
For reasons I’m still struggling to understand, the idea of “nutritional ketosis” (NK, to be distinguished from starvation ketosis, SK or diabetic ketoacidosis, DKA) is often discussed and debated in much the same way as religion or politics. Perhaps this can be said of all nutrition, which is a shame. Nevertheless, in my continued defiance of such sensitive topics, I’d like to add another layer of complexity and nuance to this discussion.
The “rule of thumb” for NK is that caloric intake is determined as follows (this excludes a subset of ketogenic diets known as calorie-restricted KD which, as the name suggests, is specifically restricted in calories):
- Carbohydrate (total, not “net”): less than 50 gm/day, but ideally closer to 30 gm/day
- Protein: up to 1 to 1.5 gm/kg, but ideally below about 120 gm/day
- Fat: to satiety
Let me illustrate what this looks like for Joe (left), Jane (middle), and Jeff (right — an example of a calorie restricted KD), three hypothetical people in NK — but each with different caloric requirements.
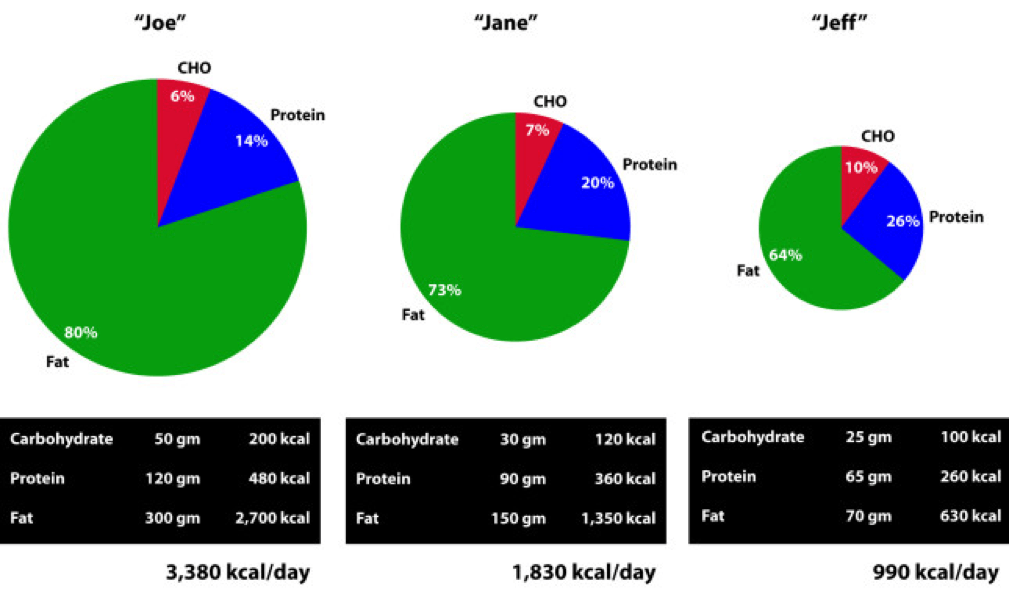
As a general rule, as caloric requirement increases the proportion of calories derived from carbohydrate and protein decreases (and the contribution of dietary fat increases), even while absolute intake of carbohydrate and protein increases.
Anyone who has bought a blood ketone meter knows how tough it can be to get “into” ketosis by carbohydrate restriction (since everyone asks, I use the Abbott Precision Xtra meter which uses two different strips: one for glucose and one for beta-hydroxybutyrate, or BHB). Most practitioners consider the minimum threshold of NK to be a fasting serum level of BHB above 0.5 mM. I’m a bit more stringent in my practice and like to see fasting BHB levels above 1 mM. To give you a sense of one person’s numbers (mine), over a 6-month stretch in 2013, when I was in NK, my mean (i.e., arithmetic average) morning fasting level was 1.7 mM with a median value of 1.4 mM. The highest morning level during that period was 5.2 mM. (The highest morning level I have ever measured in myself is 5.7 mM.)
But, it took me a long time to get it right, especially since at the outset of my foray into NK I was consuming between 4,000 and 4,400 kcal per day. (My average daily caloric intake for weight stability was about 3,800 kcal per day, which was validated by doubly-labeled water.) I could still easily “fall out” of NK. For example, on my daughter’s 5th birthday she insisted I have some of her tikka masala (contains lots of sugar), naan bread, and mango ice cream. How could I say no to a birthday girl who insisted on going to the nicest Indian restaurant in San Diego? As to be expected, the next day my BHB was 0.2 mM, and it took me 2 days to get back above 1 mM.
Here’s a little secret I’m about to let everyone in on… I like carbohydrates. I love sushi (though I now mostly eat sashimi). I love Indian and Thai food, though I prefer to make curry myself to keep sugar out. I make (and eat) the best hummus this side of the Nile River. I’ve figured out how and when I can eat them to meet the following conditions:
- Stay in NK (except on a few occasions like my daughter’s birthday);
- Increase my anaerobic performance;
- Preserve most (but not all*) of the benefits I enjoyed when I was much more strict about my ketogenic diet.
How, you ask? By learning to calculate my glycogen deficit.
(*) For me, the leanest body composition I achieved as an adult was in strict NK with no attempts to do what I’m about to describe below. Since I’m not a model and nobody cares if my body fat is 7% or 10%, I’m happy to be a little less lean if it gives me the flexibility to increase performance and live a slightly more sane life. At least for now.
PLEASE NOTE: I have never suggested, and can’t imagine I ever will suggest, that a KD is “best” or “right” for everyone. What I describe below may seem extreme, both in the amount of work required and the actual application. I fully acknowledge that (1) this is a highly analytical approach to eating, and (2) that I’m a “freak” (my wife’s words, not mine). I certainly don’t do this often, unless a lot is on the line (e.g., a big ride), but I like having this technique in my armamentarium.
If you’ve watched my presentation from 2013 at the IHMC, then you’re familiar with RQ. Through years of metabolic testing I have a pretty good sense of my RQ at any moment in time – when I’m sleeping, when I’m sitting around (most of the time), when I’m riding my bike at 200 watts, when I’m riding my bike at 400 watts, when I’m lifting weights, etc. This allows me to calculate what proportion of my energy I derive from glycogen and what proportion I derive from fatty acid. Consider the following example:
If I ride my bike at an average of 185 watts (you’ll need a power meter to infer this) for, say, 2 hours, I know my average RQ is between 0.76 and 0.80.
The approximate formula is %CHO = 3.333*RQ – 2.333, which can easily be derived from the observation that %CHO utilized increases linearly from 0% at RQ 0.7 to 100% at RQ 1.0.
Furthermore, I know my VO2 at 185 watts is 2.9 liters per min, which means (using the Weir formula which I presented previously) my energy requirement was about 14 kcal per minute, or 1,680 kcal over 2 hours. Hence, of these 1,680 kcal needed to pedal 185 watts for 120 minutes, 336 to 554 kcal came from glycogen. In other words, I utilized between 84 and 138 gm of glycogen.
(By comparison, several years prior to being in NK, this effort in me would have taken place at a slightly higher VO2 – closer to 3.2 liters per min – and at a much higher RQ – between 0.90 and 0.95 – meaning the exact same work output would have required somewhere between 300 and 400 gm of glycogen! That’s a real state of metabolic inflexibility. Basically, I was entirely dependent on carbohydrates for energy.)
Since the first metabolic priority for ingested carbohydrate is glycogen replenishment, I can, in this setting, consume probably somewhere between 60 and 120 gm of carbohydrate following this ride and stay in ketosis. Why? Because those carbohydrates are prioritized to replenish my glycogen stores AND I am highly insulin sensitive. Note the *AND* in this last sentence. (The especially astute reader will realize some of this glycogen debt will be replenished by protein and glycerol, the latter of which is liberated by lipolysis – see post on fat flux for a primer).
Clearly I didn’t consume this amount of carbohydrate on my daughter’s birthday, so why was I out of ketosis the next day? Because my glycogen debt was not high. Of course, I knew this and didn’t really care. But, if I know my wife wants to go out for sushi one night, and I know she’s going to make me eat a California roll, I can “rig it” such that I show up to dinner with a glycogen debt appropriate enough to enjoy them without significantly interfering with my liver’s BHB production.
Extreme example
At one point, I did two tough bike rides on consecutive days. Each day we rode 110 miles under challenging conditions. Over 6,000 feet of climbing each day and very strong winds, which were either headwinds or cross-winds. On top of this, we rode pretty fast. For the purpose of illustration I recorded everything I did and ate on the second day, which I rode a bit easier than the first day.
The second ride took 6 hours and 5 minutes. My average normalized power output was 225 watts, and arithmetic average power output was 184 watts. Based on mechanical work output, this required about 5,000 kcal. Factoring in the other 18 hours of that day, my total energy expenditure was about 6,800 kcal for the day, obviously not an average day. (A detailed explanation of where the extra 1,800 kcal were expended is beyond what I want to get into now, but it’s basically the energy required to keep me alive – transport ions, contract voluntary and involuntary muscles, etc. — plus move me around, and digest food).
So what did I eat that day?
- Breakfast (pre-ride): 5 scrambled eggs, 2 sausage links, 3 pieces of bacon, coffee with cream.
- In ride nutrition (I spread this out over 6 hours): 14 oz (not a typo) of salted cashews, 2 Quest bars, 1 peach, 1 apple, 6 bottles of Biosteel High Performance Sports Drink, water. (Since I know someone will ask, I did not consume super starch this day since I was craving cashews as my carbohydrate source and was craving more sodium, given the 90+ degree temperature.)
- Late lunch/early dinner (post-ride): 2 oz ham, 3 oz pulled pork, large salad with oil and vinegar dressing, 2 slices of cheddar cheese, 6 mini hamburger patties, 2 tomatoes.
What did this amount to?
- Fat – 351 gm, or 3,160 kcal of fat
- Protein – 245 gm, or 980 kcal of protein
- Carbohydrate – 321 gm, or 1,284 kcal of carbohydrate
(I used package information and Nutritionist Pro software to calculate this.)
Hence, on this day I consumed about 5,400 kcal in total at the following ratio:
- Fat – 58%
- Protein – 18%
- Carbohydrate – 24%
By all conventional wisdom I should not have been in ketosis the next morning, right?
The following morning, my BHB level was 2.2 mM and blood glucose was 5.1 mM.
Teaching point I can’t resist: Following 2 days of significant caloric deficit, about 3,000 kcal in total, I should have in theory lost about a pound (mostly fat, possibly some muscle) which would have been noticed on a scale. Instead, I gained 8 pounds over those 2 days! Sure it was mostly water retention, both from the glycogen (small) and the fluid accumulating in the interstitial space (“thirds space” fluid losses, large) due to a systemic inflammatory response. This happens under extreme conditions of exercise. In fact, the harder I exercise, the more weight I gain, transiently. I am at my absolute lightest following 2 days of travel (i.e., rest). So before freaking out at the sight of the scale, keep in mind that most day-to-day weight movement in our bodies is indeed water movement into and out of the plasma and interstitial space, respectively.
What’s my point?
Context matters! If I ate even one-quarter of that amount of carbohydrate and two-thirds of that protein on a normal day – say, 2.5 hours of riding or 1.5 hour of riding followed by 1 hour of swimming, or a day of travel with no exercise – I would have been out of ketosis for two days or more. (Of course, my appetite on those days would not have allowed me to eat 5,400 kcal without feeling sick, but I won’t get into that until a later post.) But on this day, with these glycogen demands, I was able to maintain the perks of ketosis AND glycolysis simultaneously.
There are days, though, when I overshot my glycogen need and end up with a low BHB and high fasting glucose the following morning. Conversely, there are days I underestimate my glycogen depletion and wake up with very high BHB levels and very low glucose levels (i.e., BHB levels higher than glucose levels, when both measured in mM).
Final thoughts
I felt a bit like I was in unchartered territory because the literature on nutritional ketosis hadn’t really (to my reading) explored this level of extreme activity. In future posts, I may write about other experiences and self-experiments, including my experience with exogenous (i.e., synthetic) ketones (which I did not use on this ride, but have experimented with on other rides – no, this is not “raspberry ketones” or other such gimmicks).
2017: You can read about one of my earliest experiences with exogenous ketones in this post.
Are carbohydrates necessary to produce 225 watts or more for hours on end? Yes. But, the key is knowing how much you need and when to take them. A lower RQ at a given level of intensity means less demand on glycogen. In my experience, working with athletes and non-athletes, most tend to make two errors (for lack of a better word):
- They over-estimate their carbohydrate requirement, and/or
- They forget that no factor influences RQ – and therefore substrate requirement – more than dietary composition during lead up to event (or “life”, which is sort of the ultimate event).
Know your engine, first. Then fuel it appropriately.
Photo by CloudVisual on Unsplash

OK, Peter, please provide the sources, peer reviewed studies and reference material which substantiates your position. I would enjoy reading it and would love to be proven wrong, if they exist. I know what legitimate research looks like and I don’t engage in “fat logic”. Can you provide these citations, source and reference materials please. I have my BS in Chem. E., an MS in Physics and my MBA in Finance and competed in NCAA Division I athletics winning a title in Track & Field. I fully well understand what constitutes a legitimate study and whether it exists. You can email me or post them here. I’ll look forward to it. I deal in facts and data and am very practical and pragmatic. Obesity increasing 300% in 30 years is not caused by genetics or evolution (which would take thousands and or hundreds of thousands of years). Thank you,
It seems you think I’m suggesting “genetics or evolution” are driving obesity. Not sure where you get that. Needless to say, this (hopefully) explains your confusion. If you do want to consider the link between OB, IR, and metabolic disease, you may find this interesting:
https://www.sciencemag.org/content/341/6148/856.summary
Also, consider the clinical resolution of IR s/p R-Y GB which occurs before meaningful weight loss. The is well documented in humans and animal models.
Kory, I too am a T1 for a relatively short time (2 years). By starting with a low carb diet, then transitioning to a very low carb diet (<30 gms carbs) and now being in NK for about 6 mons I find I have great BG control, rarely use any insulin over my basal dose (heavy resistence training days being the exception) and have no fears of hypos as I can be comfortably in the mid 50's with both brain and body happily living on BHB. Have yet to do a bike ride over 3 hrs without any carb intake but that is in the works for the months ahead. Cheers, Bob
Dr. Attia,
I appreciate very much your clarity of thought and attention to detail, also your engaging style of writing. Thank you for this blog!
In #3. of your earlier post “How Can I Lose Weight?” you write: As far as I can tell, there is no reason to limit non-starch vegetables. I probably eat an average of two salads per day.
Do you count the CHO in non-starch vegs as part of your daily allotment? ( If you’ve answered this already, I apologize for my oversight.) I eat considerably more veg than Dr. Bernstein allows in his 6-12-12 program, but will adjust to “eat to my (new Xtra keto-) meter,” if necessary to achieve DK. I am not diabetic, just find that I thrive on healthful VLC.
Thanks for your time. Best, KM
Thank you for your time, Best, KM
Thanks
I do, but it’s quite minimal. I just don’t feel like computing every sub-component of CHO in my diet, so I lump them altogether, though the obviously have very different impacts.
Hi Peter,
Great article again! Have you read Lyle McDonalds work on Ketogenic Diets? I’m on his “Targeted Ketogenic Diet” (3x / week weight training), having pre-workout carbs (2.5g CHO x each working set) 40 mins before.
Any thoughts on that approach?
Best regards,
JD
No experience with this, so unable to comment.
Peter,
You said you use Abbott Precision Xtra and their Ketone strips. Do you really spend $5 on each test? I looked online and the 10 pack costs $50.
Any way to testing cheaper (not meaning Ketostiks)?
Thanks,
JD
No, I buy either in Canada ($2/strip) or look for other deals.
Hi Peter, love your blog I think you’re the nearest thing to an “expert” as regards exercise and nutrition esp as it relates to LC.
In this vein I have a question (sorry!). I have been LC for quite a while and VLC / 24/1 IF’ing for over a year. I’m quite active in a biking/running/walking kind of way.
I have to be careful when VLC to avoid hypo-glycaemic episodes and need to eat about 120g of protein a day to avoid these and also be careful about eg alcohol as this can be very problematic from this perspective.
Anyway I have a few last stubborn vanity lbs to lose re: body-fat and decided to up my biking volume to achieve this. I have increased my ride length from 18 mile (avg) to much greater (60-100). Generally I have taken it easier on these longer rides averaging 17-18mph vs 18-20 on the shorter runs (this is a single speed (fixed) bike, not aero ).
I’m careful re: Fluid and mineral intake but I don’t eat any food during these rides, a 100mile ride takes between 5:40-6hrs.
After about 4 hrs I begin to “lose the plot” mentally speaking, when I stop (for a comfort break) I tend to have a very noticeable buzzing in my ears and as I go on I tend to feel punch-drunk and lose concentration. However my actual ride performance/power seem OK.
After such a ride I feel the most profound mental tiredness and I just want to close my eyes and fall asleep.
Usually after a few hours I tend to perk up (with or without food, but especially with).
My assumption is that I’m going hypoglycaemic, probably because the intensity/duration is enough to reduce blood glucose beyond my ability to compensate.
I find that in such situations carbs don’t help much, presumably as they are sucked into muscle? (if otherwise glycogen depleted).
So I either reduce intensity/duration (probably) to avoid presumed hypoglycaemia. In your opinion can I assume that whilst glycogen depleted in muscle that hypoglycaemic episodes (due exercise intensity/duration) are impossible to counter without (relatively massive) CHO intake as this will be be preferentially taken up by muscle?
In summary in such circumstances (VLC/low glycogen and not feeding during exercise), exercise intensity/duration should be such to minimise glucose utilisation?
In all other respects the effect of increased exercise volume on adiposity has been beneficial 😉
If you’re not using a very high quality BCAA, I’d recommend it. Mental acuity while exercising may be as much to do with specific amino acids as it is hepatic glucose output, as crazy as that sounds. In other words, a few well-timed BCAA may preserve brain function even as HGO decreases.
Thanks for the thought provoking blog.
If you have underestimated your glycogen stores, and did not replenish adequately, your insulin should be low. So, your body would give up the lipids from your adipose cells, they go to to your liver to be made into Ketone bodies. At the same time, with insulin low, would your liver not start up gluconeogenesis overnight, to get your blood sugar higher? So that you would get up in the fasted state with increase BHB and normal(not low) blood sugar?
It depends on the extent of the deficit.
Wait a minute! Wait just a darn minute! What about the “last chance workout” on the Biggest Loser. Would a contestant be wise to sit out the “last chance workout”? What great drama that would be, great TV! Bob would blow a casket!
Of course what they probably do is just don’t drink any water that day or night until the weigh-in. Boy that must be good for an inflamed body to be dehydrated.
Peter, thanks for the info…
I race mtb ultras and recently did a shorter event of 52 miles here in Steamboat. Was in ketosis for 10 days (av 1.4mM) and did light carb loading two dys out (500g total) mixed with lots of fat, big steak dinner night before. Then I fasted the morning of the event (til 8am). According to my ketostix I was either out of ketosis or almost.
I raced the whole event on just water, bullion cubes, and BCAAs. This was a particularly hard event (5hr 19min, 6000cal burn, 85-90% of MHR) and I beat my times from years past. Post race my ketone levels were well above 3.0mM.
It seems that once my body is adapted, when faced with the effort such as the race, it wants to burn fat and will spare the glycogen even with ketone levels reading low.
Good stuff!
Wow, Jeremy. What’s amazing here, if I’m reading this correctly, is that you were only in ketosis for 10 days prior to the race? That’s shocking. 10 days after being in ketosis I could barely walk up a flight of stairs. Obviously, you did a MUCH better job of getting there than I did back in the spring of 2011.
Great information, always look forward to your posts and appreciate your time invested on this site.
A question of less technical detail, is your hummus recipe a closely guarded secret or is there a chance you might share it?
Kind regards,
~L
I’d happily share it Lynn, except no two batches are the same. You see, I grew up in a restaurant and my father is probably the best chef I know. Never used a recipe in his life. So I sort of learned it the “old” way… a touch of this, and pinch of that. Here is the basic philosophy:
Blend chickpeas in an uber blender (e.g., Vitamix) with enough lemon juice and hot water to keep it mixable. But leave it a touch lumpy. Add salt, pepper, garlic puree or powder, olive oil, cumin, coriander, more lemon juice than you think reasonable, sesame seed paste (tahini). I wish I could explain how I do it, or what taste I’m looking for, but I guess having done it since I was 10 prevents me from explaining it well. Hope this helps.
Hi Peter,
Your blog is amazing. As a low carb eater (for the past 15 to 20 years) and weekend warrior plus (10 hours a week of mountain biking, hiking, yoga and weights), I can’t thank you enough for dedicating your career to this research, and keeping us readers up to date about your self-experimentation.
In your posts, I dig through your every sentence, looking for morsels.
During my hike last night, I was fixated on this:
“Since I’m not a model and nobody cares if my body fat is 7% or 10%, I’m happy to be a little less lean if it gives me the flexibility to increase performance and live a slightly more sane life. At least for now.”
I think you and I are about the same size. At 5’10”, I pretty much choose my weight between 153 and 159.
153 is Skeletor – skipped meals, obsessive attention to carbs and protein (29 inch waist, ribs sticking out).
159 is a lazy upper limit, where I over-eat protein and munch nuts with abandon (31 inch waist).
156 is a happy place, but still requires serious attention to diet details.
This bit from the EPIC trial in Europe left me wondering. Waist measurement correlates inversely with mortality.
https://www.nejm.org/doi/full/10.1056/NEJMoa0801891
On the other hand, I believe a previous publication from the same data set, focused upon BMI, showed the low end of the scale turning J-shaped. Among male non-smokers with extremely low BMI (can’t seem to find that right now) , extremely low BMI was associated with an increased risk of early death in men (but not in women, interestingly). But we are talking super-low BMI – 19, 20, 21 range. I suspect they suffered undocumented comorbidities.
Is it possible Skeletor is a healthier weight (and worth the craziness)? Can you propose a possible mechanism arguing one way or the other?
Charlie, these waist/BMI papers don’t apply to someone like you. The investigators, in their defense, are trying to find some simple yardstick to measure risk by. But you’re already way out of their target zone. Besides, there are FAR better ways to predict risk if you have access to lab testing. E.g., CRP, LDL-P, TG, OGTT.
Peter: I always assume that alcohol (wine) goes into the carb percentage of calories. I am generally about 65%-75% of calories from fat, with the remainder evenly divided between protein and carb – and the carbs include a glass or two of wine about four or five days a week. Do you agree wine would go into the carb percentage?
If you can isolate them. A glass of dry red wine (my choice of EtOH) is only about 4% sugar by weight, so very little. The actual source of calories is the alcohol itself. It’s probably only the case in beer and sugary-drinks that the CHO content starts to “count.”
Great article. I’m so glad I don’t have to fear the chickpeas (in moderation I suppose). Thanks Peter.
Thanks for answering, Peter. I think I’ll stay away from the Skeletor look for a while. It doesn’t seem worth the trouble.
Keep up the great work!
As always, very thorough. I’ve lost to date 100 lbs on the LC – VLC way of eating, over about three years. I stumbled through it painfully without really knowing what I was doing. I’ve read and read and read. I mange to get lucky and lose weight. My wife and others who are very interested in becoming “more-less-obese” struggle understanding any of it and my wife can’t seem to lose anything. She’s been on nothing but meat and fat for two weeks now. Others I work with, as is always the case in my experience, want/need to lose weight, but don’t read much and can’t follow these kcals, ncal and %cho (oh my!).
My question is this: Where’s the “for dummies” version? Most people I know don’t read Med Journals or sentences with formulas that contain numbers AND letters. Is there a guide for the fat and simple? And what happens when their cells are insulin resistant? (Did I say that right?)
Your work and attention to this problem captured my attention and I think your work may make the nutritional and medical society take note of the wrong information out there. Keep up the great work. It sucks being obese and not being able to do anything about it because of lack of effective information.
Good question. I don’t really know. My fear with the “for dummies” stuff is that it (obviously) simplifies things. Sometimes this is very good, but other times it can be counter-productive. I think great teaching requires the ability to know when to go simple vs. complex.
How about “The New Atkins for New You” by Westman, Phinney and Volek?
Peter,
Re. restricting protein intake to attain NK – Am I right to assume that anything above 120g/day would cause the body to manufacture glucose through gluconeogenesis, thus inhibiting production of ketones?
The `rule of thumb’ for strength training seems to be around 2g/kg a day of protein for building muscle, so adopting that for anyone weighing more than 60 kg would seem to rule out NK.
It would be tough to stay in NK while consistently consuming over 120 gm/day of protein, but as this post suggests, context is everything.
This is a timely post. I committed to low-carb about three weeks ago and have noticed a big difference–at age 36, I now know that what used to work doesn’t work any more (I have been eating low-glycemic over the past year). I’ve dropped six pounds and had no noticeable bloating during PMS (I know–fun topic–but the bloating has been getting so bad that I looked like I was pregnant). The only reason I knew I was retaining water was because my ankles were very slightly swollen–a major improvement. I do not meet the criteria for metabolic syndrome–all levels are good, I’m just heavy (187).
I’ve been laboring over tonight–my friends and are doing an urban ride and we’re meeting at a brewery that only serves pizza–and damn good pizza. I don’t think they serve whole wheat or even gluten-free, so I think the crust will be the highest in carbs it can. It’s a 10-inch pizza. At this point, I think I’m just going to load it up with protein and fat and enjoy. After all, it’s a rare occurrence, and rarely do I not have the option for a low-carb alternative when I go out to eat. My only worry is that we’re tackling a grueling trail for tomorrow’s mountain bike ride, and I suspect that I would do much better if I didn’t have the pizza (okay, AND the IPA). I fully-expect to be out of ketosis.
My question is, *if* I’m keto-adapted, so this could be hypothetical given my short time with low-carb, does that require another induction phase, or does the body bounce back into it within a couple of days of a cheat meal. Do people who do one cheat meal per week (*not* what I want to do) after induction ever become keto-adapted?
Probably depends on the nature of the meal and the time you’d previously been in ketosis.
I had the pizza, but then we did our pub crawl the next day and I singlehandedly kept the IPA industry in business. The next day, I had trace amounts of ketones in my urine and it stayed that way until this past Friday when the ketone strip turned a couple of shades darker, which made me happy because I had a 37-mile mountain bike ride yesterday (Saturday). I then had three pints of IPA and a nine-inch pepperoni pizza. This morning, my ketone strip was between the lowest two positive shades, which I’m taking as a good thing, but I’m also thinking tomorrow’s will give a fuller picture.
Regarding the ride, I made it through on 36 almonds while my friends were stuffing down Cliff bars and PB&J sandwiches. I did have great difficulties on the final multi-mile climb, but it was because I ran out of water earlier–easy problem to solve. I guess you can say that I had a water-bonk. I bonked last year, so I’m well aware of what it feels like to need more carbs. That absolutely was not an issue this year. For this reason, I am sold on low-carb for endurance sports. Also, the most I’ve mountain biked this year is 15 miles. To take on a 40-mile ride like I did yesterday is gutsy, but I firmly believe the low carb diet allowed me to tap into my reserves to keep going. Post-ride: no headaches, no lethargy, no physical heaviness. I was bright, happy, and while I certainly felt like I had completed a hard effort, I generally felt awesome.
I think what might help is that when I do eat something higher in carbs, I try to preemptively counteract it with protein and fat. I guess you could say that I’m trained to do this because I was on a low-glycemic diet prior to going low carb.
I just wanted to report back since this seems to provide a bit of an answer to my original question, and maybe it will help someone else. 🙂
Hi Peter,
Thanks for a great website. I have been reading-up on your cholesterol series–as a part of that I jumped over to lecturepad to check out some of the other info on cholesterol etc. One of Dr. Dayspring’s case studies (lipidaholics-case#291) discussed how pratictioners see a large number of “low-carbers and paleo” patients who see a worsening of their lipid profile–alarmingly–the increase in LDL particle #. Have you seen this case presentation? do you have any comments about it?
I have been doing a low-carb to very low carb, high fat diet for the past few years –primarily to stay weight stable and keep insulin levels low as I am IR(hx of pcos)—this case study really alarmed me in that it was the first time that I heard of some of the possible down sides to doing this type of regime. I know that this particular patient got things back under control by lowering saturated fats and adding some carbs back to her diet–while still staying low carb. Any comments would be greatly appreciated.
Yes, I reviewed it as Dr. Dayspring wrote it. I’ll address in Part X of my series when I get a chance to write it.
Hi Peter,
I have been in a LCHF from 2008 and still going strong. Diet has suited well for my strength training workouts and have made some personal records. Now I started hockey training which is much intensive (my average pulse for one hour game is around 160 per minute), What should I eat before hockey training? Should I eat/load carbs right before training or only after? Or does carbs before training just disturb fat burning “engine”?
Thanks,
Ripa
You will likely require CHO to maximize your performance in a game like hockey, especially at the intensity you describe.
Hi Peter,
Thanks for another great article.
What is your take on cortisol in terms of weight gain and plateau as compared to insulin?
How far is it true that being in ketosis over a long period of time can cause the body to increase cortisol levels that can cause plateau or weight gain?
Increased cortisol can certainly reverse or retard fat loss, though I’m not impressed with evidence implicating a low carb or KD. But if one is worried about it, it’s easy to test: change diet and observe change in fat and cortisol level.