
In April I was part of a panel at the Milken Global Conference, the title of which was something like, “Keys to a healthier and more prosperous society.” The panel was moderated by Michael Milken, and it was great to meet him and his rock-star staff (especially Shawn Simmons, Paul Irving, and Nancy Ozeas). The other panel members were seasoned vets of the obesity discussion: Troy Brennan (Executive VP and Chief Medical Officer of CVS Caremark), Tom Frieden (Director of the CDC), Lynn Goldman (Dean of the School of Public Health at the Milken School of Public Health, at George Washington University), and Dean Ornish (president and founder of the Preventive Medicine Research Institute). I was the pauper in the group—no big credentials and zip-zero “panel” experience.
A few weeks before panel, we all jumped on a conference call and Michael set the stage for the discussion he wanted to moderate. He pulled no punches. “If you include the indirect cost—lost productivity, for example—the total cost of obesity and its related diseases is $1 trillion per year to our economy. This is unacceptable.”
Who could disagree? Hell, I usually only reference the direct cost of obesity and its related diseases—about $400 billion annually. But whether we talk about the direct or indirect cost of these diseases, I’ve always found the human cost even greater—every day 4,000 Americans die from four diseases exacerbated by obesity and type 2 diabetes: heart disease, stroke, cancer, and Alzheimer’s disease. Now that is really un-effing-acceptable.
So, back to the panel. The idea of being on a panel kind of freaked me out, even more than the sheer terror and vulnerability of TEDMed. No control. The possible need to be defensive. Sound bites over substance.
I don’t enjoy debates. Nothing comes of them. Just greater and greater polarization. The “winner” isn’t even necessarily the one with the best “facts.” Gary Taubes shared this quote with me recently, which I find really insightful. Dallas Willard, a well-known ecumenical pastor and theologian, was often invited to debate the existence of God and other matters. These invitations included Richard Dawkins himself. His response: “I don’t debate, but I am glad to enter into a joint inquiry. We will seek the truth together.” That’s the attitude I like.
In the end, I decided to just tell a few (in some cases provocative) stories. Why? Because it’s easy to present reams of data, yet so few people remember the point. (If you want to read an amazing paper on the importance of storytelling, check out this one by one of my former surgical mentors, Curt Tribble. You don’t need to care one iota about training cardiac surgeons to realize the gems in this piece.)
I realized going into this that I would be the contrarian in the group. I don’t claim to know all (or even many) of the answers, but I’m willing to bend over backwards in search of them. I realize folks (from readers of blogs to members of the audience at the Milken Global Conference) want facts, answers, prescriptions. I think we need to know more, first.
Below are the notes I made for myself in the days leading up to the panel. Basically, I wanted to tell a few stories, plus summarize it all (if given the chance). I didn’t actually “practice” this or even take notes up on stage (which I regretted when I realized everyone else was smart enough to bring notes), so if you decide to watch the actual video of the panel, you’ll note that I only vaguely followed what’s written below.
But in my mind, here’s how I thought about it. (I haven’t watched the video and I’ve pretty much forgotten anything I said, but I’m sure what’s written below is better than anything I said. I did send the video to two of the best speakers I know to get their feedback. Their feedback: could have been much better, but not the worst job ever. Lots of work to do for next time. Duly noted.)
How did I find myself interested in this problem?
My arrival at this place is really a coming together of two revelations. First, during my surgical residency at Johns Hopkins, not surprisingly, I was often dealing with the complications from diabetes and obesity in my patients. It slowly became obvious that all I was doing was slapping on the surgical equivalent of Band-Aids without ever addressing the underlying problem. I was treating symptoms and not the actual disease. When I would amputate the leg of a diabetic patient, which I had to do, regrettably, all too often, I knew that my patient was more than likely to be dead within five years anyway.
The second revelation was five years ago—September 8, 2009—to be exact. I remember it so clearly. My sport of choice was marathon swimming, and I followed what I believed to be the iconic healthy athlete’s diet. I had just completed an especially difficult swim into the current from Los Angeles to Catalina Island, becoming one of a dozen people to do that swim in both directions. After more than 14 hours in the water, I got on the boat to begin the long ride back to Long Beach Harbor, and my wife looked at me, in my speedo, 40 pounds heavier than I am today, and said, “Honey, you’re a wonderful swimmer. But you need to work on being a bit less not thin.”
And not only was I, well, fat, despite all this maniacal exercise, but it turns out I was also pre-diabetic.
Her comment launched me into a series of nutritional self-experiments. I was already working out three to four hours a day, so the problem couldn’t be sedentary behavior. It had to be what I ate. Over the next year I manipulated my diet until I found what worked for me, which paradoxically didn’t involve eating less, just eating very different from the food pyramid. Along the way I became obsessed with reading the nutrition literature. What I learned was that the evidence supporting our dietary guidelines was ambiguous, at best, and occasionally contradictory. There was a real dearth of evidence to support what seemed like the obvious questions.
I realized then, that if the guidelines didn’t work for me and if I can’t figure this out, with my background as a doctor and someone who studies healthcare, maybe they don’t work for a lot of people. Maybe there are systemic problems here. Maybe these problems were at the root of the ongoing epidemics of obesity and diabetes. Lots of maybes…and not a whole lot of clear, solid, unequivocal answers.
Since then, I’ve made a personal and professional commitment to finding the answers. And if the studies don’t exist to give us unambiguous evidence, then raising the funds and enlisting the researchers necessary to do those studies.
What does success in public health look like?
When trying to understand complex problems, I like to start with success stories, identify patterns and work backwards—reverse engineering success. Consider the following graph.
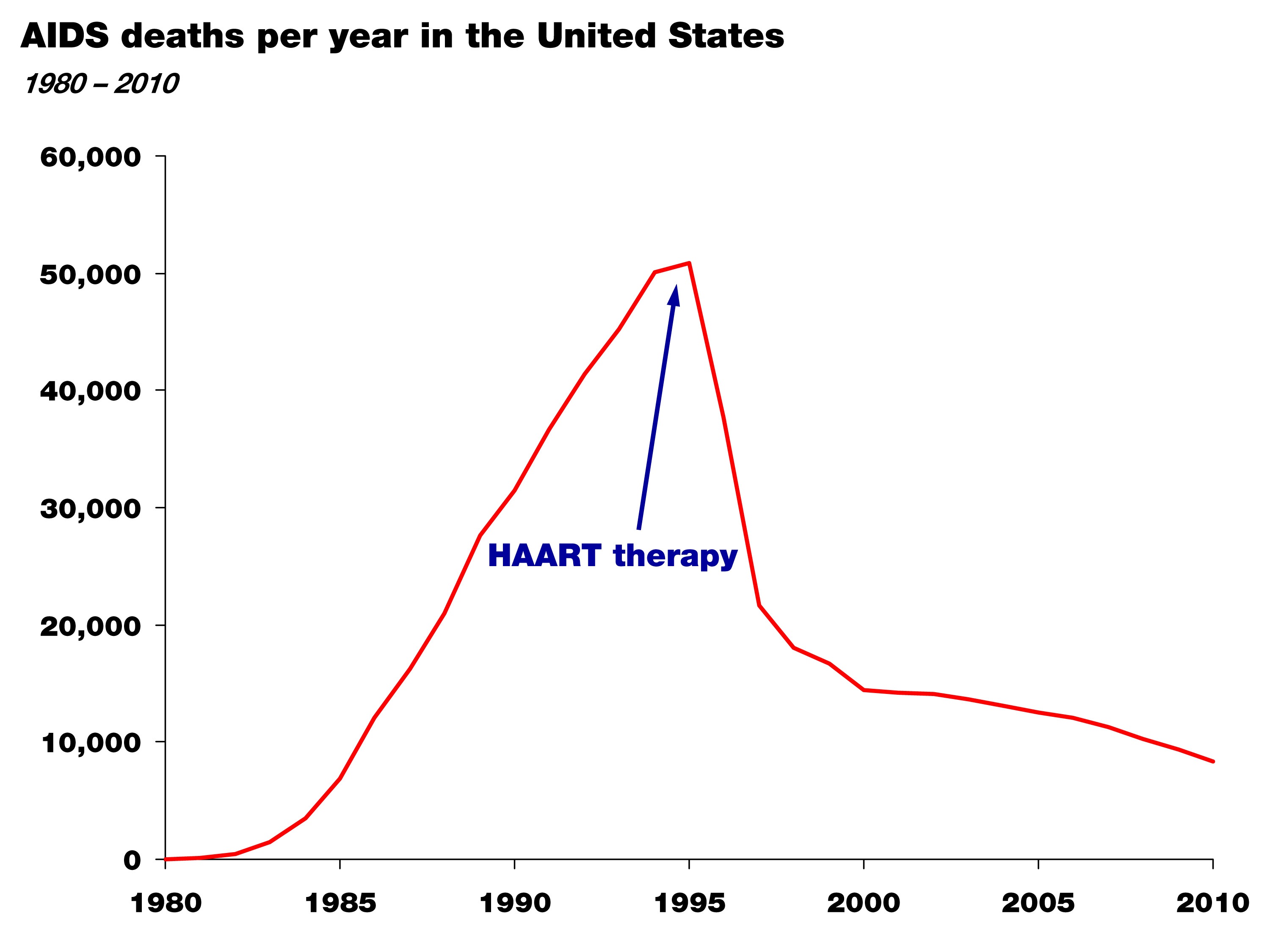
It shows the death rate from AIDS in the United States between 1981 and 2010. The point of this graph isn’t subtle. Death from AIDS rose steadily and monotonically through the mid-90s and since then has declined steadily. Though people still die from AIDS, this still represents a success story in health policy and science. For those experiencing the personal tragedy of AIDS, this is salvation.
So why did it happen? Well, first, the cause of the disease was correctly identified—the HIV virus—in the mid-80s; and second, by the mid-90s highly active anti-retroviral therapy, or HAART therapy, was able to effectively treat the virus and prevent progression to AIDS.
Again, two things happened: the cause of the disease was correctly identified, and an effective treatment was developed by an enlightened healthcare profession.
This is what success looks like. Now, let’s compare this story to that of obesity and diabetes.
Do we have this situation under control? The case study of “failure”
Let’s take a look at this figure. It shows the prevalence of diabetes in the United States over the last hundred-plus years. (Thanks to Gary Taubes who dug up these stats while researching his upcoming book.)
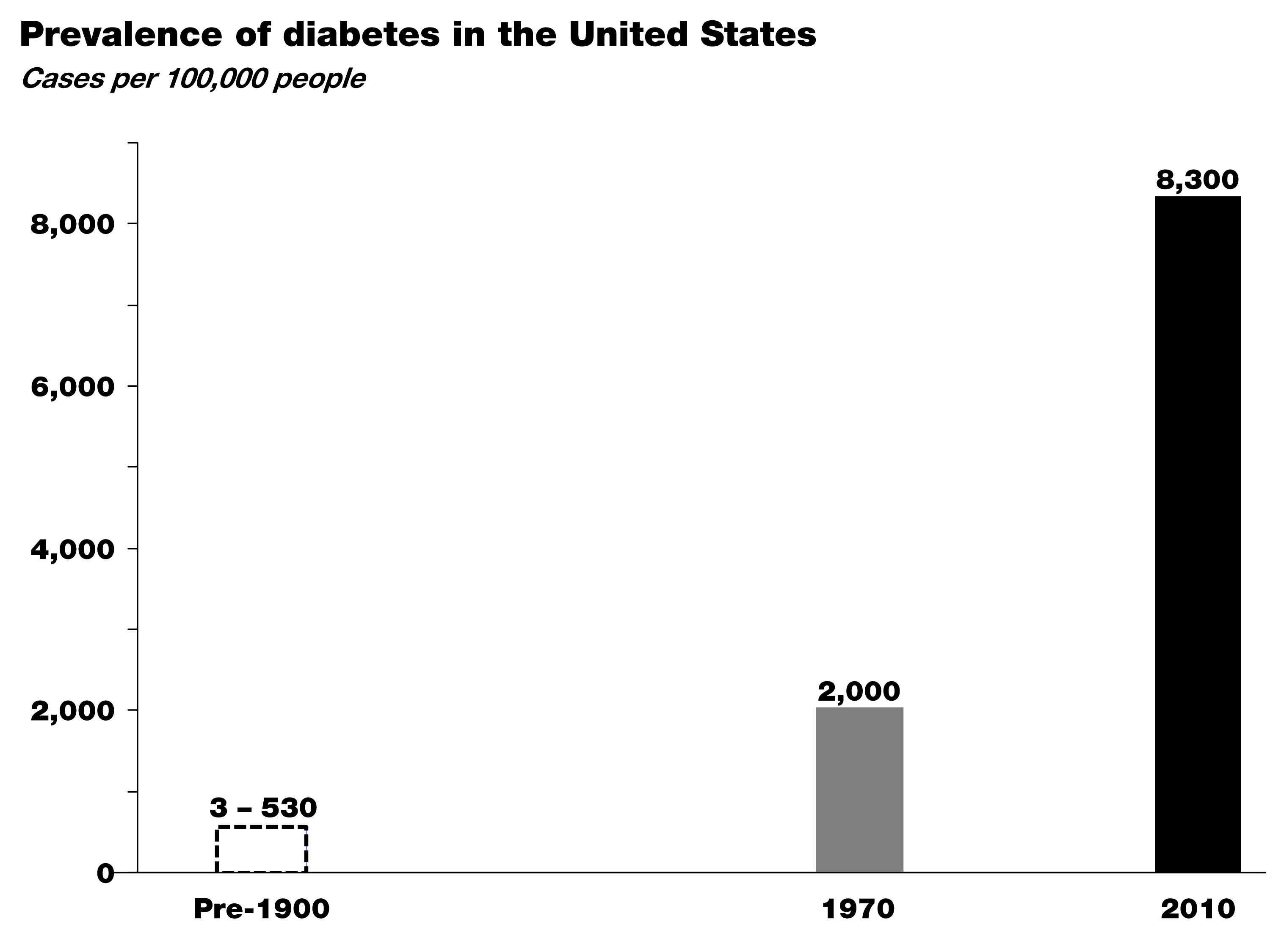
In the early 1900s the leading figures in medicine, Sir William Osler at Johns Hopkins and Elliot Joslin at Mass General, did exhaustive analyses of the number of patients with diabetes based on hospital records and census data. As you can see, diabetes was exceedingly rare in the 19th century—somewhere between about 3 and 500 cases per 100,000, depending on the analysis.
By 1970, around the time I was born, that number was up to 2,000 cases per 100,000, and between 1970 and today—at a growth rate of nearly 4% per year—that number has risen to more than 8,000 cases of diabetes per 100,000.
Worse yet, type 2 diabetes is now spreading into demographics previously naïve to the disease, particularly children. I don’t think any of us in this room today would argue that we have this situation under control. So where are we failing? Many of you understand the world of business. If this were a business, we’d be asking a lot of questions at this point, or we would be out of business. Like any business, we have two possibilities. We either look at our business plan (the basic premise for how we’re going to succeed) or the implementation of that plan (the way we operate on a day-to-day basis). When confronted with a runaway epidemic like this, we have to address the same two basic issues:
Either we understand the underlying cause of this disease and we have a good plan in place, but few individuals have the willpower or wherewithal to avoid the disease—whatever it is…In other words we’re not executing the plan.
Or, we don’t understand the disease in the first place and we’re giving the wrong advice. In other words, we don’t have the right business plan.
In this latter scenario, the failure is not one of personal responsibility, but of our assumptions about the cause of this disease. And these two scenarios have very different implications.
I am not certain which of these is more likely correct, but I do know the risk of ignoring the latter in favor of the former is not a choice we can make any more as a society.
So, maybe the question we should be asking is whether we are right about the environmental triggers of this disease—the underlying cause. Is it as simple as gluttony and sloth and a food industry that overwhelms us with highly-palatable, energy-dense foods, or is there something specific about the quality of the food we’re consuming that triggers these disorders? If we don’t answer this question about what is it in our environment that’s causing this disease correctly, just like we were able to answer it in the mid-80s with HIV’s role in AIDS, we can’t effectively treat the disease. Instead we’re stuck putting on Band-Aids.
Here’s another way to think about it: imagine this panel was on a new crisis in aviation. Planes are constantly crashing—falling out of the sky—and killing 4,000 people a day (just like obesity-related diseases are killing 4,000 Americans a day.) And you’re a pilot and you tell me that surely we understand the principles of flight. Right. Sure, we might suspect user error to be part of the problem. (Maybe the pilots aren’t flapping the wings hard enough!) But, maybe a better idea would be to go back to the drawing board to make sure we really understood this whole aerodynamics thing and we didn’t miss something important?
That’s how we think we have to look at this problem: 4,000 people in this country are effectively falling out of the sky every single day—dying—and we’re saying we’ve got it all figured out, and people just need to adhere better to our advice. I’m not confident that that’s the solution. Nor should you be.
Is there a policy-based solution to this problem?
Surely policy changes will play a necessary role in restoring our health. But it may be less about ‘how?’ and more about ‘when?’ I’d like to refer to this slide showing per capita cigarette consumption in the U.S. from 1900 until today—the number of cigarettes consumed is shown in grey with death rate from lung cancer superimposed in red.
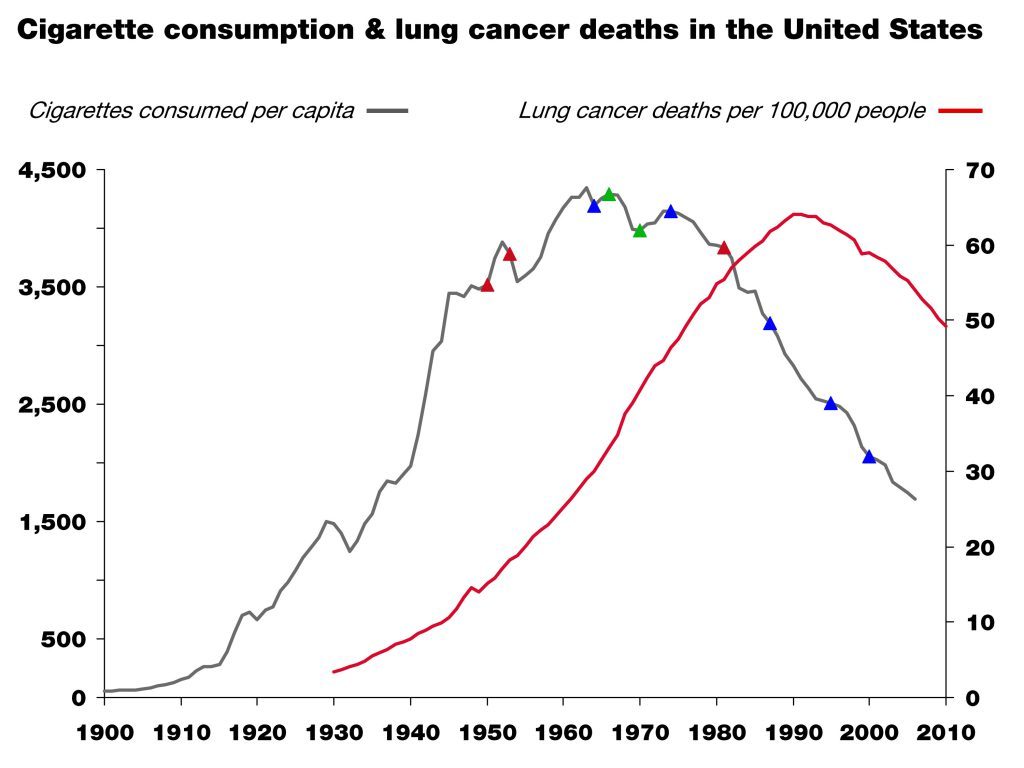
This is another success story. People in this room contributed to that success. The little colored triangles on the grey line are major milestones in science (red), market forces (green), and policy (blue). This is a great example of what one might call the “critical confluence”—scientific elucidation, policy action, market response, and behavioral shift—all coming together to save lives.
But, as in all things in life, algebra included, the order of events matters!
Which came first then? In the case of smoking and lung cancer, it was unambiguous scientific clarity, which in this case happened in the 1940s and 50s and resulted in the 1964 Surgeon General’s report. This information was absolutely necessary to drive the policy action, the market response, and the behavioral shift that followed. Without the knowledge that lung cancer is caused by smoking, no amount of policy or market response would have led to the necessary behavioral shift and so a meaningful reduction in lung cancer incidence.
When we consider the current situation with obesity and diabetes, we may still be missing the equivalent of the scientific clarity linking unambiguously the environmental trigger (smoking) that provided the obvious method of prevention (smoking cessation). And, again, if we think we do have that information, we have to ask why we’ve thus far failed to meaningfully prevent and successfully impact these disorders.
If the death rate from AIDS was still skyrocketing, I think we’d all agree we would either call into question our faith in HAART, or even the premise that HIV causes AIDS, if not both. Yet, in the face of skyrocketing obesity and diabetes, we play the who’s-on-first game all day long pointing fingers at people and industry.
Until we clearly identify the dietary triggers of obesity and diabetes, policies to shift behavior may be misguided and premature, despite their best intentions. Despite our best intentions.
I’m arguing that the policies so far may have been just that. Premature. And based on incomplete or faulty information. In other words, we may have the wrong business plan, but we blame our execution of the plan on our failure.
Parting shot
Today, we’re talking about a problem that touches, directly or indirectly, every single person in this room. It’s a topic that can be confusing and at times polarizing. We can’t lose sight of the big picture, which is easy to do when we just look at this problem through the lens of personal responsibility or will power. Remember, I used to think that “If people just learned to eat ‘right,’ (whatever that is), exercise and control themselves and their diet, everyone would be fine.” Today I reject that logic and the hubris that fostered it.
In the business world we know that the wrong strategy, no matter how well implemented, gives us little chance of success. Similarly, the right strategy, if poorly executed, often fails. What we need is the right strategy first and then the right execution second. At the moment, it’s hard to argue that we’re not failing with at least one of these two tasks. The question is which one.
Much of the discussion around this topic focuses on the execution; little attention is paid to the strategy or underlying insights that form the basis of the intervention.
Just 40 years ago the prevalence of obesity in this country was about one-third of what it is today, and that of diabetes about one-fifth. Is this all because Americans have become too gluttonous and slothful and the food industry figured out how to make food cheap and addictive enough? That they simply are too lazy and stubborn to do what we’ve been telling them to do—eat a little less, exercise a little more—for fifty years. Maybe. And I trust many good minds are already working on solutions to address that hypothesis.
However, what if the problem isn’t about non-compliance but about the nature of the advice we’re passing along. Maybe it’s our failure in that we have a simple idea about what causes these diseases, and like many simple ideas—paraphrasing Mencken here—it just happens to be wrong. It’s hard to fathom that two out of three Americans are simply too lazy to be active and too stubborn to eat healthy, despite losing their lives and their loved ones to the negative sequelae of these diseases. I find that hard to believe.
So, what if the problem is that our dietary advice is wrong in the first place? And incorrect dietary advice has resulted in an eating environment where the default for most people is a diet that causes obesity and diabetes?
If HIV or lung cancer were still spiraling out of control—as they were thirty and fifty years ago before the causes were unambiguously identified—the great minds in this country and the world would be leading investigative teams of scientists to figure out what we may have missed in our understanding of the cause of these diseases. We would not be complacent, perhaps because it would be harder to blame these diseases on the victims and their lack of will power. When we fail completely to prevent two devastating disorders for half a century, isn’t it time to investigate what we might have missed—what is it about these disease states that we do not understand? If nothing else, shouldn’t we hedge against the possibility—however slim you think the odds are—that we’re not as smart as we think we are. Those of us who are here today because of our business acumen know the importance of hedges in business. Isn’t it time we did that with obesity and diabetes?

Photo by PICSELI on Unsplash



Peter,
Love your work and have benefited greatly from it (lost over 40lbs being on a low carb diet and in being in ketosis). Also like your data driven approach. Speaking of being data driven, have you been able to measure your level of “insulin resistance/sensitivity” of muscles (while controlling for exercise and associated muscle glycogen depletion). In other words, are your muscles able to take up glucose more efficiently with smaller levels of insulin after your experiments with ketosis? Is there a test that can do this?
Also, given the importance of insulin levels for fat storage and obesity (from your previous posts), wouldn’t a point-of-care blood insulin meter be of great interest (along the lines of a glucose and BHB meter?). I ask because I have seen some publications on technology that can accomplish this (from universities).
It would be great, Ravi, and I’ve wasted, err… spent, many hours discussing it with POC experts. The problem, unfortunately, is that POC devices don’t work for complicated assays, of which measuring insulin is. It’s a RIA and requires an ELISA or similar test to detect, so hand-held and quick options don’t work (yet).
Peter,
You are indeed a gentleman & a scholar! A literal breath of fresh air amongst an atmosphere heavy of intellectual smog. Thank you for your strength and fortitude. Hopefully I can buy you a shot of MCT one day 😉 Pursuing Bliss for the win!
Thanks for the kind words, Anthony.
I read as much as I could trying to find your message about what to eat and what not to eat. Correct me if I’m wrong, are you basically endorsing the Atkin’s diet?
The answer is probably no, as I haven’t seen an endorsement of any particular diet on the site, but Atkin’s is based on similar science as what is described here. My personal reaction to this site and Atkins was that this site allows me to tweak problems in weight loss on my own because I understand some of the underlying biochemistry, while in Atkins if you run into any problems you were/are expected to see a clinician for them to try solving it. Dr. Atkin’s was a clinician, and if you read the section in his book on when people run into trouble with weight loss, you’ll see that he was not successful with a certain percentage of people. Possibly a combination of his not having time to read all the relevant research and that we now have much more research results available than he did.
Peter Attia: “If you’ve been reading this blog at all you’ve hopefully figured out that I’m not writing it to get rich. What I’m trying to do is help people understand how to think about what they eat and why. I have my own ideas, shared by some, of what is “good” and what is “bad,” and you’ve probably noticed that I don’t eat like most people.
However, that’s not the real point I want to make. I want to help you all become thinkers not followers. And that includes not being mindless followers of me or my ideas! Being a critical thinker doesn’t mean you reject everything out there for the sake of being contrarian”
https://eatingacademy.com/nutrition/is-red-meat-killing-us
Thanks for reminding folks, Vicente.
I noticed on Twitter someone was giving me grief for “having a blog called the eating academy, yet not wanting to spend much time talking about what I eat.”
Isn’t that like saying you want to take a course on are appreciation (or wine tasting) and you want the teacher to just tell you their favorite art (or wine), rather than teach you how to appreciate art (or develop your palate for wine)?
Obviously, what I do isn’t for most people.
Forgive me for being new here. I found my way here via Tim Ferriss. I enjoy his approach with disseminating information and wanted to get deeper into what he eats to lose or gain weight. Obviously I am not going to follow everything he does nor will I do it here either. There’s a lot of info to digest here and from what I gather, correct me if I am wrong, this is similar(not exact) to the Atkins way. Nothing wrong with this. I just want to know where this blog stands.
I don’t know your conversation on twitter, but I am not here for art/wine/food/health appreciation. I am looking to eat for optimal health. It’s akin to me taking a course by Tiger Woods on how to drive a golf ball. Yes, the info on the physics, mechanics, and drills are important. But I want to also see Tiger in action. I want to analyze his swing. I may never swing like him. But I can certainly learn a lot by seeing him put it all together. To a certain degree we learn and succeed by copying what other successful people are doing. And I hope to continue to learn from your wealth of knowledge.
Watching Tiger swing is likely to be much less helpful for improving your swing than having an expert golf pro actually teach you how.
Is there any work or reading material on something I find to be helpful to me.
I read alot about the digestive system having its own “brain” in that it decides what saliva to combine with what food and how to digest and the many decisions that we do not make in our brain consciously.
Then I read that the colon produces a lot of seratonin which produces a happy feeling.
Could it be that without meaning to, we have shown our ‘gut’ how to eat certain foods to make us happy and the ‘gut is very smart and will do that for us to make us happy but it does not possess the awareness of our brain in our head. So people are very happy getting fatter and fatter. Is this something that has been studied?
I think this is what has been going on with me because as I reduce stress and begin to eat well, I can experience a moment of stress that causes me to feel bad and my digestive system says to eat a fast food meal. Sorry for going on so long.
Dr. Attia,
I want to extend my gratitude for everything that you share on your website. Using your information about Ketosis, I was able to lose 22 lbs of fat, gain 7 lbs of muscle and go from climbing V2 to V6. (Rock climbers will understand. V-scale is the climbing scale for difficulty.) The rock climbing improvements were the only data that I was interested in. The body composition data was a side benefit. Well, less fat on my belly was an excellent side benefit.
Keep up the excellent work!
Jason
Thanks Jason. I’m pretty sure I’m a V0 if such a category exists.
Hi peter, I am very thankful to have found your blog. I am in my 4th week of no sugar, no starch and trying very hard to get into ketosis for weight loss. I have lost no weight despite being strict. I bought a glucometre that also reads ketones and my fasting results today was bsl 5.5mmols and ketones 0.3 .
I also only eat very small amounts due to previous gastric sleeve. My gp doesnt know much about ketogenics and dont know what I sm doing wrong. I have eaten nuts but chose macadamia nuts and about 10 per day…and I have been having half cup of full cream milk in my twa. That is all I can think of. Would appreciate any advice.
Hi Kelly,
For me, I had to restrict the amount of dairy I use ( heavy cream, 2tbl. In my one coffee a day). I love nuts and chesse (probably to obsession ) but found I needed to limit those to 2-4oz. A week. Remember, this is a lifestyle change, a process that will have to be adjusted several times. Also, the sugar cravings will be a constant source of contention for about a month (or more, depending on your body). Even now that occasional homemade cookie gives me cravings for days after I indulge. BUT, it will get easier. Read, experiment, and above all, Don’t give up. You need to find what works for you. I am just sharing what helped me lose the weight and become healthy. Hope this helps.
Hi,
In addition to reducing the nuts and dairy, I found that counting calories and being really mindful of my ratio of fat to protein helped me quite a bit as well. For example, if a given meal has 25 grams of protein, I make sure that I’m getting at least 50 grams of fat as well…hopefully that makes sense.
I know that many low carb high fat advocates say it isn’t necessary to count calories, but I’d like to point out that VERY few of them have ever been truly obese. I count calories because I’ve been so out of touch with my body for so long that I am just now, after over 2 months of LCHF, beginning to recognize when I am sincerely hungry, and not just eating out of habit.
Of course, we are all different and it’s important to experiment to find out what works for you.
Peter, the Energy Balance Consortium Study / Pilot study completion date was 6/30/2014 – any idea when the results will be released? This is really really exciting …
The pilot study will be completed this summer and data should be analyzed to design the 2nd phase by EOY.
Oh and I add about a tablespoon of coconut oil to my tea at least once, twice a day and cook in more generous amts of butter, olive oil. I have noticed since regularly checking my ketones that in the late evening I am 0.9 and in the morning I am 0.4 and by lunch I am 0.5….
When I quit sugar I gained 2kg and a couple of days after that I quit all starches too and my weight has not done anything…. I seem to have lost weight eating sugar and carbs and now I am healthy my body is rebelling!
Very enjoyable and logical discussion! It’s interesting that there is currently a bit of a backlash against universal low carb recommendations within the ancestral health and low carb communities, which I think your points speak to beautifully. With obesity, we don’t have all the answers and can’t provide a universal prescription without completely understanding the various forms of the “disease.” I think that the issue is even more complicated in women, and hormonal health (especially thyroid) can have a significant impact in determining the “best” diet prescription. I’m so thankful that people are still out there thinking, exploring, and researching that are willing to admit we don’t have all the answers but are doing their best to find them. Bravo!
Great job, Peter.
The government fella, toward the end, was basically saying, “Just give me money so we can DO SOMETHING! We’ve got to DO SOMETHING!”
That’s kinda how we ended up with these recommendations sending us down the path of diabesity, is it not? McGovern and his staff just wanted to “do something!”
anyway, great job planting the seed.. maybe we don’t know what we think we knew.. maybe our premise is wrong…
Is it just me or is that Milken guy creepy looking?
Anyway, since I’m originally from NYC the “Cynic’s Clinic” I speculated on the purpose of this event and the Milken Institute’s role/angle in it. It comes subtlety, like Ben Hur’s chariot” around min 39 when Mr. CDC explain’s the monumental profits to be had collectively and privately through public policy influence or otherwise. Who could benefit from a leg-up on that hey?
I think “not thin” Peter did a good job not splashing a not small glass of water on Mrs “I solved obesity” Berkeley, and for avoiding a debate with undebatables, but I’ll argue, at risk of alienating my caring co-bloggers that there is no shortage of “confusion crimes” on either side of the nutritional debate isle; Belief puncturing aphorism’s “fructose is good/bad”, “saturated fat is good/bad” “Carbs are good/bad” I suspect are the hobgoblins of……….
However, maybe all the Tempeh and tofu chicken I ate as a child, which falsely convinced me domestic livestock was much lighter and softer than it actually is, have instilled a desire for hard debate and generated fantasies of a Bruce Lee “Enter the Dragon” style shootout, where our nutritional icons and Iconoclasts (Fuhrman Mcdougall, Taubes, Attia, Ornish, Esselstyn, Bernard, Davis, Westman, Bernstein….) fling papers, journals, studies, chemistry, 19 syllable words and god forbid “epidemiological studies” at each other, one on one, until one gets the “deer in the headlights” look. (rear naked choke in the nutritional debate rule book). The last man standing owns the nutritional pyramid for a year.
I need to work on the paring though….Barnard-Bernstein, Mcdougall-Taubes….hmmm, Pete who will you take first?
Ha ha ha! As long I’m not playing the character of Kareem Abdul Jabbar…
The ultimate answer to the tobacco problem was simply people not smoking as much. They did this in a voluntary fashion, with some nudges. Part of the “nudge” was a legal one when the tobacco companies were found to be engaging in criminal behavior and this became widely known. Another part was the expense of smoking. Another part was the stigmatization of smoking.
The parallels with obesity are imprecise. We will likely never have the near unanimity of agreement about the main root cause of obesity as we did with smoking; further, obesity is already maximally stigmatized. And, there’s no clear target for taxation, increasing the cost of the behavior causing the disease. This is a much more difficult problem than the one involving tobacco.
The best chance for solution of the problem is mass education which requires solid data about what is really causing the problem. I believe sufficient data is already out there, but NuSi’s efforts will yield more. Solid data in the setting of a free market is the only thing which will solve the problem.
Peter, you were the most important member of the panel because you and Gary are doing the only thing that can be done at this point — providing education and gathering more data. Pretty much everyone else up there on the panel was either useless, more or less, or an outright fraud.
At a minimum, we’re “in the arena.”
Hello Dr Peter Attia,
I am intrigued with the paradigm and the data. My own weight struggles parallel the changes, but started in 1997 in Canada. Things got worst when I had my gallbladder out two years ago I was put on an extremely low fat carb diet, to lose 50 pounds and so called be better for my digestive system. Amongst other problems, I had no satiety. I controlled my calorie intake and for a time I (two years) was eating between 1200 and 1600 a day. And I was thinking about food all the time–it was horrible. During the two years, I gained 30 pounds. I thought I must be some kind of mutant at 5’10”. JM said I should be eating 2900 calories per day which I did not comply — she is nuts. I have dumped the low fat regime and I have reduced carb to 25-30 grams per day, added nuts and grass -fed or wild protein. BTW I am training for a half marathon, so moderate exercise. I am satiated. More to follow… . Niki
So many of you commenting on the blog are physically fit and avid exercisers. I am 61, overweight with high blood pressure. I just don’t know what to believe. I wasn’t tolerating blood pressure medication, so for the last 2 weeks I went on the DASH diet. My blood pressure lowered on all the vegetables and fruit, but my weight won’t budge. I’ve been logging on MYFITNESSPAL.com, faithfully sticking to 1200 calories. I’m hungry, and my weight won’t budge. I walk on my treadmill each day for 30 minutes. I started to read this blog when I started to search for answers. I am so confused. I would like to try your way of eating, but I’m scared to! I don’t want to lose my blood pressure lowering benefits, but I’m not satisfied with this low calorie way of eating. I eat a big apple and I’m hungrier than ever an hour later. I remember as a slender teenager I would eat rump roast with the crispy fat and it was so satisfying, and I stayed full, and I never gained weight. When I was 18 and got married and moved out of state, we lived with my inlaws for a while. I ate what they ate, bread with meals, and jello after dinner. I started to put weight on. All I know is the doctor told me I was insulin resistant, and so I got online to read about it. I feel like I have to figure out a rubic’s cube to go in the right direction. I wish I could trust something.
This may not be the best spot for this, but I was curious to know if you had any plans, through NuSI or your personal work, at looking into the possibility of using intermittent Rapamycin as a possible treatment option, or aid, in treating NIDDM? Or possibly any work treating NIDDM involving mTOR deactivation through CR, with or without NK? Seems as though this would be an area ripe for further study. Especially in further characterization of “benign” IR due to low mTOR activity versus “malignant” IR (blocking) due to overactive mTOR.
I’m personally interested in this idea, but it’s not on NuSI’s radar.
TII. following Dr Bernstein since 2010, generally ok.
But on April last year had a coronary;
they saved me with angioplasty and placed a stent.
Hi Dr A., what can i do about arteriosclerosis. I’m on LC already.
Afraid that stent may not hold, another coronary and so on…
many thnx in advance for your reply.
44 Y/ old/ father of 2.
United Kingdom
You should have advanced lipid testing to determine your true risk and be sure it’s being treated appropriately, even with pharma, as necessary. Many problems can’t be “fixed” or treated with diet alone.
thank you doctor. They let me go in 2 days, no advice not follow ups. [usually i feel ok, it feels like almost it did not happen] I got ramipril & bisoprol for B.Pressure [now BP is fine] and 75 mg of aspirin. [for life they said] Also was give me 2 types of statins [which to tell you the truth i do not take] but i i have increased Aspirin to 150 mg, on my own initiative. Te problem i have is that this incident has caused quite some trouble in the family, they watch me everywhere and…are more concerned than me [I feel nothing, physically am ok] and I still don’t know what to do about arteriosclerosis. Will ask my GP very soon for a full lipid test/ bloods etc and post main parameters in here…so you can take a look- if at all possible.
I would like to know if there’s a drug/ medication out there who would help, and please do not hesitate to recommend it. I got plenty on Dr-s on both sides [mine/my wife’s] in my country of origin [not uk] but they all are terrified of LC, and being a “nutter” is not easy at best of times 🙂 let alone after what just-happened. They all were kind enough not to go in “we told you so” mood, but I don’t like “the looks” and tck-tck-tcks. So- drugs i can find, advice that fits (LC) me…not! For many years i been following Dr. Bernstein, also read quite few others, yours included and seen your videos regularly; still i can’t get my head around “how to treat lipids/ arteriosclerosis” Pls help me a little, if you can.
Thnx!!!!!
Have you seen this yet regarding rFGF1? Hopefully this stands up to further experimentation.
https://www.nature.com/nature/journal/vaop/ncurrent/full/nature13540.html
I’ve become pretty obsessed with the FGF21 literature. This is just the tip of the iceberg. Probably worth a dedicated post at some time, as there is an interesting interaction with BHB.
Hi James,
Definitely take Peter’s advice to heart about the advanced lipid testing profiles that can be obtained. I would even go one step further and if possible find someone who is the equivalent of what we have here in the US which is a board certified lipidologist. They really do have advanced training in exactly what you need right now. Also think about more than just the underlying cause of the athero. I worked on the bench and then eventually used to help manage one the largest clinical reference molecular genetics and pharamcogenomics operations in the US (half a million+ DNA extractions alone per year) and I was surprised to learn that I actually carried a bad copy of a gene target known as Factor V Leiden which affects blood clotting in the reverse of Factor 8 Deficiency. Meaning I had a much larger chance of experiencing a complication from a blood clot than someone who didn’t have the gene. Someone that carries a bad copy from both parents has to be placed on anticoagulation pharma therapy immediately upon diagnosis. Little things like this can have a large impact on outcomes and if they aren’t known you can’t plan for them. Because of my discovery I began taking daily aspirin at a relatively early age and now I also supplement with Nattokinase. Do your best to learn all you can because ultimately you are the one most responsible for your health and to a certain degree we are all operating our own little health experiments even if we are allowing someone else to make all the decisions for us. Good luck to you and stay healthy!
many thanks Dan, I certainly will. After the tests will post a lipid profile so you guys and the doctor can take a look. Any advice would be appreciated. For 1 yr they give you ticagrelor, then is discontinued. I know patients who have test for clots, “how thin their blood is” as they take blood thinners for ages; but obviously I’m not as bad as them – maybe they think of it this way. Truthfully speaking, I have no idea what’s going on with me/ them/ everything. 🙂
I must enter into LC fully and ri-start to burn Ketones as I’m a T2 [like before/ but getting lil apprehensive/ i went more moderate] but is it good right now? Am also reading about Nattokinase, never having heard of it before; is it safe? is “Aspirin for life” safe also? ..and could 150 mg be too much? [i was recommended 75] Is there a “good statin” or any drug that can Fight Arteriosclerosis, so i get it asap and stat to take it… .
From GP to anyone, the only advice I had was: stop LC [my cholesterol is lil high from few years] ” you eat too much fat” Wish i can jump to N.York and see Dr Bernstein but the guy charges a lot. So basically am stuck…:) thanks again, @ you an anyone who is reading us.
Hi Elizabeth,
I am not an avid exerciser nor a fitness expert. I am a 56yr. Old overweight female who also reduced my blood pressure medication on my own (perhaps unwisely, admittedly) from 10mg. To 5mg.. I would suggest you browse the posts and read the ones (comments included) you think are relevant. Somewhere among the lowcarb blogs I have visited I read it was possible to eat mostly low glycemic veggies and stay low carb. But perhaps you need to analyze what it was you stopped eating that contributed to your lowered pressure. Fat is not the culprit to your weight issues. Start reading, this blog offers plenty of advice from readers and experts alike, including books, and other websites (I posted one below). That said, if you decide to stay lowcarb you won’t be disappointed, but be patient, become informed, ask questions.
https://livinlavidalowcarb.com/blog/does-insulin-deserve-a-bad-reputation-the-low-carb-experts-weigh-in/9458
On a personal note since it’s coming up this week, I’ve wondered, does comic con drive you crazy or do you just rarely ever make it to the Gas Lamp? I have some close friends that live near Kensington and we all went in 2012 and 2013 and had a blast. Huge revenue generator for the city but I’m sure many people would rather see it go to Vegas or Anaheim. I hope it stays in SD forever though. I love visiting and am definitely going to make a few more cons before I’m finished.
Not to add anything further to your plate… but part of why I like keto so much is the effect it’s had on my mind. I feel superbly clear headed and able to focus for long periods of time. I find the relationship between insulin/leptin/dopamine incredibly interesting. I wonder, even if it’s not so much on your radar, if anyone is doing research on ketones and the brain. I have seen some studies being done with coconut oil and Alzheimer’s for instance. This article in the Economist this month got me thinking about how there could be so many more practical applications of ketosis… at least worth researching. https://www.economist.com/news/21608314-consortium-researchers-has-shone-powerful-light-schizophrenia-some-needles-haystack
Is this even remotely on your radar?
Yes, very much on my radar.
That’s encouraging! Except we kind of need a clone of you to keep up with all these applications (and maybe another to write the blog… ha!) Thanks again for all you do. I tried to explain ketosis to a friend once, and he laughed and said, “Fat is good for you? HA! Why don’t we ask my wife who’s in the medical profession?” (Which was, of course, rhetorical, and by the way she’s a physical therapist… sigh.) I stopped talking about it to people that aren’t my family because they think I’m crazy to question people with far more credentials and apparent “intelligence.” Classic logical fallacy, yet my friend is a successful lawyer. I try not to let it bother me though, it keeps the prices low on grass-fed beef. Yep, red meat can kill you… better go buy some Cheerios.
I’d welcome the clone, but I’m pretty sure the NuSI staff (and my wife) would not!
Yes, I’m very much interested in this topic as well. I gained 25 kg in a short period (year or two) when I was given neuroleptic drugs for some “serious mental issues”. I lost that weight by restricting carbs, and also starting to exercise more. What’s more, I feel quite well, I don’t eat any psychiatric drugs anymore and so on. They’ve used low carb diet for treatment of epilepsy at least in children, and I guess it’s possible it can be helpful for some psychiatric diseases too. Of course it an in principle also be detrimental for some people, such as causing mania, etc. Some things maybe related to brain functioning and effects on mind of a low carb high fat diet: energy expedition and related issues (ketone bodies vs glucose, etc), GABA, inflammation.
Caitlin, Regarding your friend’s rhetorical comment, “Why don’t we ask my wife who’s in the medical profession?” I get frustrated with this one too. I know someone who has a drastic case of progressive MS her mom is a doctor, (who is overweight and always trimming the fat off of her steak! hehe It is difficult to even hint at suggestions. Peter has commented about how little that diet and nutrition is covered in a doctor’s training… only a couple/few weeks worth. Doctor Terry Wahls, author of “The Wahls Protocol” has also commented about how little she was taught of diet and nutrition and has had to make a complete about face in now teaching how the Paleo Diet has made such a dramatic change to her own progressive MS.
There is no quick comeback for these people (that isn’t just all-out insulting. hehe) but I would rehearse a few of these facts and learn some of the statistics. (verifiable) But then, as you yourself suggest, just be ready to walk away from a conversation. 🙁
In order to make suggestions to people whose health is headed downhill fast, despite orthodox treatment, though, I try to keep a mental list of medically trained people, of whom Peter is one (thankfully) who actually know something, and point them in that direction.
I also tell them that Peter’s Canadian and that gives him cred! *grin*
Oh… btw… here is a link to a study (government website) of how many hours of nutrition, as a subject, that are included in medical training:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2430660/?report=classic