
You’ll recall from last week’s post I did a self-experiment to see if I could learn something about the interplay of exercise and ketosis, at least in myself. To understand this discussion, you’ll want to have read Part I of this post.
However, before getting to this, I want to digress and briefly address two unrelated issues:
- Some of you (about 67 or 68 as of this writing) have sent me various links to news reports released yesterday reporting on a study out of Harvard’s School of Public Health. I was planning to eventually write a post about how observational epidemiology is effectively at the heart of the nutritional crises we face – virtually every nutrition-based recommendation (e.g., eat fiber, don’t eat fat, salt is bad for you, red meat is bad for you) we hear is based on this sort of work. Given this study, and the press it’s getting, I will be writing the post on observational epidemiology next week. However, I’m going to ask you all to undertake a little “homework assignment.” Before next week I would suggest you read this article by Gary Taubes from the New York Times Magazine in 2007 which deals with this exact problem.
- I confirmed this week that someone (i.e., me) can actually eat too much of my wife’s ice cream (recipe already posted here –pretty please with lard on top no more requests for it). On two consecutive nights I ate about 4 or 5 bowls of the stuff. Holy cow did I feel like hell for a few hours. The amazing part is that I did this on two consecutive nights. Talk about addictive potential. Don’t say I didn’t warn you…
OK, back to the purpose of this post: How is ketosis impacting my ability to exercise? Here is the summary of the results from my personal experiment:
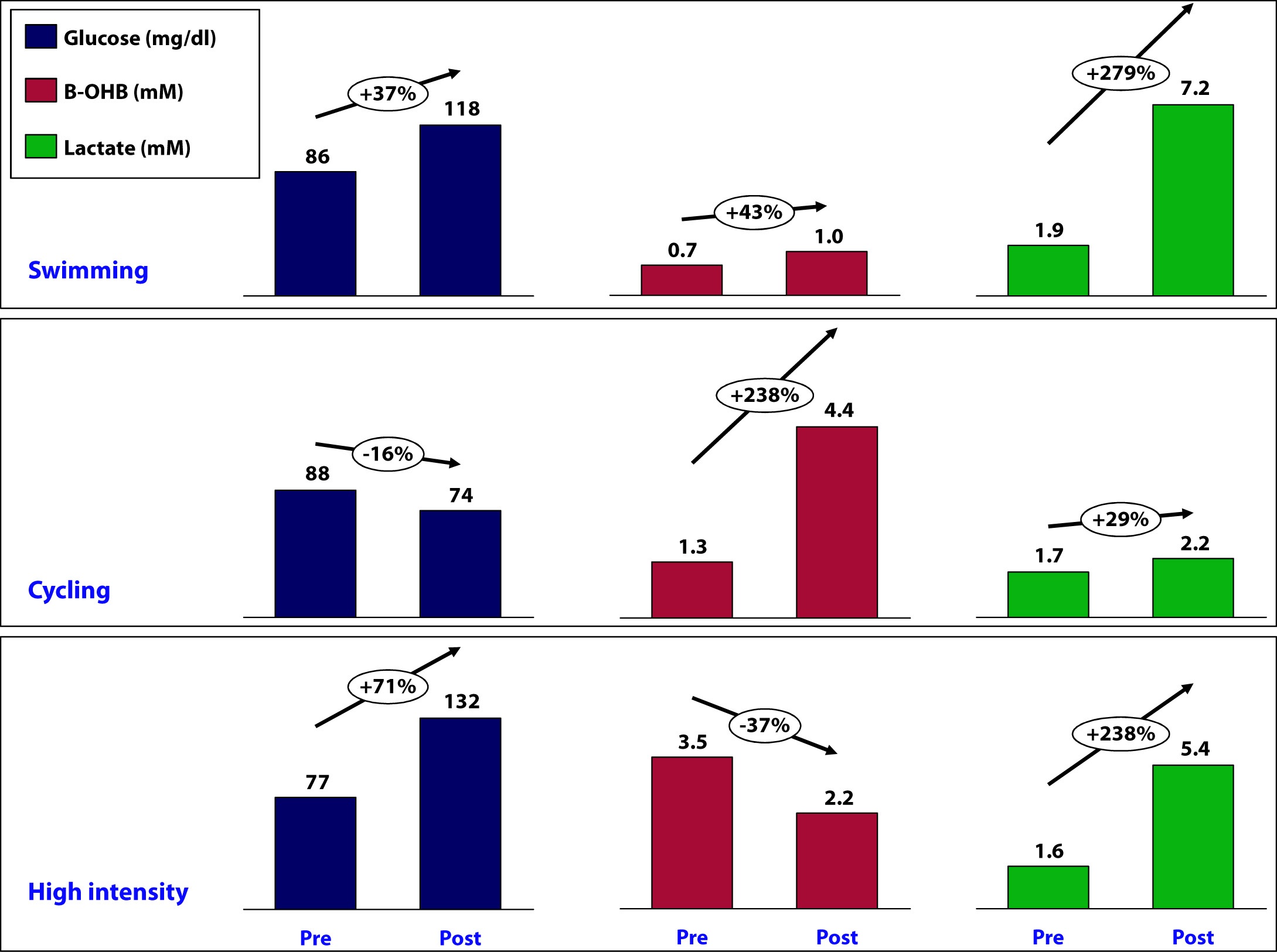
Let’s take a closer look at what may have been going on in each workout and see what we can learn.
Swimming
This workout probably produced the most lactate of the three workouts (we don’t know for sure because I only measured immediate pre- and post- levels without measuring in-workout levels). My glucose level rose by nearly 40% during this workout despite the fact that I did not consume anything.
How does this happen? Our bodies store glucose in the liver and in muscles in a “storage” form (a long chain of joined glucose molecules) called glycogen.
Whenever our bodies cannot access sufficient cellular oxygen, our metabolism shifts to a less efficient form of energy acquisition called anaerobic catabolism. During these periods of activity, we cannot oxidize fat or glycogen (i.e., use oxygen to harness the full chemical potential of fat or carbohydrate molecules). I will be writing in much more detail about these ideas in the next month or so, so don’t worry if these ideas seem a bit foreign right now. Just know that sometimes our bodies can convert fat or glucose to energy (efficiently), and sometimes we can only convert glucose to energy (inefficiently).
Because of my ketosis, and the metabolic flexibility that accompanies it, I only “require” that my body turn to glucose for energy under the most “stressful” forms of exercise – like I was doing a lot of during this workout. But keep in mind, my muscles CANNOT export one gram of the glucose they store, so any glucose in my bloodstream is either ingested (which I didn’t do) or coming from my liver, which CAN export glucose.
Furthermore, the stress of a workout like this results in my adrenal glands releasing a set of chemicals called catecholamines, which cause my liver to export even more of its stored glucose via a process called hepatic glucose output (HGO).
[As an aside, one of the major defects in type-2 diabetes is the inability of insulin to suppress HGO. In other words, even when not under the catecholamine stress that “should” lead to HGO, their livers constantly export glucose, which contributes to elevated blood glucose levels. The very popular drug, metformin, used often in type-2 diabetes, blocks this process.]
While I did experience a pretty large rise in lactate (almost 3x), my ketones still went up a bit. This could imply a few things:
- Elevated lactate levels do not directly inhibit beta-hydroxybutyrate (B-OHB)
- Mild elevations in glucose do not directly inhibit B-OHB
- Mild elevations in glucose do not directly inhibit B-OHB, if insulin is being suppressed (as is the case during vigorous exercise)
- B-OHB was suppressed, but we are only appreciating the net effect, which was a small increase (i.e., because of my MCT oil and activity, B-OHB levels were rising dramatically, but the rise was blunted by some other factor, such as HGO, insulin, and/or lactate)
More questions than answers from this workout, so on to the next workout.
Cycling
Despite this being a tough ride at several points, on average it was less stressful than the other two workouts and I spent the greater fraction of time in my aerobic to tempo (zone 2 to zone 3) zones.
A ride like this, however, is a great example of the advantages of improved metabolic flexibility that accompanies nutritional ketosis. My average heart rate during this 6 hour ride was 141. Prior to becoming ketotic, at a HR of 141 my respiratory quotient (RQ) was about 0.98, which meant I was almost 100% dependent on glycogen (glucose) for energy. Today, at a HR of 141 (with the same power output), my RQ is about 0.7 to 0.75, which means at the same HR and same power output as prior to ketosis, I now rely on glycogen for only about 10% of my energy needs, and the remaining 90% comes from access to my internal fat stores.
This is an important point. I will devote future posts to this topic in more detail, but I wanted to use this opportunity to mention it.
So what happened physiologically on this ride?
- My glucose levels fell, probably because I was slowly accessing glycogen stores for peak efforts (once my HR reaches 162 I become 50% dependent on glycogen) throughout the ride (e.g., peak climbing efforts, hard sections on flats), but my liver was not “called on” to dump out a massive amount of glucose in response to a catecholamine surge (and if it was, at some point during the ride, that amount of glucose had been used up by the time I was finished).
- B-OHB levels increased by about 2.5x – to 4.4. mM, which is pretty high for me. My highest recorded B-OHB level was 5.1 mM (also after a long ride). This confirms what my RQ data indicate — my body almost entirely relies on fat oxidation for energy for activity at this intensity. In the process, B-OHB is generated in large quantities, both for my brain and also my skeletal muscles (e.g., leg muscles). In reality, cardiac myocytes (heart muscle cells) also “like” B-OHB more than glucose and probably also access it when it is abundant.
- Lactate levels by the end of the ride were effectively unchanged though. Based on “feel,” I suspect I hit peak lactate levels of 8 to 10 mM on this ride during peak efforts, but I had ample time to clear it.
A few observations:
- I consumed 67 gm of carbohydrate on this ride (of which 50 gm was Generation UCAN’s super starch), yet this did not appear to negatively impact my ability to generate ketones. Technically, we can’t be sure this is the case, since I would have needed a “control” to know this (e.g., my metabolic and genetic twin doing and eating everything the same as I did, but without the consumption of super starch and/or without the bike ride). It’s possible that super starch did slightly inhibit ketosis and that my B-OHB level would have been, say, 5.0 mM instead of 4.4 mM. Metabolic studies of super starch show that it has a minimal impact on insulin secretion and blood glucose levels, hence the name “super” starch.
- Whatever impact peak levels of lactate production and hepatic glucose output had during the ride, they seem blunted by the end of the ride (and the ride did finish with a modestly difficult 1.4 mile climb at 6-7% grade, which I rode at a HR of about 150).
Since neither lactate levels nor glucose levels (nor insulin levels by extension) were elevated, I can’t really draw any conclusion about whether one factor, more than any other, suppressed production of B-OHB, so on to the next workout.
High intensity training
This sort of workout spans the creatine-phosphate (CP) system and the anaerobic energy system, and probably involves the aerobic energy system the least. I’ll write a lot about these later, but for now just know the CP system is good for very short bursts of energy (say 10-20 seconds) and recall the previous discussion of aerobic and anaerobic catabolism. In other words, this is the type of workout where my nutritional state of ketosis offers the least advantage.
- This workout saw the greatest increase in glucose level, about 70%. It is important to recall that during this workout I ingested water with a small amount of branched chain amino acids (BCAA’s – valine, leucine, isoleucine) and super starch, about 4 gm and 10 gm, respectively. I do not believe either accounted for the sharp rise in blood glucose and, again, I believe hepatic glucose output in response to a strong catecholamine surge attributed to this increase.
- Lactate levels also rose, though probably less so than during a peak swim effort. This suggests more of the effort in this workout was fueled by the CP system (versus the anaerobic system, which probably played a larger role in the swim workout).
- This was the only workout that saw a fall in B-OHB levels, which now offers some insight into what might be impacting B-OHB production.
Contrasting this workout with the swim workout draws a pleasant contrast: both saw a similar rise in lactate, but one saw twice the rise in blood glucose. In the former, B-OHB was unchanged (actually rose slightly), while in the latter, B-OHB fell by over a third.
This suggests – but certainly does not prove – that it is not lactate per se that inhibits ketone (B-OHB) production, but rather glucose and/or insulin. It is possible the BCAA played a role, and if I was thinking straight, I would not have consumed anything during this workout to remove variables. But I have a very hard time believing 3 or 4 gm of BCAA could suppress B-OHB. When you see hoof prints in the sand, you should probably think of horses before you think of zebras.
Conversely, there is some evidence that lactate promotes re-esterification of fatty acids into triglycerides within adipose cells. What does that mean in English? High levels of lactate take free fatty acids and help promote putting them back into storage form. This would prevent free fatty acids from making their way to the liver where they could be turned into ketones (e.g., B-OHB). In other words, we may be missing this effect because of my sampling error – I only sampled twice per workout, rather than multiple times throughout the workout.
So what did I learn, overall?
I think it’s safe to say I did not definitively answer any questions, which is not surprising given the number of confounding factors, lack of controls, and sample size of one. However, I think I did learn a few things.
Lesson 1
The metabolic advantages of nutritional ketosis seemed most apparent during my bike ride, evidenced by my ability to access internal fat stores across a much broader range of physiologic stress than a non-ketotic individual. (More on this in Lesson 4.)
Lesson 2
The swim and high intensity dry-land workouts suggested that my state of nutritional ketosis did not completely impair my ability to store or export hepatic glucose. This is a very important point! Why? Because, it runs counter to the “conventional wisdom” of low-carb (or ketotic) nutrition with respect to physical performance. We are “told” that without carbohydrates we can’t synthesize glycogen (i.e., we can’t store glucose). However, those who promote this idea fail to realize that glycerol (the backbone of triglycerides) is turned into glycogen, along with amino acids, not to mention the 20 to 40 gm of carbohydrates I consume each day (since my brain doesn’t need them). We know muscles still store glycogen in ketosis, as this has been well studied and documented via muscle biopsies by Phinney, Volek, and others. But, my little self-experiment actually adds a layer to this. Because muscle can’t export glucose (muscle lacks the enzyme glucose-1-phosphatase), we know that the increase in my blood glucose was accounted for by HGO – my liver exporting its glycogen. In other words, ketosis does not appear to completely impair hepatic glycogen formation or export. Again, we’d need controls to try to assess how much, if any, hepatic glycogen formation and/or export is inhibited. It’s hard to make the argument that being in ketosis is allowing me to swim and do high intensity training with greater aptitude, and as I’ve commented in the past, I feel I’m about 5-10% “off” where I was prior to ketosis for these specific activities, but at the same time, I could be doing more to optimize around them (e.g., spend less time on my bike which invariably detracts from them, supplement with creatine which may support shorter, more explosive movements), which I am not.
Lesson 3
Consuming “massive” amounts of super starch (50 gm on the ride), did not seem to adversely affect my ketotic state. My total carbohydrate intake for that day, including what I consumed for the other 18 hours of the day, was probably close to 90 gm (50 gm of super starch plus 40 gm of carbs from the other food I ate). This suggests one or two possibilities:
- Because of the molecular structure of super starch (I’ll be discussing this in the future, so please hold questions) and the concomitant metabolic profile that follows from this structure, it may not inhibit ketosis like other carbohydrate, and/or
- During periods of profound physical stress insulin secretion is being sufficiently inhibited that higher-than-normal amounts of carbohydrate can be tolerated without negatively impacting ketone production.
This is pretty straightforward to test, even in myself. I just haven’t done so yet.
Lesson 4
While it’s probably the case that my liver has less glycogen (i.e., stored glucose) at any point in time, relative to what would be present if I were eating a high-carb diet, it’s not clear this matters, at least for some types of workouts. Why? Take the following example:
- Someone my size can probably store about 100 gm of hepatic (liver) glycogen and about 300 gm of muscle glycogen at “full” capacity. This represents about 1600 calories worth of glucose – the most I can store at any one time.
- Before I was ketotic, my RQ at 60% max VO2 (about 2,500 mL of O2 per min consumption) was nearly 1.00, so at that level of power output (a pace I can hold for hours from a cardiovascular fitness standpoint) I required 95% of my energy to come from glycogen. So, how long do my glycogen stores last? 2,500 mL of O2 per minute translates to about 750 calories per hour, so I would be good for about 2 hours and 15 minutes on my glycogen stores.
- Contrast this with my ketotic state. Let’s assume my glycogen stores are now only half what they were before. Muscle biopsy data suggests this is probably an overly conservative estimate, but let us assume this to be the case. Now I only store 50 mg of hepatic glycogen and 150 gm of muscle glycogen, about 800 calories worth of glucose.
- In ketosis, my RQ at 60% max VO2 is 0.77 (at last check), telling me I am getting only 22% of my energy from glucose and the remaining 78% from fat. So, how long do my depleted glycogen stores last? Nearly 5 hours. Why? Because I barely access glucose at the SAME level of oxygen consumption and the same power output.
I know what you’re thinking…why is this an advantage? Just consume more glucose as you ride! It’s not that simple, but you’ll have to wait until my upcoming post, “What does exercise have to do with being in the ICU” to find out.
Going back to the black sheep example I open Part I of this post with, we know that at least one person in nutritional ketosis seems to make enough liver and muscle glycogen to support even the most demanding of his energetic needs.
Photo by Troy Oldham on Unsplash

Hi Peter,
Thanks so much for all this information!!
So is it beneficial to use metformin while on a ketosis eating plan or is that something that will inhibit the process? All the warnings talk about diabetic ketoacidosis and not to use metformin but I know that is different than nutritional ketosis.
Thanks again!!
It probably would make it easier, but that’s a speculation. It is by no means close to necessary.
Hi Peter
I am really enjoying reading through your website, I am a high performance endurance type athlete and trying out a Keto diet.. My dietician is not so impressed at this stage! Just wondering if you had done any research into the low carb diet and immune function? The main concern being that carbs have such a influence on immune function, and so by dropping the carbs, my immune response may not be good enough when flying etc.. Also was wondering what you thought about how having gels or high carb on race day only would affect the whole process?
Thanx!
I’m not a fan of gels/goos any time.
I have a question about pre-race diet. I will be running Boston in three weeks. I am on a quite strict LCHF diet and it seems to be working well – have been training hard and feeling good. The question is, do I maintain the LCHF diet all the way to the race, specifically two days and one day before (I eat almost nothing race morning – don’t like to have anything in my stomach)? Or do you recommend taking in a certain amount of carbs?
Thank you.
Stay where you’ve been training. No sudden switches on race day.
Peter,
Thanks for providing all this info to us. Two things (1) I was on a 3 hr ride today and since I only workout alone, I tend to think a lot. So, I didn’t have a particularly good day yesterday carb-wise, about 250g. This morn, I had my normal no/low carb/ high fat breakfast. Only consumed a little H2O on the ride and had what felt like boundless energy. After burning off 2500+ cals on the bike, am I jump starting ketosis this way? Is this the right way to think about it? I have a blood ketone meter but am just hesitant to use too often due to price. (2) love that Richard Feynman was included here. I was forced to read “What do you care what other people think” as a ninth grade summer reading assignment. Well, it really forced me to think about things differently and was one of the most enjoyable reads of my life. So, kudos for including him here.
Regards.
Hard to know what is going on. It would hard to be ketosis one day after consuming 250 gm CHO, I suspect. This would be a great time to do a check, despite the cost.
Hi Peter,
I have only started the last 8 days with less than 50g of carbs per day. I am on a week long training tri camp in Tuscany Italy. 6 hours on bike today, felt sluggish until stop after 4 hours then had some carbs felt like I was on rocket fuel the last two hours. Look forward to trying Ucan SS soon when I can get hold of it! Racing half Ironman on 19th May, hilly bike.
Question is it possible to be in nutritional ketosis and use Ucan SS so you can start an Ironman race with full glycogen levels in your muscles, and still have the metabolic flexibility you speak of?
Hello again Peter,
I wanted to ask you a couple of questions that I am struggling to get answered, so I thought you could help.
I have been on a ketogenic diet for a while, I was testing myself daily with a blood ketone monitor but it got a bit expensive so I stopped. I have been experimenting with getting in carbs here and there to try and preserve my top end so to speak. I am a triathlete but also road racing on the bike.
I just wondered, firstly are you still in nutritional ketosis? How is it going? Are you still using the superstarch? Have you had any more physiological testing to see how you are on that front?
I have been trying to boost my ketosis with MCT, mostly from coconut oil/creamed coconut. have you ever tried this? Do you know of any studies (or any personal experience) of using MCT based products to support ketone production in the presence of carbs?
Also, I have noticed something odd. I tried a similar approach to the cyclic ketogenic diet, with a carb refeed on weekends. I mostly did this due to reading some worrying articles on the affect of ketosis on testosterone production and the resultant effect on testosterone/cortisol ratio.
Anyway, I have noticed that the day after a re-feed my heart rate variability plummets and I feel awful. Have I made myself carb intolerant? Is this the result of pushing myself out of ketosis?
I have just ordered a large batch of ketone test strips so hope to have some answers soon.
Sorry for all the questions!
Yours
Tom Hughes
Hi Peter,
Having been cycling long distances (40-70miles) for 3 years and ultimately gaining weight over that time, I found Phinney, Volek, Taubes and you and for the past month or so have been strictly LCHF and ketogenic, have dropped 10lbs, feel great, do not get hunger pangs etc…(still have some weight to drop btw).
But I’m struggling with my cycling…if I ride at a high, but not exhaustive tempo, things are generally ok, I feel my legs are a little “heavy”, but manageable. However as soon as I need to push it (hard effort on flat/rolling terrain, or a long sustained climb – gradients of 6% and higher, up to as much as 17%), then I just seem to lack the energy to sustain that effort.
I dont take Mg supplements, but make sure I get enough sodium, but I wonder if an almost complete lack of CHO is failing me on these efforts and whether I need to think about taking carbs before and/or during my rides?
I really believe in the science of this LCHF lifestyle, but I have doubts due to a couple of rides where I just didnt feel “up to par”…yet your scientific approach seems to suggest I’ve got something wrong…..how do your legs “feel” when tackling sustained effort like climbs of 6-8 miles?
do I need to give it more time?
Thanks!
Impossible for me to troubleshoot without spending time with you, which I can’t do. If the issue is not one of sodium, potassium, magnesium, or hydration it seems like you (as was the case with me) need more time to adapt. This literally means your muscles need to re-train to be more reliable at oxidation (vs. their preferred state of glycolysis). It will take a while. For me, 3 months to feel pretty good. Two years to feel better than ever. Worthwhile investment for me, but a personal decision for everyone.
Hi Peter,
First of all I’d like to thank you for the informative blog you brought to life. the amount of information is enormous.
Second, I have a question, to which I could not find an answer for so far.
I’m genetically pretty lean with a pretty fast metabolism. 6 Months ago I started weight training (to put on some weight preferably in muscle) and went from 141 lbs (11% bf) to 162 lbs (16% bf)
Naturally, I developed a little pot belly which now I’m trying to get rid of. (That’s how I stumbled upon ketosis and therefore your blog)
My BMR at the moment is at 3400 kcal a day. If I would go with a ratio (a figure I have from another place) of 60% fats 35% proteins and 5 % carbs. I’m obviously way over 120-160gm of proteins. (about 300gm)
I’m unsure how to ask this correctly cause English is not my native tongue. But what I’m trying to ask is, if I can ever reach ketosis with a percent based approach, or are the 120-150mg of proteins a (more or less) a fixed value. Would in my case something along the lines of 80% fats 15% proteins and 5% carbs the better solution? 80% (302gm) fats just seems to be a ridiculous amount to me.
I realize that you can’t give a definitive answer to my question, as obviously no two people are the same. I’m just looking for a pointer to what makes more sense. Percent based approach or strictly control the amount of carbs/proteins and the fill the caloric deficit with fats.
Thanks again for your awesome blog.
Fabian
Can’t troubleshoot with any value over blog. But if by “BMR” you mean basal metabolic rate, 3400 would be really high. If you mean “TEE” (total energy expenditure), that would make more sense. I prefer the terms REE, TEF, and TEE (as described on the blog).
I’m Sorry. What I was trying to describe is in fact what is described as TEE in your blog. I have obviously not yet managed to read all of your blogs. So on a training day I “need” about 4300 Kcals and on a normal day 3400kcals. If I go below these numbers, I definitely lose weight rather quickly.
No worries. That makes more sense.
I’d like to sincerely thank you for sharing your ‘n=1’ study. This was exactly what I was searching for. 🙂
Sid
Peter,
I have been on a Ketogenic diet for almost 6 months now and it has changed my life. I am down 47 pounds with about 60 or so to go. I am working with a great doctor at SpecialtyHealth in Reno who is very supportive of my plan and keeping an eye on my blood work and lipid panels including the NMR LipoProfile (86th percentile in insulin resistance). I supplement daily with a multivitamin, 600mg potassium, 400mg magnesium, 2000iu vitamin D and 1000mg fish oil. I for the most part am very strict on my diet with no cheat days. I even avoid all artificial sweeteners because I wanted to completely lose the taste for sweet.
For most of my time on this diet I did not exercise. My weight, lethargy and even depression made it so I had no interest in it. During that time I found that I had no need to supplement sodium. I love salt on my food and it has seemed to be enough. Over the past month I have stopped salting food (after preparation) in an effort to reduce blood pressure. My doctor mentioned there is conflicting opinions on the effect of sodium on blood pressure and exercise along would probably get my blood pressure in place. I wanted to perform an N=1 on my self and see if reducing my salt intake would lower my blood pressure (without exercise) and it did. It appeared to have taken me from pre-hypertensive to normal. Even without the additional salt on my food I still felt great and did not feel the need to supplement sodium. Recently I have started exercising in the form of mountain biking. Three days ago I rode 11.5 miles on a relatively easy trail. I felt great with lots of energy and finished even stronger than I started. Since that time I have really slipped into feeling bad with no energy, yawning throughout the day (which I never do anymore and definite “brain fog”. I feel so good most of the time now that feeling this way is horrible. It took me until today to remember the sodium supplementation and to me it made perfect sense with the introduction of the exercise. I took 2mg in the form of bouillon and already feel much better.
My question is does this make sense that I have just reached a level of exercise to require supplementing sodium or should I have always been doing it? Is there a way to gauge how much to supplement other than the way you feel? Also I wondered if the vitamin supplementing I am doing above seems appropriate or if you had any other suggestions.
Thank you in advance for your time and and for also being the architect of the lifestyle change that is turning my life around after i’ve tried everything else and failed.
Kevin
Hard to know, Kevin, without doing some blood work, though sodium needs can largely be addressed by “feel” — if you feel light-headed, you likely aren’t getting enough. Similarly, cramping is usually a sign for more sodium and magnesium (the potassium often takes care of itself when these two are corrected).
Hard to know, Kevin, without doing some blood work, though sodium needs can largely be addressed by “feel” — if you feel light-headed, you likely aren’t getting enough.
Hi Peter,
In case you haven’t seen it, Ben Greenfield has a great podcast with Jack Kruse on performance on a very low carb diet. He covers a lot of different topics and I guess he could for days on each of them. Basically his view is that you can perform at the highest level on a ketogenic diet but you need 24-36 months to adapt (and then add the cold thermogenesis). Jack Kruse’s blog must be right up your alley too 🙂
I’m not saying he is right or wrong but it’s at least some very interesting views he has.
https://www.bengreenfieldfitness.com/2013/06/jackkruse/
In my experience, there seemed to be a real turning point in my anaerobic capacity about 18 months in, so I think there is something to the idea of long-term adaptation that goes well beyond the short term adaptation.
Really interesting. I’m hoping for more info on that in part 3 of this series. Do you still eat around 100g protein/day, 20g carb/day and the remainder in the fat or have you tweaked the levels a little?
Lots of tweaking. Heavily dependent on training and travel schedule.
I had a question about how alcohol fits into the scheme of blood lipids and CV disease especially the belief that alcohol has a protective effect and this seemed like an OK place for it since you reference Gary Taubes article that includes the “compliance effect” in this essay.
The first mention I ever heard of alcohol consumption having a heart protective benefit was an old 60 Minutes segment on “The French Paradox”. That Paradox turns out to be the fact the french have lower rates of CV issues even though consume a relatively high fat diet….which we all know causes heart disease, hence a “paradox”.
Obviously the alternative hypothesis would hold that this isn’t a paradox at all, it’s just evidence the premise is wrong. They go on though to decide that french moderate consumption of alcohol has a mysterious protective effect against their obviously heart stoppoing fat laden diet.
Since then this line has come to be widely believed.
Perhaps you can someday do a piece about how alcohol is metabolized and how it fits into other issues.
I had the notion recently that the “compliance effect” that Taubes writes about as a major confound may explain much of the supposed protective effect of alcohol.
It seems a good guess that “moderate alcohol consumption” may be a pretty good marker for “high compliance effect individual”. People who drink immoderately are probably not high compliance and people who don’t drink at all may be either recovering problem drinkers or people with an undiscovered propensity for it.
“Moderate drinkers” may correlate pretty strongly with the sort of high compliance person who has better medical outcomes either with the treatment or the placebo.
Otherwise the French diet fits with your essays about asian diets. It’s not historically very high in sugar which is the main factor whose consumption increased in parallel with metabolic syndrome and obesity.
I’m also wondering about how closely related alcohol and fructose might be in long term effects on the liver and all that complicated biochemistry the liver does.
Yes, I need to learn more about this topic. At least two separate issues confound it: 1) the CHO content of some alcoholic beverages; 2) the specific effect of EtOH on the liver, independent of point #1, and how that impacts VLDL production, etc.
Hello, Mark and Peter, a very detailed and enlightening discussion of this topic is part of Dr. Lustig’s presentation “Sugar the Bitter Truth”.
Thanks MaryAnn, I’ll check it out.
On topic for Ketadaptation and exercise I just went through the excellent explanations again of ATP pathways, super starch and endurance exercise. Great stuff.
If I follow it correctly it seems to have implications for the much larger group of people interested in metabolic syndrome, obesity and exercise. It seems to imply that for ordinary pretty unfit people with too much fat, that aerobic exercise will have different effects in people with ketoadapted metabolisms than with glycoadapted (or whatever ya call it). If I’m not misunderstanding, ketoadaptation ought to produce a faster rate of fat loss and perhaps more rapid improvements in aerobic exercise performance for the same levels of exercise than would occur with glycoadapted people, especially where both are on non-calorie restricted diets.
This may be another variation on experiments contradicting the “calories are calories” paradigm that might have unambiguous results.
Dr. Attia,
Was wondering if you can discuss Metformin and how you feel about the addition of this drug? I started using it a few months ago and I have to tell you it has greatly helped in how I feel after I eat. And I am super super sensitive to carbs. I can tell fairly quickly if I’ve eaten too many about 30 min after I’ve eaten – even if I haven’t had a grain…I can feel the insulin response. I can tell that my insulin has risen. The addition of just 500 mg of Metformin has really helped squelsh that feeling. I really really try to watch grains, carbs, sugar etc. Sometimes I will have an insulin response after eating veggies or a salad and I even cut out balsamic vinegar b/c I thought that was what was causing this response. I do better with olive oil and red wine vinegar. I’m PCOS and wanted to come off of YAZ as i’m approaching 40 and I just was afraid of what would happen if I did. So I added the metformin. I can’t tolerate more though. I tried to up it to 1000mg and my digestive system can not handle it. Just wondering what your thoughts are. Again – have about 20 pounds to lose. My BP and cholesterol are all great. BTW I did a search on your blog for Metformin before posting this comment and only found one mention of it. If you have discussed just point me in the direction. Much thanks – Jessica
Jessica, it’s certainly a reasonable drug for some patients, and I’d prefer it over other oral agents used in T2D. As you note, though, the side-effects can be troublesome for many. Perhaps the ER version? (ext release)
Anyone (Peter or other) found about how much MCT Oil one can consume for 8-12 hours without experiencing GI distress during moderate to hard exercise? Just checking to see if anyone else has done the trenchwork before I go do it. 😉
Ben, VERY person dependent/specific. I can do 30 mL with ease, with our without BP coffee. 45 mL I’ve gotten away with, but not always. It basically depends on how quickly I can turn it into ATP. If very quickly, I’m ok; if not quick enough, I get GI distress. Lesson: start slow.
Hi Peter,
Have you noticed (for ex. during your bike rides) any changes of your heart rate for the same speed/power since you are keto-adapted and during your transition period.
I am reducing slowly carb (though I am not in ketosis) and I have the feeling that my RQ is changing (for ex. no carb during my rides and no bonking) but my HR is slightly higher. Then in this case I am wondering if I don’t waste the benefit of a better RQ with a higher HR…
I think so, but there are so many confounding variables, I can’t be sure. Fitness, hydration, etc., all play a significant role.
I was talking with my sister who is a cardiology nurse at Mayo Clinic and she freaked when I told her about the consumption of fats, protein and carbs. Her first comment was, do you know what this is doing to your kidneys? Is she confused about what eating too many proteins will do compared to what being in ketosis will do to the kidneys?
Who is eating excess protein?
I have 2 questions regarding athletic performance & ketosis:
Will being in a state of ketosis help increase performance in underwater hoceky (Yup, it’s real: The first 2 min of this vid will give a good indication of intensity and gameplay, if you’re interested: https://www.youtube.com/watch?v=zWftTaLD9rw )?
Will it help with post-exercise recovery?
From what I’ve read it seems the answer is no or slightly though my understanding of this topic is not yet where it should be. I intend to experiment (guinea pig = me).
Game description:
A weighted puck is pushed along the bottom of the pool by people wearing fins, masks & snorkels. No scuba gear allowed. One of the keys to great play is an excellent breath hold. Even a slight increase in bottom time would yield fantastic results in a player’s contribution to the game. A quick recovery on the surface (taking 2-3 breaths instead of 5-10) would also make a player more effective. So I’m really keen to sort that out.
Would a state of ketosis help me get a few extra seconds? From the definitions & explanations I’ve read underwater hockey is anaerobic and we certainly spend a lot of time in Zone 4 & 5. So no, ketosis probably won’t help. But what confuses me is that the VO2 seems to come down. And your performance at high altitudes has improved. Would that help in this situation or is it irrelevant?
Typical game time (tournaments): 20 – 30 min
Game time (weekday practices): 60 – 90 min
My second question is would ketosis help with post exercise recovery? Weekday practices are Mon, Wed & Thurs nights. On Thursdays my in-game performance is down (subjective observation: I feel tired, can’t out-swim people as often and bottom time is shockingly bad) and on Friday mornings I struggle to get out of bed and am physically tired for the rest of the day.
When do I have an “empty liver” and what’s a good way to fill it up again without going out of ketosis? Where can I find more detailed information on starting this diet? I’ve read the “How can I lose weight?” but I need a bit more info because as soon as I try to implement step 4 & 5 I start feeling irritable, hungry, I bonk and start craving sugary foods.
Thank you so much for this blog. It’s incredibly informative.
Am I correct in saying that your O2 consumption went down during exercise? Does that mean that you would enter the anaerobic cycle later and exit it faster? If so, does that mean being in ketosis could give me a few extra seconds underwater?
I’ve been reading more posts on your blog. My questions about going into the diet have been answered.
Yes, appears O2 consumption decreases, which may also explain the altitude adaptation I spoke of in other posts.
Hi Peter
Great article, it’s fun to read others self expermentations.
I was wondering, what do you use to check your blood glucose, lactate and B – OHB levels? I’m a nutritionist student and I’m very interested in this subject.
Thank you for sharing your knowledge and experience, it is very useful for all the curious brains out there!
Precision Xtra.
Thank you! Feel free to let me know if you have any interesting ideas for nutritional experimentations, I and my fellow students will have a go!
Peter,
You know the breakdown of your carb / fat energy usage during exercise because you have been tested and know your RQ at various VO2 levels. For those like me who have not been tested, is there a simplistic equation that shows the general relationship between %VO2 max or %max heart rate and RQ so that I can know, approximately, the % of carbs and % fat that I am using at a particular effort?
These numbers need to be measured. See post/video on Quantified Self.