
Protecting your hearing is just as important to healthspan (the how-well-you-live part of longevity) as protecting your teeth, but I don’t think considerations about how to prevent hearing loss get enough attention. This WSJ article caught my attention because it outlines some recommendations toward protecting hearing (in kids). While it is important to raise awareness about noise exposure for young people, I think holding that the same level of awareness applies to adults, too.
Hearing loss can result from a number of factors such as genetics, complications at birth, chronic ear infections, and, most relevant for this discussion, the compounding effect of loud noises. Noise-induced hearing loss (NIHL) can occur from a one-time intense sound like an explosion or can more commonly occur from repeated exposure to loud sounds. The result is irreversible damage to hair cells in the inner ear. Located in a spiral-shaped bone found in the inner ear called the cochlea, hair cells convert sound waves into an electrochemical signal that is carried to the brain, producing what we perceive as sound (Figure 1). Here is a 30-second simulation of how different levels of sound exposure affects hair cells.
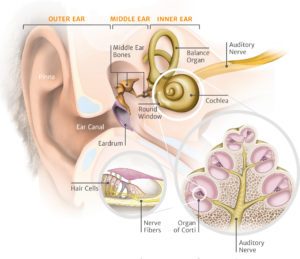
Figure 1. Anatomy of the inner ear. The cochlea pulsates the basilar membrane that contains sensory hair cells (inset) that move in response to the pressure created by the sound waves. Image credit: AudioCure
The effects of hazardous sound exposure accumulate over time such that it has the potential to be more damaging as people age (much like atherosclerosis). Indeed, results from the National Health and Nutrition Examination Survey, which uses point estimates to gauge the prevalence of NIHL, suggest that NIHL prevalence increases up to the fifth decade of life. The report estimated that about 13%, of the nearly 7,000 children and adolescents (between the ages of 6 to 19) surveyed, have permanent damage to their hearing from excessive noise exposure. In the population of nearly 3,600 people surveyed between the ages of 20 to 69, an estimated 17% have NIHL. While the prevalence of NIHL increases from early to mid-adulthood, it then decreases in adults that are in their 60s. The regression could be explained by the co-occurrence of age-related hearing loss (ARHL) in later decades, which is distinct from NIHL although is also the result of damage to hair cells in the inner ear and, similar to NIHL, also affects hearing at higher sound frequencies (think the highest note on a piano). Despite the overlap in clinical presentation, hearing loss in adults who are in later decades of life is attributed to ARHL and accounts for the much higher prevalence of hearing impairment in adults 65 years and older. The current understanding is that ARHL that occurs in later decades adds to NIHL (if already present), meaning that the total hearing loss in later decades is the sum of NIHL and ARHL.
The reason for my writing on this topic is that there is increased concern about NIHL in younger decades of life, namely due to the rise in recreational noise exposure from the likes of smartphones and portable music devices. The World Health Organization (WHO) projects that the uptick in recreational noise exposure puts over a billion young people at risk of developing hearing loss that ultimately impairs communication in daily life. With that said, NIHL is preventable but, as this kind of hearing loss can progress for years before it is perceived or diagnosed, NIHL prevention requires a cognizant approach.
Hearing damage from noise is primarily due to 3 factors: loudness of the sound, duration of listening, and the distance of sound input relative to the inner ear. As such, a strategy to avoid NIHL requires understanding what a “loud” sound means, tracking sound exposure, and choosing protective listening device options.
Many people would likely be able to approximate weight in units of pounds or kilograms, eyeball height in meters or feet, and even guess the temperature outside in Celsius or Fahrenheit, but guesstimating sound as a threshold value would likely be less relatable. Sound is measured in units called decibels (dBA). To give you an idea of the volume levels, I have included a Table below. The measurement of sound in dBA is based on orders of magnitude, a logarithmic scale rather than a linear scale. This means that a sound 10 dBA greater in comparison to another is 10 times louder, whilst a sound that is 30 dBA greater is 1000 times more powerful. For example, a phone ringing (around 70 dBA) is 10 dBA higher and 10 times louder than a normal conversation (around 60 dBA). A normal conversation compared to a quiet room (around 30 dBA) is 30 dBA greater and about 1000 times more powerful. The WHO has created guidelines for permissible daily noise exposures to avoid hearing loss (the guidelines include a useful infographic, copied here-below; Figure 2). According to the guidelines, there is no risk listening to sounds below 80 dBA, regardless of the duration. The guidelines propose that the daily recommended safe volume level stay below 85 dBA for a maximum of 8 hours per day, as sound levels above 80 dBA can cause hearing damage over long periods of time. And for every 3 dBA increase in volume, the amount of safe listening time cuts in half; that leaves you with about 28 seconds of “safe” listening time at a rock concert (assuming you don’t wear noise-cancelling protection like earplugs), as sound levels above 120 dB can cause immediate hair cell damage (Figure 2).
Table. Common sounds by approximate noise level, measured in decibels (dBA). Data adapted from The World Health Organization and The Federal Aviation Administration
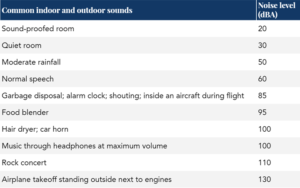
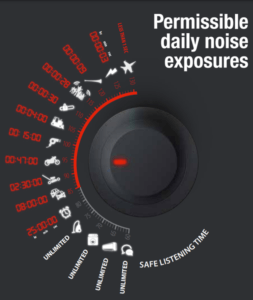
Figure 2. Examples of different sound levels produced by objects with the daily recommended safe listening time. Image credit: The World Health Organization
In order to monitor sound volume and duration in the past, someone would have had to buy a stand-alone decibel meter, but modern smartphones can run applications that measure ambient sound and can track and summarize listening volume. Here is a review of smartphone decibel reader applications for both Apple and Android devices.
In addition to monitoring noise exposure and tracking volume, there are noise protection options to consider. Here is a review of earplug technologies intended for concert listening, which reduce ambient noise without completely blocking sound altogether. EAROS ONE is one of my preferred earplug options, which have a 17 dBA reduction capacity (which, according to The WHO guidelines, buys me about 30 minutes of safe rock concert listening attendance compared to the measly 30 seconds I had without ear protection). When it comes to headphones, the name of the game is to use devices that provide high-quality sound without having to turn up the volume to negotiate ambient noise. Active noise-canceling listening devices use battery-powered technology that creates sound waves that cancel out ambient noise up to 15 to 20 dBA (the difference between 8 hours and 15 minutes of safe listening time). Here are two reviews of noise-canceling headphone options. And all things equal, over-the-ear headphones may be preferred to in-ear devices, which deliver sound directly into the ear canal.
Just as I train my body to be able to pick up my grandchildren, among other activities I want to do into late life (you can find my Centarinarian Olympic discussion archive here), I just as well want to hear them properly too (notwithstanding the few times I wish I could press the mute button on them). Aside from age-related hearing loss, avoiding NIHL is possible with awareness of risk factors: volume, duration, environment, the related appropriate ear protection, and the choice of listening device. With those factors in mind, someone can modify behavior to optimize for the ability to hear later in life.


Hi Peter. Avid follower of your content. Thank you for putting out such gem.
I have tinnitus for several years. Is there any medication that can treat damaged nerve cells? Or are there any hope for foreseeable future on tinnitus treatment?
Thanks!
Hi Peter
Thank you for high lighting the need for saving from noise induced hearing loss.
I am a recently retired Head of Audiology and I am very concern about the young kids.
I am happy to join any project you may have to help people with NIHL.
Feel free to reply if you think that is worthwhile.
Regards
Richard.
I appreciate info on hearing loss. What I don’t understand is why more research is not devoted to tinnitus. It is a horrible affliction that affects quality of life every day.
Hard to find ANY progressive research or strides made in curing it. Disheartening for many.
The American Tinnitus Association is a good place for research info and clinical trials https://www.ata.org/research-toward-cure/clinical-trials