problem showing your audience that.
I would be very interested in that conversation! Or a conversation with Dr Robert Malone, or Dr. Peter McCullough. Searching for a balanced dialogue. It’s so hard to find.
There are other types of vaccine risk which can take quite a while to appear. If for example a vaccine is “leaky”, that’s to say it protects against symptoms without preventing transmission, then it can cause the pathogen to become more virulent over time. An extreme example is Marek’s disease, which in the early 1970s was a relatively mild disease of chickens but after widespread use of a leaky vaccine the fatality rate in unvaccinated chickens is now 100%. Do we know yet whether the COVID vaccines prevent transmission? If they do turn out to be leaky, then it may be safer to be around unvaccinated people (because if they fall ill they will have symptoms and stay home) than vaccinated people.
In some parts of the world that prior to vaccination had few or no COVID deaths, there have been large and odd-looking steep spikes in COVID deaths immediately after vaccination campaigns started; Gibraltar was the first, and at the time we accepted it as an odd coincidence, but since then we’ve had Seychelles and other South Asian countries: Bangladesh, Mongolia, Thailand, perhaps even the recent Indian spike although it’s harder to know what to make of that. We’ve seen something a bit similar reported in the UK but against a far noisier background of endemic infection; to give one example of many, this study https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/982499/S1208_CO-CIN_report_on_impact_of_vaccination_Apr_21.pdf found “an abundance of patients admitted to hospital within 7 days of vaccination”. Correlation is of course not causation, as we have to keep reminding lockdown advocates, but it is troubling and if something like this had happened following use of say, ivermectin, then we know it would have been used to ban it. The usual official explanation is that newly-vaccinated individuals have let down their guard, although mobility data don’t support this.
With the assumption that 80% vaccination + natural immunity = Herd Immunity, what are the metrics to watch to determine if this is true? Hospitalizations? Deaths? New Infections?
Hi, as a physician, I am really interested in calming the hysteria about the vaccine. BUT I have a molecular biology point to consider:
So called “Line-1” DNA is presumably ‘ancient’ retroviral DNA in the human genome and accounts for a large amount of DNA (? as much as 17% in one article I read reviewing it). Reverse transcriptase can be found among these remnants in our DNA. That doesn’t mean it is constitutively TRANSCRIBED (though really, do we know either way?).
We have transposons and retrotransposons, jumping genes, and they are able to transcribe and then reintegrate. Am I misinterpreting the biology of retrotransposons? Don’t they transcribe, then reverse integrate? If so, then isn’t it plausible that OTHER mRNA can use this as a means to re-integrate into the genome? I know the nuclear membrane is tightly controlled and that mRNA (?presumably) is a one-way transit OUT of the nuclear envelope. But, is it?
I am not an ‘anti-vaxxer’ (sp) at all — but when you dig in with the biology of it, maybe the reality of it is not so clear after all. So, possibly it is not quite correct say to patients, “there is absolutely no way that this mRNA can get ‘into’ your DNA” ?
You ask, “I know the nuclear membrane is tightly controlled and that mRNA (?presumably) is a one-way transit OUT of the nuclear envelope. But, is it?” Yes, it is: the nuclear envelope is a very strong barrier, and almost nothing can get in without a nuclear access signal — which mRNA lacks. Imagine what an inefficient mess it would be if every gene transcript could drift back into the nucleus instead of being used to make protein!
And what else could it do there? There’s no ribosomes inside the nucleus, so it can’t make protein. And there’s no way for it to integrate any genetic material into the nucleus, because it’s RNA, not DNA, and has no reverse transcriptase to convert it. And if it DID somehow create a paired nucleic acid sequence to form a DNA sequence, it would still need or an integrase to insert itself into DNA — which it ALSO doesn’t have. So it’s a non-issue.
It was pretty shocking when the jump came to manadory vaccines including kids. Even in the near future.
I’d like to believe everything is up & up, that the vaccines are good but I am more confident in my belief to manage my own health.
Government in my opinon hasn’t earned my trust when so much money & power is to be gained. Makes me wonder how far I’d have to go to resist, it”s now becoming a matter of principle.
great podcast! very informative and timely. thanks!
QUESTION: Does anyone know what is the absolute risk reduction of the mRNA vaccines if only one does is ever taken? That could be a critical question if many people skip/avoid the 2nd dose (esp. young ones, or those worried about wide spread anecdotal reports of much higher rate of greater symptoms/reactions on the 2nd dose). Hopefully, those experiments were done and data is known.
Very good question! How about a discussion of the absolute vs the relative risk reduction in regard to these vaccines?
Dr. Attia,
Can you (and/or other subject matter experts) address the warnings made by Dr. Geert Vanden Bossche regarding the unintended consequence of immune escape caused by mass vaccinations during a pandemic? He appeared on Dr. Bret Weinstein’s podcast recently to explain his hypothesis. As a layman, I have no way of backstopping his argument, but as Bret said, he puts forth a plausible warning. Is it possible to get an honest, objective, systematic assessment of his claims?
Thank you for your time. I appreciate your work.
Snopes (and some immunologists) got ya covered:
https://www.snopes.com/news/2021/03/26/geert-vanden-bossche/
Originally, I came here to leave a note of thanks to Peter and Paul for the podcast. However, after reading the comments, I’d also like to thank those folks for the follow-on conversations. The vast majority of the podcast and the comments are way over my head, but I appreciate them, nonetheless.
Unfortunately, as a layperson, I’m no closer to deciding whether or not to get the vaccine. Regular folks like me rely on experts to provide guidance, but, in the case of COVID-19 vaccines — more than I’ve ever experienced with anything else — there appears to be discord even among the experts. Or, perhaps I’m simply unable to identify the true experts. Certainly, that’s a great possibility.
Initially, my vaccine hesitation was due to my pre-existing health issues. I was concerned a vaccine may cause a worsening of existing symptoms or a relapse of prior ones. Now, the more I read and try to become better informed, the more uncertain I am about the possibility of new symptoms being introduced by the vaccine itself. It’s like being in mental quicksand.
One positive point, I suppose, is that I live alone and keeping to myself isn’t a hardship. In fact, I rather prefer it. Of course, when I do have to go out (to the grocery store), my presence does potentially impact others. I’m keenly aware of this. I always wear a mask, keep as much distance as I can (usually going 15 minutes prior to the store closing, as it’s almost always nearly empty), and use hand sanitizer and wash my hands. I realize there’s debate on these actions, too, but they’re not troublesome to me and I feel that doing something is better than doing nothing.
Anyway, back to the main point, I appreciate all the current comments and those that will likely follow. I wish everyone good health.