
Stephan Guyenet is a neuroscientist focused on the neuroscience of obesity and energy homeostasis. He is the author of the book, The Hungry Brain and founder/ director of Red Pen Reviews. In this episode, Stephan explains how obesity has changed phenotypically over the course of human history as well as what might explain the dramatic increase in prevalence of obesity in the last few decades. He talks in depth about the role of genetics, the brain, and hormones like leptin play in the regulation of fat mass. He dives deep into two common theories of obesity—the carbohydrate-insulin model and the energy balance model and provides his take on which theory has stronger evidence. Additionally, he provides insights on how we’re hard-wired to think about food and the consequences of modern foods designed for maximal pleasure. Finally, he goes through the factors that affect body weight, set points, and provides takeaways for people wanting to take advantage of what we know about the brain’s role in regulating our body weight.
Subscribe on: APPLE PODCASTS | RSS | GOOGLE | OVERCAST | STITCHER
We discuss:
- Stephan’s neuroscience background and his focus on the nuances of obesity [2:15];
- How obesity has changed for humans throughout history [8:00];
- The association between obesity and adverse health outcomes, the “obesity paradox,” and confounders when relating BMI to longevity [14:00];
- The sharp increase in obesity across demographics [23:30];
- The hypothalamus and its role in obesity [30:00];
- The role of the hormone leptin in obesity [40:00];
- The genetic component of obesity [46:30];
- Understanding the tendency of humans to store fat through an evolutionary lens [57:00];
- The hedonic aspect of food, and how the brain reacts to modern, highly-rewarding foods [1:03:30];
- How we are hard-wired to think about food [1:14:30];
- A review of the “Carnivore diet” [1:21:45];
- The energy balance model, carbohydrate-insulin model, and unifying the theories around adiposity [1:34:15];
- Body weight set points: a hypothetical comparison of two individuals [1:41:45];
- Takeaways for people who want to lose weight and keep it off [1:48:30];
- Evidence that favors the energy balance model of weight gain [1:56:00];
- The synergistic effect of fat and carbohydrates and observations that a low-fat diet or a low-carb diet can cause weight loss [2:04:30];
- Red Pen Reviews [2:11:00];
- More.
Stephan’s neuroscience background and his focus on the nuances of obesity [2:15]
Stephan’s path to becoming one of the most thoughtful people on the nuances of obesity
- Stepahn was a biochem major as an undergrad, but had neuroscience in mind
- His idea was that biochem would provide a foundation for going into neuroscience later
- He did his PhD with Al LaSpada at the University of Washington studying neurodegenerative disease
- He stayed at the University of Washington for a postdoc with Mike Schwartz
- He has always been fascinated by the brain, but didn’t know which area of neuroscience he wanted to get into for a long time
- He became interested in neurodegenerative disease for a few different of reasons:
- 1 – They’re just absolutely horrible diseases
- 2 – His grandmother had Alzheimer’s disease
- In grad school he was studying a class of neurodegenerative diseases called triplet repeat diseases
- This includes Huntington’s disease
- They are also called polyglutamine repeat diseases
- The genetics of Huntington’s disease are complex and interesting
- It’s non-Mendelian because the length of the CAG repeat actually changes intergenerationally
- The weird thing about it is these CAG repeats are unstable in replication
- Theycode for polyglutamine structures in the protein
- You tend to see an enlargement of these polyglutamine repeats from one generation to the next
- So it has this really weird non-Mendelian pattern
- The penetrance is pretty high, meaning if you have this repeat of a certain length, you are going to develop disease
- But it’s not 100% fixed
- Stephan was studying a less common disease called SCA7, spinocerebellar ataxia type 7
- Not many people have this disease
- He had always been interested in fitness and nutrition
- So when he started learning about the neuroscience of obesity during his PhD work, he got really into it
- This was a way to satisfy his desire for impactful research
- He realized there was a ton of information on this topic that was incredibly enlightening and not making its way to the public
At what point, finishing up your PhD did you connect with Mike?
- He was interested in obesity and wanted to stay at the University of Washington for personal reasons
- Staying at the same institution after your PhD is atypical but he was not a big fan of the typical academic thing
- Mike’s lab was a really good fit
- He was a postdoc with him until 2013
- Peter remembers meeting Stephan at a conference in 2012, 10 years ago
How obesity has changed for humans throughout history [8:00]
- Humans have been around for maybe 6 million years
What has changed over the last 1000 years in terms of our phenotype?
- Thinking of body shape of people in modern, affluent societies (like the US) compared to a typical human 1000 years ago, we are much fatter
- 1000 years ago there was obesity among the wealthy, probably for similar reasons that we have obesity today
- There is evidence of this from Egyptian mummies
- Certainly the prevalence was much lower
- Just to be clear, we’re defining obesity in the most traditional way as a BMI (body mass index) of more than 30
- The advantage of BMI is it’s really easy to measure and you can calculate it from these really simple measures that go back a long time
- Unfortunately they didn’t have DEXA machines in 1890, which would’ve been a more informative way of looking at it
How BMI has changes in recent history
- 120-130 years ago only a few % of people (low single digits) had a BMI > 30
- More recently, we start to have really good data in the US in 1960 when the NHANES (national health and nutrition examination survey) began
- The % of people who are obese by this measure has gone up from the late 1800’s to maybe 12% of adults in the US
- The category of extremely obese refers to a BMI over 35
- There is class 1, class 2, and class 3 obesity; these correspond to a BMI of around 30, 35 and 40 (see the table below)
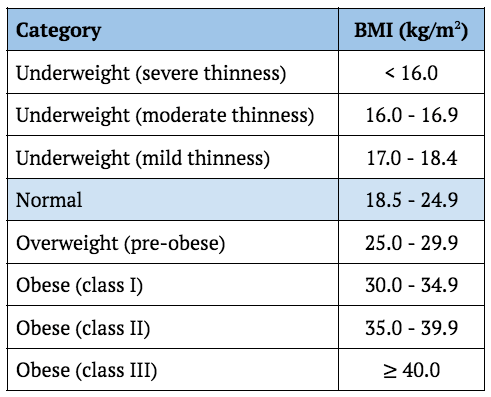
Figure 1. Basic BMI categories. Image credit: Wikipedia
- More recently, the median BMI has increased too
- The most extreme changes happened in the more severe obesity category
- Very few people had BMIs > 35 in the earliest measures
- Today 9-10% of adults have a BMI > 35
{end of show notes preview}
Stephan Guyenet, Ph.D.
Stephan Guyenet earned his BS in biochemistry at the University of Virginia and PhD in neuroscience at the University of Washington. He then went on to study the neuroscience of obesity and eating behavior as a postdoctoral fellow in Mike Schwartz’s lab. He’s spent a total of 12 years in the neuroscience research world studying neurodegenerative disease and the neuroscience of body fatness. His publications in scientific journals have been cited more than 3,600 times by his peers.
Today, he continues his mission to advance science and public health as a researcher, science consultant, and science communicator. His book, The Hungry Brain, was released in February of 2017 and was named one of the best books of the year by Publishers Weekly and called “essential” by The New York Times Book Review. He is a Senior Researcher at GiveWell and scientific reviewer for the Examine.com Research Digest. Past clients include the Open Philanthropy Project.
He is the founder and director of Red Pen Reviews, which publishes the most informative, consistent, and unbiased popular health and nutrition book reviews available. He is the primary designer of an innovative course-based body weight management program called the Ideal Weight Program, which is part of the HumanOS platform. He periodically contributes to the scientific literature and is a review editor at Frontiers in Nutrition. [Stephan J Guyenet, Ph.D]
Twitter: @sguyenet

So carnivore diets raise the risk of cardiac ASCVD, but as Peter often asks, where is the body count?
Sorry, that question should read either “what is the body count?” or “where are the body bags?”. Do you really believe that all these other biomarkers of health would improve and people would feel great and potentially resolve health issues, but high LDL should be a concern? Maybe you should be considering the idea that high LDL is a risk under certain conditions, but not others.
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2788975?widget=personalizedcontent&previousarticle=0
https://www.atherosclerosis-journal.com/article/S0021-9150(19)31501-1/fulltext
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7793228/
I believe the idea of different areas of the tongue tasting different things has long been debunked. All areas taste all flavors. Some areas are more sensitive but those areas are more sensitive to all flavors.
https://www.smithsonianmag.com/science-nature/neat-and-tidy-map-tastes-tongue-you-learned-school-all-wrong-180963407/
Depending on when this was recorded the FDA has TWO (not 1 as mentioned in the podcast) approved weight loss obesity drugs – Eli Lilly’s injectable Mounjaro (tirzepatide) induced greater weight loss than placebo and Novo Nordisk’s semaglutide in adults with type 2 diabetes. Both are glucagon-like-peptide-1 receptor agonists.
Given how much literature there is indicating the weakness of both elevated LDL and/or low LDL as predictors of CVD, I think it’s time to reconsider it as causal. In fact, there are those who propose that – under specific metabolic conditions – high LDL is actually normal and protective. Dr. Ali presents an argument that counters both Peter and Tom Dayspring. It’s a slight variation on Dave Feldman’s model (which Peter has apparently – and rather smugly – dismissed), that I’d like to hear Tom’s and Peter’s take on. It’s here: https://www.youtube.com/watch?v=qXtdp4BNyOg
Link between high cholesterol and heart disease ‘inconsistent’, new study finds
https://jamanetwork.com/journals/jamainternalmedicine/article-abstract/2790055
I have some detailed comments on different sections of the talk. I am an independent researcher on this topic for >20 years out of personal interest. Obesity is too multi-variable an issue in reality than some of the podcast discussions on isolated variables, e.g., genetics profile of 50% of the population somewhat pre-disposed to obesity (based on current incidence rates).
The discussion of “genetics” as primary driving variable hypothesis ignores other key environmental (food type availability, usage-> sugar, highly processed foods), economic (why does obesity run higher in lower income US segments currently is an interesting question), & cultural factors (direct family, upbringing, community peer groups, official gov’t/AMA guidance on nutrition, etc).
I am very familiar with caloric energy-based model of nutrition vs a metabolical model (insulin, energy storage/usage types, endocrines, gut biome), but found that part of the podcast somewhere between missing the key points & context, or even a little confusing, when it should be relatively straight forward.
In other words, the % pre-disposed genetically to obesity may not really be 40 or 50% (as current US obesity rates) but could be much higher or even quite different based on the other strong driving factors, e.g. food composition/balance/% highly processed food. The familial/food cultural/food usage environmental variables are very likely strong co-variables that also play into the “heritability” metric that may not be pure genetics—though epigenetics are also certainly also at play, population wise.
Overall, some pretty interesting discussions in this podcast nonetheless, and I will have to go listen to some of the older ones (e.g. U Colorado Richard Johnson, a personal favorite).
Personally, I have been doing lower carb diets for >20 years, but in last 12 months I persistently and slowly reduced 20%/50# of my previous weight, changed shape (minus 4 inches belt size) with minor tweaks to add regular intermittent fasting, and focus on more real food sources (mostly plants some nuts, whole grain) for fiber as essential menu item. A side effect was complete remission of psoriasis, which had only shown up within last 5 years, a likely connection via formerly “leaky gut” that is much improved…more later….
And, as Peter should know as well as anyone, the marker we should be looking at to assess cardiovascular risk is apoB, not LDL-C. So why allow the conversation with Stephen about carnivore diets to devolve into mocking of those with high LDL-C? https://jamanetwork.com/journals/jamacardiology/fullarticle/2786334
Can anyone answer why some people get an elevated heart rate taking semiglutides? Does this make it dangerous for some people to take even as it is considered generally safe?
I wanted to share David Barker conducted research on mothers’ nutrition during gestation and the long-term outcomes of their offspring – he used the Dutch Hunger Study as well as data collected in England tracking birth weights, mother’s health, and the long-term health of their adult children. It’s all observational but suggests that a mother’s diet can have an effect on their child’s likely hood of obesity.
Jason Fung preaches that fasting works through decreasing insulin levels. Lower insulin levels mean the body can burn its fat reservoirs.
But then how can Semaglutide work if it increases insulin levels?
Is Jason Fung wrong?