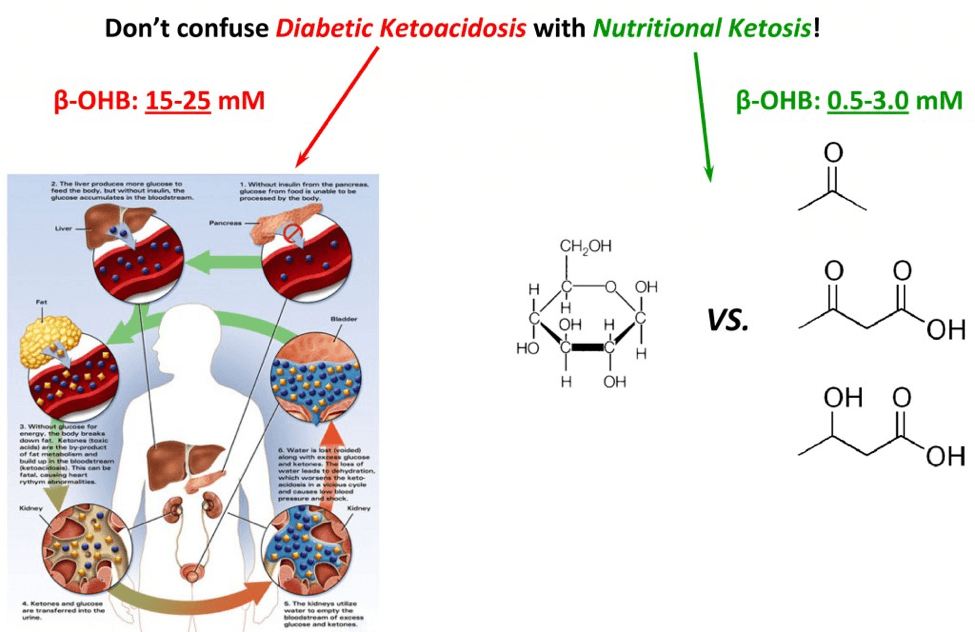
You may have heard from your doctor that ketosis is a life-threatening condition. If so, your doctor is confusing diabetic ketoacidosis (DKA) with nutritional ketosis, or keto-adaptation.
First, some semantics. Our body can produce, from fat and some amino acids, three ketone bodies (a “ketone” refers to the chemical structure where oxygen is double-bonded to carbon sandwiched between at least 2 other carbons). These ketone bodies we produce are: acetone, acetoacetone, and beta-hydroxybutyrate (B-OHB). [For anyone who is interested, they are the 3 most right structures on the figure, below.]
Why do we make ketones? For starters, it’s a vital evolutionary advantage. Our brain can only function with glucose and ketones. Since we can’t store more than about 24 hours’ worth of glucose, we would all die of hypoglycemia if ever forced to fast for more than a day. Fortunately, our liver can take fat and select amino acids (the building blocks of proteins) and turn them into ketones, first and foremost to feed our brains. Hence, our body’s ability to produce ketones is required for basic survival.
What is diabetic ketoacidosis? When diabetics (usually Type I diabetics, but sometimes this occurs in very late-stage, insulin-dependent, Type II diabetics) fail to receive enough insulin, they go into an effective state of starvation. While they may have all the glucose in the world in their bloodstream, without insulin, they can’t get any into their cells. Hence, they are effectively going into starvation. The body does what it would do in anyone – it starts to make ketones out of fat and proteins. Here’s the problem: the diabetic patient in this case can’t produce any insulin, so there is no feedback loop and they continue to produce more and more ketones without stopping. By the time ketone levels (specifically, beta-hydroxybutyrate) approach 15 to 25 mM, the resulting pH imbalance leads to profound metabolic derangement and the patient is critically ill.
But this state of metabolic derangement is not actually possible in a person who can produce insulin, even in small amounts. The reason is that a feedback loop prevents the ketone level from getting high enough to cause the change in pH that leads to the cascade of bad problems. A person who is said to be “keto-adapted,” or in a state of nutritional ketosis, generally has beta-hydroxybutyrate levels between about 0.5 and 3.0 mM. This is far less than the levels required to cause harm through acid-base abnormalities.
Keto-adaption is a state, achieved through significant reduction of carbohydrate intake (typically to less than 50 grams per day) and moderate protein, where the body changes from relying on glycogen as its main source of energy to relying on fat. Specifically, the brain shifts from being primarily dependent on glucose, to being primarily dependent on beta-hydroxybutyrate. This has nothing to do with what a diabetic patient is experiencing in DKA, but does illustrate how poorly informed and quick to react the medical community is. DKA and nutritional ketosis (or keto-adaptation) have as much in common as a house fire and a fireplace.