Alternative Hypothesis
Obesity is a growth disorder, just like any other growth disorder, and fat accumulation is determined not by the balance of calories consumed and expended but by the effect of specific nutrients on the hormonal regulation of fat metabolism.
§
Calorie
A calorie is a unit of measurement for energy. That’s it, really. By formal definition, a calorie is the amount of energy required to raise one gram of water from 14.5 to 15.5 degrees Celsius at atmospheric pressure. One-thousand calories = 1 kilocalorie, or a kcal, for short. Here’s where it gets a bit tricky. Most people use the term “kilocalorie” and “calorie” interchangeably. So when someone says, “A gram of fat has 9 calories,” they actually mean 9 kcals. The important thing to remember is that a calorie (or kcal) tells you – in the case of food – how much energy you get by burning the food. Literally. In the “old days” this is how folks figured out the energy content of food, using a device called a calorimeter. As a general rule, carbohydrates have approximately 3.4 kcal per gram; proteins also have approximately 3.4 kcal per gram; fats have approximately 9 kcal per gram.
§
Carbohydrate
Carbohydrates are one (of three) classes of what we call “macromolecules,” the other two being fats and proteins. [Some argue alcohol is a fourth class.] They are organic compounds consisting of carbon [C], hydrogen [H], and oxygen [O] atoms, and they fit together (almost always) in the form of Cm(H2O)n, where m and n are integers, either the same or different. For example, glucose, which is a very simple carbohydrate consisting of a single ring of 6 carbons has the formula C6H12O6.
The more important point is that carbohydrates can be “simple,” as in the case of glucose, which is just one ring of six carbons (one ring, gives it the subclass distinction of being a “monosaccharide”) or fructose (also a mono-saccharide of 6 carbons, but only 5 in the ring structure). They can also be slightly more “complex” 2-ringed structures (you guessed it, “disaccharides”). With increasing numbers of rings – “complexity” – they take on broader names like oligosaccharides and polysaccharides. The complexity is often inversely correlated with how quickly they lead to a rise (and fall) in blood glucose levels. In other words, it’s usually the case that the more simple (i.e., smaller) a carbohydrate, the quicker it gets into the bloodstream, and the quicker it elicits an insulin response.
Our body breaks carbohydrates down into smaller molecules, most of the time into the smallest version possible, and with the aid of insulin aims to store them as either glucose or fatty acids.
§
Fatty acid
Fatty acids are a subset of the sort of waste-basket term “fats.” Specifically, a fatty acid is a chain of carbon atoms with a specific end called a “carboxylic acid.” While fatty acid metabolism and nomenclature is one of my favorite topics on earth, it’s also one of the most cumbersome. For the sake of simplicity, let’s just deal with the basics: fatty acids can be “saturated,” which means there are no double bonds between any of the carbon atoms (i.e., every carbon atom is “saturated” with hydrogen atoms); they can be “monounsaturated,” which means they have only one double bond in the entire carbon chain; or they can be “polyunsaturated,” which means they have at least two double bonds in the carbon chain. Polyunsaturated fatty acids are typically further subdivided by the location of their first double bond (omega-3 versus omega-6, for example). Of course, further complicating this is the fact that, in addition to all of the different bond locations, they can have different numbers of carbon atoms.
Here’s the 30,000 foot view: fatty acids have a few destinations in our body worth mentioning. One – we can burn them for energy via a process you’ll hear me refer to often called “beta-oxidation.” [This process yields more energy than any other metabolic process in our body.] Two – we can store them in their storage form, triglycerides. Three – we can use them for important structural functions in our body, perhaps most notably making cell walls (“membranes”). Four – we can make other things out them that act as important signals in our body. Five – we turn the excess carbohydrate we eat into fatty acids (and this is a so-called metabolic one-way-street: once you turn carbohydrate into fat, you can’t turn it back into glucose).
§
Glycogen
Glycogen is the storage form of glucose in our body. Unfortunately, many people (like me) use the term glycogen and glucose almost interchangeably. But they are, technically, distinct. Glycogen can be stored in either your liver, where we can store around 100-120 grams worth, or your muscles, where (obviously, depending on the size of said muscles) you can store up to roughly 300 grams.
There is an important distinction to make between these two storage sites. The liver contains a special enzyme called glucose-1-phosphatase, which enables glycogen to be broken down entirely to glucose, and therefore exported from the liver into the bloodstream. The muscle does not possess this enzyme. Hence, glycogen from the liver is available to the brain as glucose. Glycogen from the muscle is not – it must be used by the muscle.
Final point worth mentioning: As you can see our ability to store carbohydrates (as glycogen) is quite limited in capacity. This is partially why carbohydrates are so fattening. Most people consume carbohydrates far in excess of their storage capacity. What can’t be stored as glycogen, or immediately used, gets stored as fat in the form of triglycerides.
§
Insulin
Insulin is a hormone secreted from the pancreas. The cells of the pancreas that secrete insulin are called “beta cells,” and they actually represent a fraction of the mass of the pancreas (less than 5%), though they are vital to our survival. [Technically, the beta cell doesn’t secrete insulin, per se, but rather a precursor to insulin, but this detail is only rarely significant.] Insulin is what we call an “anabolic” hormone, meaning it’s a hormone that helps “build” things (e.g., helps get amino acids into muscle cells, gets glucose into cells). It plays a primary role in how our bodies handle carbohydrates, fats, and proteins – though most people primarily associate insulin only with its role in carbohydrate metabolism.
There is no shortage of stuff to read (e.g., entire textbooks) on insulin, so I won’t even attempt to reproduce it. Let me try to give you the most important info:
- Insulin facilitates the delivery of glucose from the bloodstream into cells. Insulin engages with a receptor on the cell surface (conveniently called the insulin receptor). This creates a signal inside the cell that culminates with a structure (think of it as a tunnel) called GLUT-4 (pronounced “glute-4”) inserting itself in the membrane of the cell to allow for glucose to enter the cell.
- Insulin also up-regulates (i.e., makes more of) an enzyme on the surface of fat cells, called lipoprotein lipase (LPL). LPL, when on fat cells, brings fatty acids into the fat cell to store them at triglycerides. In other words, insulin promotes the storage of fat in fat cells. Similarly, insulin down-regulates (i.e., reduces) LPL on muscle cells. This reduces the ability of muscles to access fatty acids for oxidation (i.e., the prevents muscle cells from burning fat).
- Insulin also promotes the storage of glucose in the liver and muscle as glycogen, provided there is “room” to store them. Both the liver and muscle have a finite, and relatively small, storage capacity for glycogen (see, above).
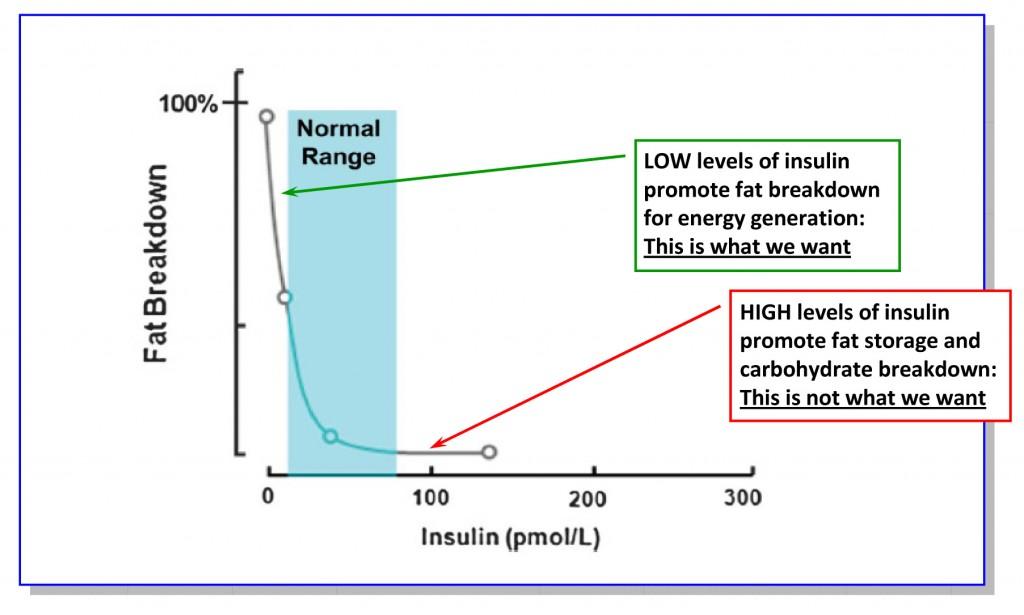
If you remember nothing else, remember this: insulin plays the central role in fat metabolism. When insulin levels are elevated, the body goes into “storage” mode – not just of carbohydrates but also fat. In other words, elevated levels of insulin turn off the ability of the body to burn fat. This is why people are insulin resistant are typically overweight. Insulin resistance (see, below) almost always leads to a tonic state of hyperinsulinemia (high insulin), and hence, always storing fat, rather than breaking it down.
If you ever forget this point, just look at the figure below:
- High insulin – store fat/don’t break it down
- Low insulin – break down fat/don’t store it
§
Insulin resistance
As the term implies, insulin resistance (IR), involves the tissues of the body (especially muscle cells and fat cells) becoming resistant to the effect of insulin, thereby requiring greater and greater amounts of insulin to achieve the same outcome – namely regulation of glucose in the blood. There is no shortage of discussion and debate about both the cause and mechanism of IR. I enjoy discussing both of these concepts ad nauseam, however, I’ll refrain from doing so here.
Remember this: when you are insulin resistant, you need more insulin to do the same “job.” This is bad for at least two reasons:
Chronically elevated levels of insulin – in and of itself – leads to a non-favorable metabolic state of fat storage over fat oxidation (i.e., storing fat instead of burning it).
In many people, IR leads to diabetes, as the pancreas eventually fails to “keep up” with the demand for insulin. So while insulin levels remain high, blood glucose also remains high. This is called type II diabetes.
§
Ketosis (or keto-adaptation)
Ketosis is a state, achieved through significant reduction of carbohydrate intake (typically to less than 50 grams per day), at which point the body makes a fundamental change from relying on glycogen as its main source of energy to relying on fat as the primary source of energy. In particular, the brain shifts from being entirely dependent on glucose, to being primarily dependent on beta-hydroxybutyrate – a so-called “ketone body.” Ketone bodies are chemical structures made by the liver (also somewhat in the kidney) out of fatty acids, primarily.
Whenever one has a discussion about nutritional ketosis, it’s always important to distinguish it from a pathological state referred to as diabetic keto-acidosis (DKA), which I describe in more detail in an in-depth FAQ post.
§
Metabolic syndrome
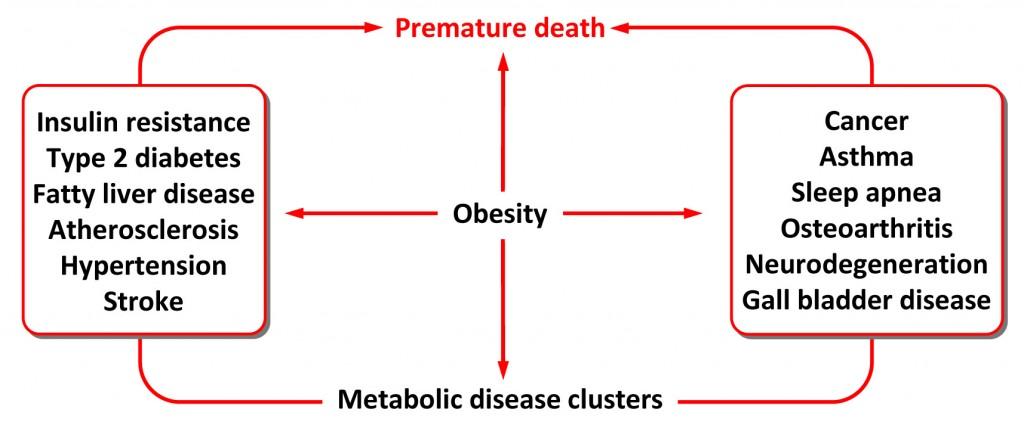
Formerly referred to as “Syndrome X,” this syndrome is classified according to a number of criteria, many of which differ slightly between organizations. You can read about it in exhaustive detail here, but the essence of metabolic syndrome is as follows: obesity, a bad lipid profile, and insulin resistance.
There is no longer any dispute in the medical community as to what having metabolic syndrome leads to. The figure, below, summarizes this. The debate ensures around what causes it (and, therefore, how to reverse it).
§
Ordered terms
The important features of a problem, in relative order of importance. An example will make this clear: If someone is on a sinking ship in the middle of the ocean, the first-order term (or requirement) is finding a lifeboat with oars. The second-order term is securing an adequate supply of fresh drinking water. The third-order term is having sufficient food to eat. The fourth-order term might be finding a map of nearby islands. And so on. The tenth-order term, by extension, is having a high quality pair of polarized sunglasses. I am not suggesting that being on the ocean for days without good sunglasses would be pleasant — it would be miserable — but it’s nowhere near as important as having a boat, water, and food.
§
Sugar
The term “sugar” is typically reserved for a subset of carbohydrates called monosaccharides and disaccharides (see definition of “carbohydrate,” above). While most folks associate the word “sugar” with white crystals they put in their coffee, the term is much broader. That said, great confusion arises when folks (including me) use terms like, “blood sugar” and “glucose” interchangeably. For this, I apologize.
Rather than explain what each and every sugar is, I’ll call out a few popular ones. Glucose is a 6-carbon ring that is the final common breakdown produce of most carbohydrates. Fructose is a 5-carbon ring (with another carbon hanging off) that is actually much sweeter than glucose, found naturally in fruit, but unique in that only the liver can metabolize it. Sucrose (i.e., table sugar) is a disaccharide formed by a 50/50 mix of glucose and fructose. High fructose corn syrup (HFCS) is essentially the same as sucrose, except instead of being a 50/50 of fructose and glucose, it’s 55/45). Lactose, found primarily in milk, is a disaccharide formed from glucose and another monosaccharide called galactose.
§
Triglyceride
Triglyceride (abbreviated TG or TAG, for triacylglyceride) – is the storage form of fatty acids. Triglycerides are made of up three fatty acids linked to 3-carbon molecule called glycerol that acts as a sort of backbone. While triglycerides are stored in fat cells (called adipose cells or adipocytes), they also circulate in the bloodstream, and are easy to measure. Obviously elevated levels of stored triglycerides are harmful (i.e., excess fat stored in fat cells), but so, too, are elevated levels of circulating (i.e., in blood) triglycerides. In particular, when circulating triglycerides are made up of saturated fatty acids, there is evidence of harm. Contrary to what people think, eating saturated fat does not increase saturated fatty acid content in triglycerides. In fact, reduction in carbohydrate intake, coupled with increased saturated fat intake, actually lowers both circulating triglycerides and the amount of saturated fatty acid within triglycerides. Unfortunately, most doctors don’t realize this and they tell patients with elevated triglycerides to reduce fat intake. Ironically, this is the wrong treatment.