
Check out more of my recent content on COVID:
- (January 3, 2022) COVID Part 1: Current state of affairs, Omicron, and a search for the end game
- (January 23, 2022) Why I’m for COVID vaccines, but against vaccine mandates.
- (January 24, 2022) COVID Part 2: Masks, long COVID, boosters, mandates, treatments, and more
- (January 29, 2022) A follow-up to my article on vaccine mandates
If you are reading this, then you’ve made it beyond the title of this newsletter! Congratulations – I’m sure the subject elicited more than a few eye rolls among my readers.
Yes, this week we’re giving you more content about COVID. (The last of it, I hope. Really.) Why? Because in last week’s newsletter on vaccine mandates, I implored you all to think. Many of you rose to the occasion with insightful feedback – both positive and negative – which absolutely merits additional discussion.
I was also surprised by two particular themes of feedback, both of which I received in spades:
“I was strongly in favor of vaccine mandates, but after reading your argument, I have changed my mind. Thank you for taking the time to walk through your argument in such detail.”
–and–
“I agree with your assessment, and I think vaccine mandates are a bad policy, but I can not say so publicly because I need to stay out of thorny political issues. Sorry I can’t also speak up on this.”
I appreciate this feedback (though I remain confused by the second of these, as this discussion was centered on scientific evidence, not politics), as well as the thoughtful comments and questions about the limitations of the points I made last week. I’d therefore like to spend a little time drawing attention to some of these questions and giving them the careful consideration that they deserve.
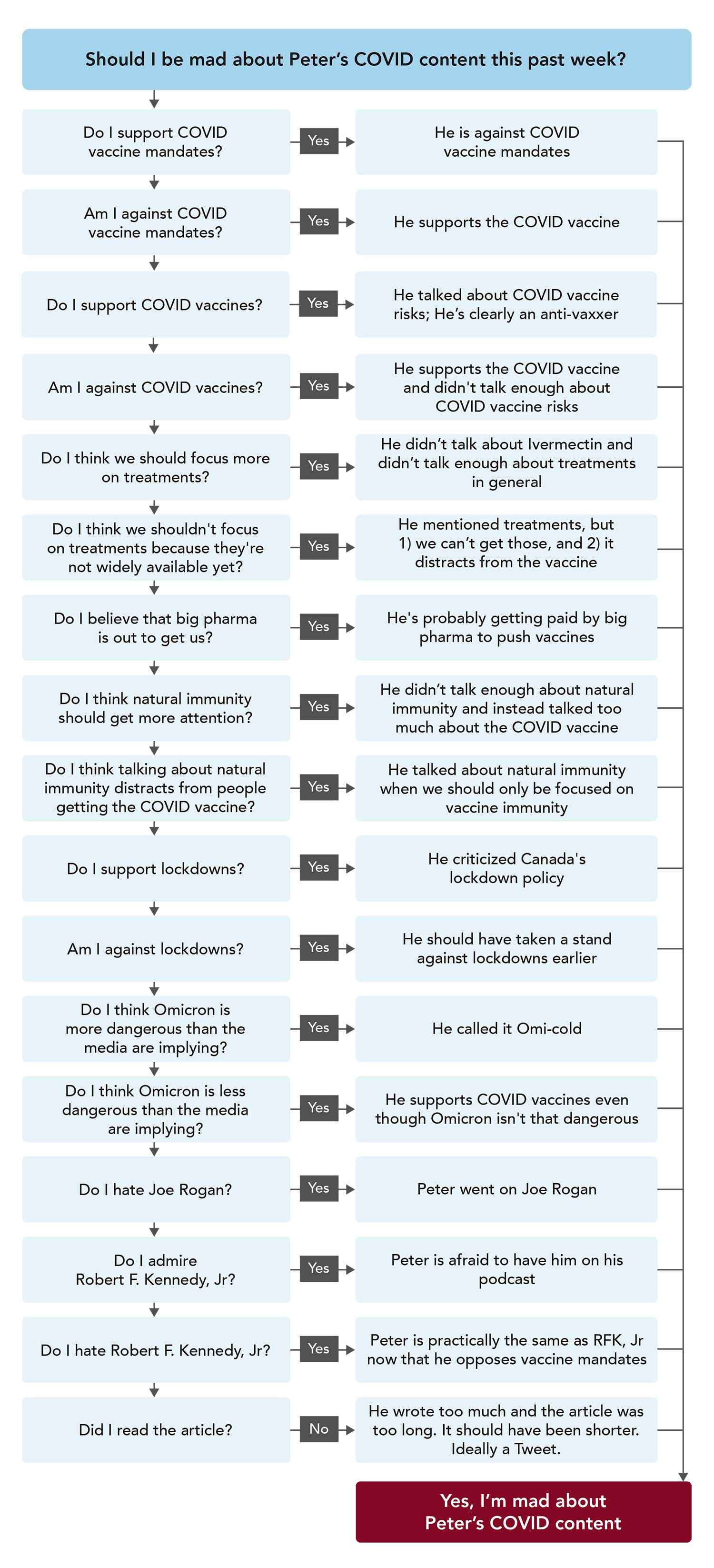
…But before we do, let’s take a look at the *other* feedback. In weighing in on such a charged issue, I expected to have to fight a few battles along the way. In fairness to all viewpoints – after all, the internet tells us that Twitter agitators have just as much authority as medical experts, and we all know the internet is never wrong – I’ve decided to present some of these criticisms, too, and have asked my team to make a handy flowchart to organize the various lines of thinking.
OBSERVATION 1
… My inbox this week might be the closest I’ve ever come to experiencing a blitzkrieg. And yet here I am, returning to this subject, ready for the air raid sirens to start blaring all over again as soon as I share this.
OBSERVATION 2
In all seriousness, we received some really great follow-up questions from people who (i) actually read the piece in its entirety and (ii) were versed in the novel technique of disagreeing with the argument I made without reverting to ad hominem attacks. This relatively new technique is called making-a-counter-point-that-focuses-on-the-arguments, whereby they made counter-arguments in good faith to the actual points I raised.
Here are some examples:
1. You’ve neglected to acknowledge that the decision not to vaccinate oneself can potentially impact others. You discussed the relative likelihoods of vaccinated vs. unvaccinated individuals becoming infected and potentially passing the virus along to others, but infection isn’t the only way in which the vaccination decision has broader repercussions. As you pointed out, anti-vaxxers are more likely to be hospitalized or die of COVID, so a “my body, my choice” viewpoint doesn’t apply when one’s personal decision can impose a massive burden on the healthcare system. As an example of an even more profound and personal impact, we could look at anti-vaxxers who have left their children as orphans after dying needlessly of this disease. How is that not reprehensible?
I think this is a fair criticism of my argument. With regards to children becoming orphans because their parents died from COVID while unvaccinated, I have no idea how large that data set is. I guess the only silver lining around this is that the people most harmed by not taking vaccines are, typically, sufficiently older, and therefore hopefully not people with young kids. People in their 30s and 40s, even if unvaccinated, are still at very low risk from COVID (even from the original strain). But no doubt there are some young kids out there today who do not have parents because of this, and this is no more or less tragic than a child losing a parent to any preventable cause of death.
Of course, the same can be said of so many other things that take so many more lives than COVID will ever take. How many parents have died because they didn’t manage their lipids and ended up with premature cardiovascular disease? How many were killed driving drunk or speeding or by others doing so? How many took their own life by suicide or overdose? The answer here must be multiples of COVID. We could certainly enforce mandates to address these things (e.g., forcing statins on people with LDL-C > 150 mg/dL; banning alcohol entirely; forcing automakers to prevent cars from driving more than 60 mph), but is that the world we want to live in?
A similar argument applies to burdens on the healthcare system. Those who chain smoke or drink to excess are increasing their risk of disease and death. Yes, certain high-risk behaviors come with higher health insurance costs to offset the added burden, but that is very different from entirely removing the right to engage in these behaviors. And what about athletes? Team sports and other athletic endeavors frequently cause fractures, sprains, and other sports-related injuries – many involve significant healthcare costs, but we’d never forbid these activities or penalize athletes for engaging in them.
2. You don’t clearly acknowledge that your argument against mandates would fall apart in the presence of a more deadly virus—while rampant misinformation and vaccine resistance would probably still flourish. Given a sufficiently deadly pathogen, we’d vaccinate everyone at gunpoint if necessary—and we’d be right to. So, while I agree with your position on mandates, especially given the turn that Omicron has taken, I feel that we are set up to fail massively in the presence of a more dangerous pandemic.
I mostly agree, and the first version of the vaccine newsletter did address this exact point. I removed it because the piece was, and probably still is, too long, in my opinion. I went through the argument for other vaccines and touched, specifically, on the measles, mumps, & rubella (MMR) vaccine. Essentially, the point I made was that each vaccine-disease pairing must be evaluated separately. It must address the following questions:
- How effective is the vaccine at reducing the severity of the disease to the vaccinated individual?
- What treatment options exist for the infected?
- What are the consequences of infection, beyond death (that is, what is the morbidity for the survivors)?
- How well does the vaccine prevent transmission? (Here, for example, is where MMR is very different from COVID because of the nature of measles vs. SARS-CoV-2. Measles requires a long incubation, 10-14 days typically, and spreads only once virus is present in the bloodstream, so vaccines virtually eliminate spread. This is, of course, not at all true of COVID vaccines, because the virus causing COVID incubates for a much shorter time and does not require viremia to spread, which is why it spreads so easily and quickly via mucosal surfaces.)
So I would argue this is another reason to oppose mandates for this virus with these vaccines and this time. A mandate is a very extreme measure; therefore, it should be reserved for cases in which it really moves the needle. It clearly does not move the needle for COVID – currently, at least. The scientific community and health policy community have already squandered most of their good will. By ramming mandates down people’s throats in a scenario when they help virtually no one, they effectively torch the chance to go back to this nuclear option if and when it is ever truly justified.
The last point I would make is that I’m not sure we would need to force effective vaccines at gunpoint if a mandate truly made sense. If we were dealing with a virus that killed 10% of the people it infected, that spread as easily at COVID, and for which we had no treatments, I suspect people would be lining up for vaccines once they saw, with their own eyes (which they would undoubtedly see if 1 in 10 were dying) the toll of the virus on the unvaccinated.
3. You say that Omicron is milder than Delta and previous variants, but daily death rates from Omicron are as high as they have ever been.
This is a fair point. I think there are two things to keep in mind when evaluating the daily death toll from Omicron. First, what you are witnessing with this death toll can’t be compared directly to the previous variants because Omicron is much more contagious than Delta, so the velocity of disease is much greater. In other words, it’s not just that more people are being infected, it’s that the entire population will be exposed to this in a much shorter time frame. So if a previous variant of COVID might be expected to kill X people over 2 years, this one might kill 25% of X people (because it’s less virulent), but over 3 months instead of 2 years because of the speed at which it spreads. Second, in looking at the daily death toll–and to be clear this is a hypothesis that can only be tested once we have all of the mortality data, on a daily basis, for every cause of death in the U.S.–I suspect the daily numbers we are seeing today include two groups of patients: people dying because of Omicron and people dying from some other cause (e.g., cancer, ASCVD) who tested positive for Omicron incidentally. Obviously, only the former should be included in the death toll, but the only way to know the size of the latter is to look at excess and deficit deaths during this peak period, which will take some time. My intuition is that this latter group represents a nontrivial fraction of the COVID deaths we are seeing.
OBSERVATION 3
A few people commented on my calculation of the NNT (number needed to treat, or NNV–number needed to vaccinate) for the vaccines, arguing that such a calculation was misleading.
Some comments were in good faith (the novel technique described above).
Some comments were based on a different technique, which I believe is called the If-I-call-you-a-big-enough-piece-of-shit-who-misrepresnts-data-for-personal-gain-it-makes-me-feel-better-about-myself technique.
For those hoping to emulate the former, here is an example:
You list the ARR for ages 65-74, for example, as 0.035%. This review of over 100 studies reports the infection fatality rate (IFR) at age 75 as 4.6%. (Subsequent data like these and these have found a similar if somewhat lower range, presumably after natural immunity had provided some protection.) If the RRR is 84%, then I think the ARR should be 4.6% X 0.84 = 3.86%, for a NNT of ~26.
The study you’ve cited looks at an entire population and asks what is the ARR prior to any infection, whereas my analysis looks at IFRs (i.e. what happens if you are already infected and unvaccinated vs. already infected and vaccinated). However, given that the high likelihood that unvaccinated individuals would be infected at some point in their lifetimes, the difference of looking at a total population vs. infected population would result in only a small change in NNT.
I have been trying to see where I am wrong, either in my understanding of the age-specific IFR or in the calculation of NNT. Given the relative efficacy of vaccines, and the fairly high IFRs at older ages, the ARR should be more appreciable than 0.035%. Apologies if I am mistaken.
(Note: For those who would rather emulate the latter technique, check out this app called “Twitter.” It has an accredited fellowship program which focuses on all the fine points of this style of inquiry.)
I think there is a point to this argument. Upon some further reading, and after reaching out to 5 epidemiologists, 2 virologists, and 3 biostatisticians, I think I would say that the NNT calculation I included, while correct “technically” (it is, after all, the reciprocal of the ARR) does not fully capture the benefit of vaccines. In other words, I understated the value of vaccines, when it comes to preventing hospitalization and death in absolute terms.
Here is an interesting letter I was sent by one of the people I reached out to on this question and here is another interesting piece that explains the limitations of using NNT (or NNV) to estimate the effectiveness of vaccines. My takeaway from digging into this more closely is that the roughly 6 months of follow-up in the VA trial, despite its size of over 4 million patients, did not give enough time to see the full difference in mortality and hospitalization between the groups (unvaccinated and vaccinated). Giving enough time for every single person to be exposed to COVID, however long that takes, would be necessary before we can apply the ARR/NNT framework.
There is, of course, a great irony in this mistake. You see, it makes the argument for vaccines even better than I initially made it. This implies (based on the formal tools of logic) that the rationale for mandates is even weaker. After all, my argument against mandates is:
- Vaccines do a great job of protecting the vaccinated [correcting the NNT argument now makes this a stronger case];
- Vaccines do a poor job of preventing transmission;
- We have very successful treatments–both new drugs and one old drug–to treat COVID;
- Natural immunity is, at a minimum, as good as vaccine immunity and with each passing day the fraction of people who are not immune, via infection and/or vaccine, is shrinking precipitously; and
- Omicron is less virulent than all variants that preceded it and will eventually infect everyone, with or without a vaccine, thereby providing an excellent booster.
This is a good example of “majoring in the minor” as one of my professors used to say (as opposed to “majoring in the major” and “minoring in the minor”). Several people who were very upset about my analysis and conclusion were especially upset about this low estimate of NNT, but most failed to realize that this error was not germane to the overall argument and that correcting this mistake makes the argument stronger.
OBSERVATION 4
This is less of an “observation” per se so much as a follow-up for the sake of transparency and thoroughness. I recently shared the graph below on social media, and for those who might be interested in looking into this further, I wanted to share additional details about my sources for these data, as well as a limitation of this type of analysis.
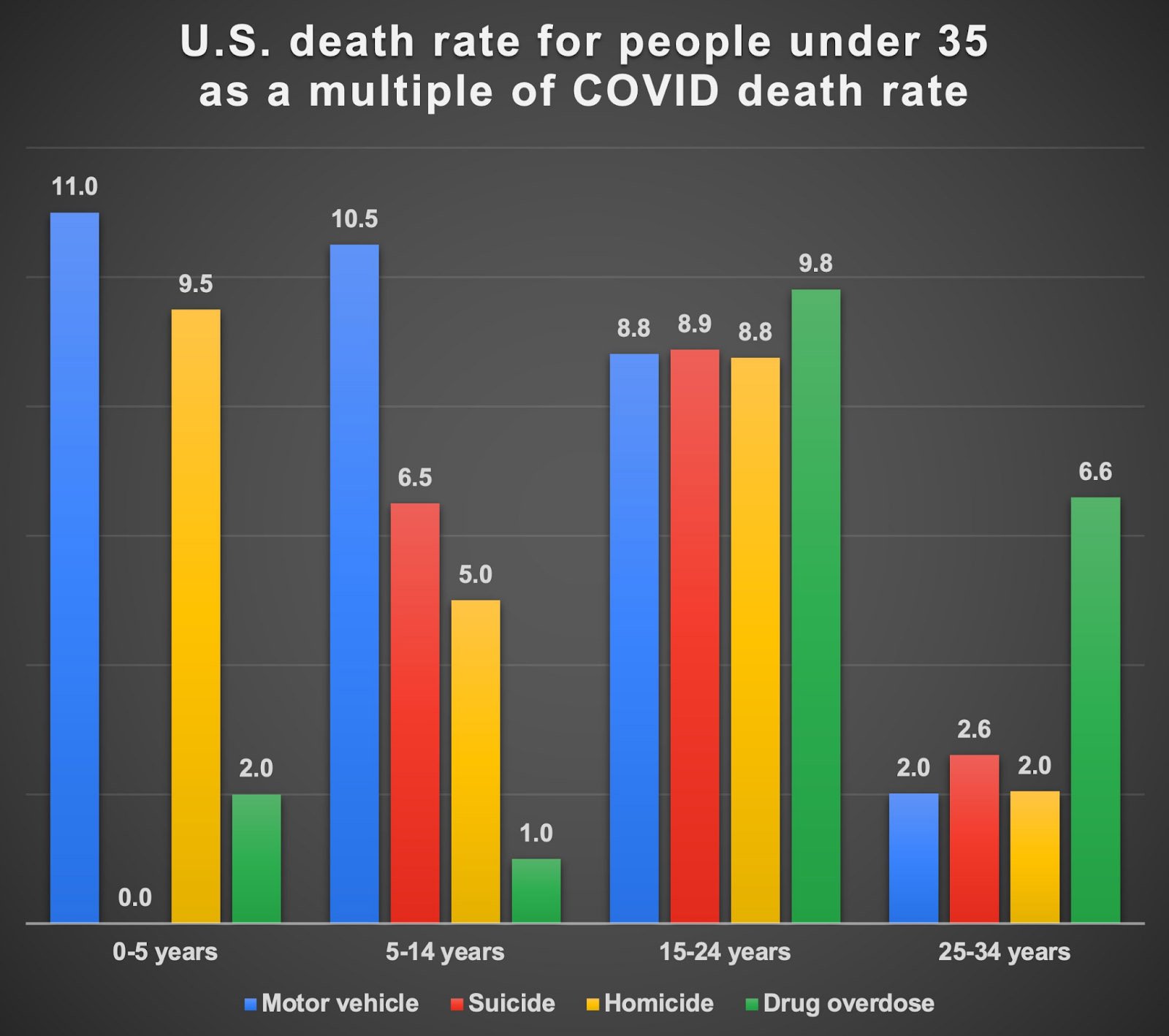
Data for annual U.S. fatalities attributable to suicide, homicide, drug overdose, and COVID were sourced from the CDC, while the National Center for Health Statistics (NCHS) provided data for annual U.S. fatalities from motor vehicle accidents. For suicide, homicide, and drug overdoses, crude death rates were calculated from a 12-month period ending in Q3 of 2020. Motor vehicle-related death rates were calculated from a 12-month period ending in Q4 2019 and COVID-related death rates were calculated from a 12-month period ending in Q1 of 2021. The data for all fatality categories were further stratified by age and reported as rates per 100,000 persons within that age group. The raw data are presented below:
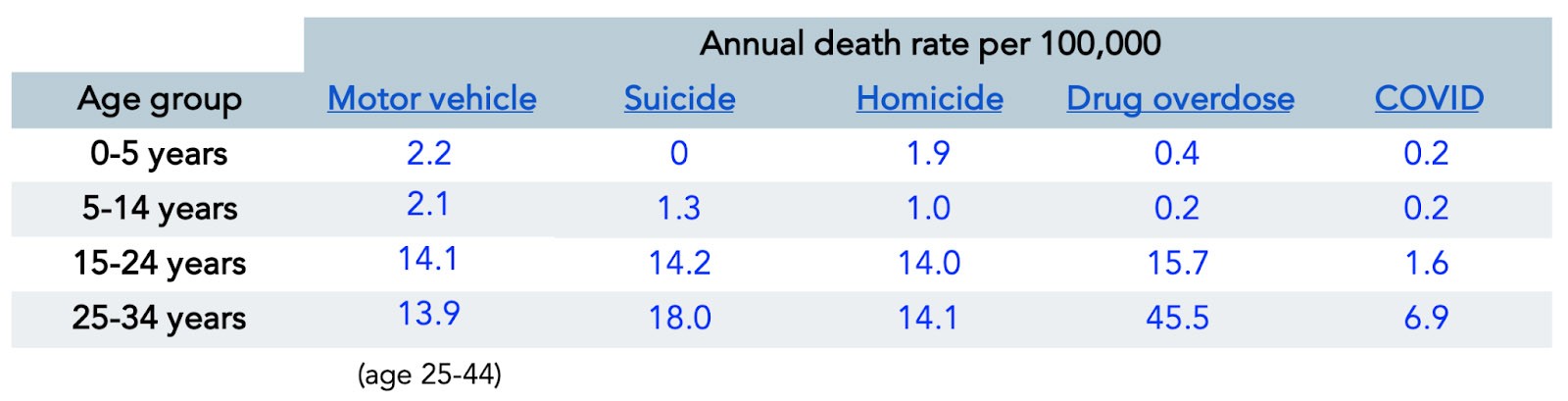
In creating the graph above, I normalized death rates from each category to the death rate from COVID for each age group. (For instance, to compare motor vehicle death rates to COVID death rates in the 0-5 year age group, I divided 2.2 by 0.2 = 11.0, meaning motor vehicle deaths were 11 times greater than COVID deaths per 100,000 children aged 0-5 years over the period of one year.) In other words, all values are presented relative to COVID death rates, which on this graph would all be equal to one. This graph seemed to generate a lot of anger, perhaps because people took it to mean we should not care about COVID. On the contrary, the point was merely that there are many things that pose a far greater threat to the lives and well-being of young people, contagious (e.g., influenza and pneumonia for people under 14, which is 3-5x more common as a cause of death, though not shown here) or otherwise.
OBSERVATION 5
I also generated some harsh criticism for commenting on social media and in last week’s newsletter that I felt it was wrong to remove a patient from the organ transplant list because they had not been vaccinated. In the case of one person, he had already been infected with COVID. In the case of the other, prior infection status was not provided.
Despite allegations to the contrary, I do have a sense of organ allocation, having spent many months on the transplant surgery service during my residency years at Johns Hopkins. If one argues that not being vaccinated implies poor compliance with subsequent medical care, then yes, this would rightly constitute grounds for deprioritization. If one argues that not being vaccinated increases the risk of organ rejection or subsequent infection that could lead to organ rejection (or death), then yes, this would rightly constitute grounds for deprioritization.
I think this is a far more difficult question to contemplate than, say, the utility of mandates, which seems very clear to me. Reasonable people can disagree on this thorny issue. I asked one of my closest friends from residency, Dr. Chris Sonnenday (also a previous guest on the podcast) who is the Surgical Director of Liver Transplantation for Michigan Medicine the following questions:
Is a person who has not had a hep B vaccine ineligible for a kidney?
Is a person who does not get the flu vaccine ineligible for liver or heart?
If this is a longstanding requirement, is it because it speaks to “non-compliance” or is it because the risk of death in the recipient is now too high to justify the organ?
Chris, being one of the most gracious people I know, wrote me a very long response and then hopped on a call with me for about 30 minutes to discuss further. All of this on a Saturday night when he was wrapping up a liver transplant.
I appreciate the opportunity to comment on this issue – I realize it is challenging and nuanced, and I appreciate your willingness to consider it.
I attached a response, which is essentially my description of our rationale for our vaccine requirement, and some of my own thoughts.
Ultimately, as you alluded to, this is about stewardship of a precious resource that demands a zero tolerance for preventable graft loss and patient death.
I will stipulate that the rationale included in my discussion relates to the specific context of immunosuppressed solid organ transplant recipients. The implications of natural immunity and vaccine requirements applied to healthy people are completely different, as I have heard you discuss recently on the podcast.
I have had a lot of long and emotional discussions about this issue with our patients. As you know, there is a lot of distrust of messaging about the vaccine, and appropriate concern about the accuracy of some of that messaging. I have developed great empathy for our patients that struggle with this decision. I am humbled to say though that the overwhelming majority of our vaccine-hesitant patients choose to become vaccinated when we explain to them our rationale and our commitment to their best possible post-transplant outcome. I am aware of only a few (single digits) of the more than 1000 patients on our collective waitlists at UM that have decided to delist or consult with other centers.
Chris’s attached response, which he literally wrote to me while sitting in the OR between cases, can be seen here. If you read this response, you can probably tell why I refer to Chris as, perhaps, the greatest doctor I’ve ever met.
After reading his letter, and speaking with Chris over the phone, I can honestly say I see his point of view with more clarity now. While there are inconsistencies in the requirements for vaccination to be a transplant recipient (e.g., it is not required to receive an annual flu vaccine), vaccine requirements (e.g., Hepatitis B vaccination) have been in place long before the arrival of COVID. More importantly, I now see how the best outcome for a transplant patient–someone who will spend the rest of their life immunocompromised–is likely better if they are vaccinated than if they are not. To that end, I will reverse my position on this particular mandate and I can only hope that everyone on an organ waiting list has the luxury of speaking with someone like Chris, if they are vaccine hesitant.
The Wrap-Up
One unexpected but pleasant surprise of this past week was the great dinner conversations with my 13-year-old daughter, who is learning about critical thinking in school. I was able to use the unfounded criticisms (those that didn’t bother to argue any of the points I made) as a teaching opportunity to demonstrate how not to think critically or rely on logic. As she finds herself at an important stage in life, when she is learning the value of skills such as critical thought and technical writing, I think it can be just as helpful to demonstrate what not to do as it can be to demonstrate what to do.
I was utterly amazed at some of the childish, immature comments and slurs hurled by other MDs, of all people. I really wonder what this says about my profession. Maybe I’m too naive and hold people to too high a standard, but I would have imagined that people with so much education would also have the neuronal reserve to simply focus on the substance of what they disagree with. Regardless, they have all provided an excellent example of everything I don’t want my kids to grow up to be.
Lastly, I want to return to that which I said first, namely, that my goal was to invite everyone to think. My brother Paul reminded me of an important lesson that he learned from one of his best friends and mentors in life. Paul, a former prosecutor and (by his own admission) a professional question-asker, was speaking to this friend about a need for greater question-asking and cross-examination of government policies and asked, “Do you think we, as a society, are afraid to ask tough questions and critically think?” His friend replied, “Maybe. Or maybe we are afraid, so it’s tough to think. Be patient.” His wise friend makes a great point. And to that end, I close this piece where I began my first piece. My simple invitation to everyone is that I’d like us all to think our way through these issues and to do so honestly, accurately, and fairly. If we can do that, our results as a society are bound to improve, even when we all don’t agree.
Thanks for braving the air raid again!
I appreciate the rational and thoughtful discussion on points and particularly the willingness to change your position (vacine requirement for transplant list)
Normally I never comment, (and avoid social media), however I felt compelled to offer my appreciation for you providing balanced discussion during this very polarized times.
Thanks!
KiwiChris has summed up my feelings as well, thank you both.
KiwiChris has summed up my thoughts and appreciation of this post and approach as well, thank you both.
I’m another member of the “alt-middle” as you guys described yourselves, and I appreciate you continuing to draw criticism for the facts and opinions you share. Thank you. Your platform reaches a lot of people and I like being able to direct friends and family to your podcast for education.
With all due respect to your profession, I think what the internet has laid bare when other MDs insult or disparage you demonstrates a dynamic that many (most?) people are well versed in – the arrogant, condescending, even contemptuous doctor. You, and many other doctors, keep your minds hearts open and available to their patients. AND there’re a lot of doctors who calcify in their beliefs and take mental shortcuts to reach conclusions that feel “right.” The “MD” embroidered on the jacket means they know the answer and other opinions or interpretations are just plain wrong and there’s not enough time to actually explain why, so any and all means to shut down the conversation are justified.
Here’s my most recent anecdata I’ll use to support my argument –
My 10 yr old son broke his radius last fall while playing soccer. Two days later at the ortho appointment my wife asked the doctor whether a cast was the only way to treat since a removable brace would be easier to keep clean. My wife is an emotionally intelligent person and would have asked such a question in a suitably deferential manner, but the doctor’s response was disproportionate. The ortho doctor took the question as a personal attack on her ability and training rather than as an opportunity to educate. This is bedside arrogance is not identical to ad hominems hurled through the twittersphere, but I think both take root in similar mental soil.
This may be the best thing I’ve read on Covid. Our collective national neurosis and inability to have a rational discussion about anything has grown so tiresome. I’m a type 1 diabetic with an A1C of 6.1. While I could stand to lose 25 pounds, I’m in overall good health. I’m not afraid of Covid, I’m mindful of it. I mostly follow public health guidance like wearing a mask inside when required. I’m vaxxed, and I’m boosted. I’ve been going to the gym at least 4 days a week since they reopened. Some would call that risky. I would ask what’s the risk of not going? Living my life aware, but not afraid, has worked out for me so far. That’s not the same thing as being “done,” I know. But I am done with the never ending neurosis. I will take some basic precautions as necessary, and will follow the advice of my MD when it comes to possible future vaccination decisions for Covid.
Well for all the hate that’s spread around I very much appreciate the nuanced view presented here.
But talking about majoring in minors: shouldn’t we take opportunity cost into account as well? All this time spent on majoring in the minors of COVID vaccines could have been allocated to other topics which are more likely to impact longevity. So before we have to add another reason to that flowchart of why someone could be mad about Peter’s COVID content (because it’s excessive), maybe it’s time to get back to first order principles.
Dr. Attia, thank you so much for your thoughtful newsletters on COVID. This has been and is an extremely divisive issue, that really shouldn’t be. I’ve given up trying to explain my position to friends and family members that are proponents of vaccine mandates.
I agree that the public health systems have lost any semblance of trust due to really bad messaging and misplaced priorities. I know quite a few vaccine hesitant people, they are not the knuckle draggers characterized by the media, they simply don’t trust the government or corporate media. I don’t see this correcting anytime soon and the mandates are not helping in the least.
Thanks again for your thoughtful and detailed discussion!
I am a chemist, teacher, business owner, as well as a curious person.
I loved both podcasts.
I have share with many people; some who will listen and some who will not, but all you can do is try
Thank you, Peter, for addressing the logical arguments related to your stance, but also for addressing the more significant issue of the emotional responses. It’s so clear how these irrational responses merely lead to strife, and not improved individual or collective health. Also, thank you for noting how “health” does not supersede all other priorities in life with your comparative examples of car accidents, for example.
Finally, I would like to reiterate one glaring lack in your rationales. You provided a checklist of four points for how each vaccine-disease pairing must be evaluated separately. You left off any question about the harm the vaccines cause. Iatrogenic injuries, as you well know, are all too common. As physicians, we must absolutely remain humble with our solutions and never forget that medical interventions must weigh both beneficence AND non-maleficence.
Thank you again for what is (sadly) genuine bravery in your willingness to speak out and stand for rationality with a respect for humanity.
This was quite a remarkable presentation on this topic. I would like to give our leaders and decision makers the benefit of the doubt but my impression is, that there is a general laziness of thought and curiosity about so many things . These individuals have so much data at their fingertips and can literally compel the scientific community to give it to them …. Why don’t they even seem to approach and present to us something close yo what you have presented …
On an other note … I think it’s time for your daughter to interview once again … the questions and concerns of her generation are not getting the attention and demand for critical thinking that is needed .
Good morning Peter,
I am a Hospice volunteer and a Death Midwife who has been deeply interested in science all my life. I am also surprised that so many people look at your truly scientific facts and rail that they are incorrect. A line of thinking has developed in this country that we have never had before. The line of thinking that if you think other than “this way” you are wrong, you are stupid and you should not have the same rights as “they” do.
Many of us, especially, those of us who truly love our country and understand its Constitution, are aghast, dismayed and actually, in my case, worried about what could happen.
In the beginning, we were shown people dropping in the streets of China and heard about the fear and death in Northern Italy. I think at that point, if there had been a vaccine, probably 99% of us would have taken it. However, as time went on and more information came out about alternative treatments, information that some doctors agreed with and who tried to calm the fears by talking about the actual numbers of deaths FROM COVID and not hearing the true numbers of actual deaths of those WITH COVID and FROM COVID, some of us became skeptics. The total shutdown and actual demonizing any conversation of alternative treatments, was so unusual in our lives that many hackles were raised. Defiance began to set in. The conversation stopped being a conversation and began being a loss of choice.
If those alternatives had not been seen as working in many instances, I think there would not have been such a strident resistance. I remember the resistance when the alternatives were being discussed, and it was a political discussion from very early on, Science lost out to politics. Many, who were opposed to the vaccines in the beginning, took on the stance that they should now be mandated. The confusion of the science of masking gave many the idea that there was no “truth” to the science we were hearing. At this point, why should we believe the vaccines work? And many of us felt as if our right of discussion and choice was gone.
I am 72 and took the vaccine including the booster. My 92 year old mother did as well. My youngest daughter, an Natural Nutritionist and healer did not, nor did her family. The got the original COVID, were ill for a while, but are fine now. My mother got Omnicron and was ready to go out on her daily rounds in a week, I have not had it yet, I have not been masking and if I want to do something or go somewhere, I do it.
I am sad. With more and more facts and, what I consider, science coming out, and eventually when more conversation can be had on all aspects, without fear of being shutdown, I think we will find, the resistance to the vaccines will not be as large or vocal. I believe, it is resistance to the restrictions more than the vaccines.
We have been taught to believe we have the freedom to choose, and I believe the when that freedom is not shut down, there will be less resistance to any vaccines. And so, I am for the vaccines, but not the mandates. I am for open conversations and choice and I see, that in some minds, “Science” has become a religion of politics and my stomach churns.
I appreciate your reasonable and rational take on this issue. It terrifies me that the constant drumbeat of fear and death via our government and the mainstream media have created an environment where anyone would call for a vaccine mandate for a virus with a .27% (Ioannidis) overall IFR. As you can see by the responses you’ve received, the vaxx at all costs crowd are still alive and well and immune to your logic.
Thanks Peter, for all your effort and willingness to clarify, correct and change your mind. Your children will benefit most from witnessing your good behavior.
I still cringe that you think going out in public unmasked is a good idea. Here’s my take on that issue, for what it is worth.
I found your site in March 2020 when I became ill with Covid. My cousin the MD called to give this advice: “Assume you have Covid and self-quarantine. Once you recover, assume it was NOT Covid and behave accordingly. If you have any difficulty breathing, call immediately and we will get you to a hospital, but if not, the last place you should be is near a hospital right now.”
My recovery was unremarkable. But a month later, I began my wild ride on the Covid Coaster, suffering from the “echo” one of your early experts mentioned. A Facebook group was formed which has been a lifeline. When new symptoms start, I can check that group to see if this is being manifested in others. And their leaders performed the first survey that discovered we could be parsed into 4 groups, in a statistically robust method that is the core of most of the research now underway on Long Covid.
This pandemic is so much easier to go through with people like yourself being willing to forego profit for the public good. Thank you.
Today, I am triple vaccinated, and like you, am against vaccine mandates unless the individual works in healthcare, where they are dangerous to compromised individuals. And I would not hire an anti-vaxxer in a sensitive position because they have demonstrated the inability to examine and parse coverage in the media with facts.
As for masks, I wear them always. Myself, I have one 4 layer mask I prefer for several reasons. But when the mandate for FFP2 masks came in the community I was in, I bought FFP2 masks. They are a problem because they ride up into my eye socket, and I can’t get a good fit after trying 4 different brands. But I’m unwilling to appear in public wearing a mask that others will assume is less sufficient than the FFP2 (Europe’s version of N95) because it adds to the distress of the compromised and implies I do not support efforts to calm this pandemic to its natural demise. Now, I wear my favorite mask under a FFP2, which is pulled down away from my eye. It works well enough, I can breath, and my eye is able to recover from recent surgery. Intelligent people should take some responsibility to find what works for them, but supports the community. Only the stubborn insist on having everything their way. I tried at least 12 different masks when I was first shopping in 2020. Most people don’t need so many, but I’m sceptical of anyone who tells me they can’t wear a mask because they can’t breath in them, they hurt, or they cause higher humidity and that is an incubator for Covid.
Sometimes we need to do things that might not be our preference, for the public good. Masks are merely a signal that you want this to end as quickly as possible.
I very much appreciate your clear, detailed and balanced approach to difficult and fraught issues. Your humor is refreshing, especially in the face of nasty and personal attacks. Please keep up the good work.
By the way, I was unable to download the Chris Sonnenday pdf. It just hung. A server issue, perhaps?
Very well done Peter Attia. I am grateful for your studied precision around a difficult subject. Many people do not have the ability to study and understand the statistics and information (often false) around this topic. Science has become “ the Science.” Unfortunately this means for many of us making decisions based on confusion, fear, and coercion.
These are extraordinary divisive times. Lack of ability to safely discuss opinions have become the lightening rod for which families, friendships careers, and communities are in ruins.
. I myself am fearful of the serious and perhaps long lasting affects of this division. Thank you for your reason and clarity.
Warmest regards.
Sandra
Thank you for these two great newsletters! Can we sign Neil Young up for the newsletter as well?
Love this. Thank you for modeling how a logical and thoughtful argument can change a person’s viewpoint. (Your friend Chris’s patients and colleagues are lucky to have him. I, too, appreciate his insight.) I am the director of a small school I founded a few years ago. Your reflection with your daughter and thoughts on thinking are invaluable for young people to consider. Thank you.
Peter,
I’m mostly with you, but not all the way yet because of one last point that I think you may still want to consider addressing (apologies if I missed it).
Omicron appears to be infecting at a faster rate than previous variants. Even though usually mild, the number of folks in the icu is still overwhelming the health care system due to the rate of infection. In Canada, this has resulted in more beds taken from other areas for Covid patients, more staff taken from other areas for Covid patients, etc. Our understanding is that the vast majority of the Covid patients are un-vaccinated. Even if the outcomes are not as fatal as the old strains, vaccinated folks are impacted by surgeries cancelled, etc.
I fully realize that mandates to slow this down would be a mandate, and not root cause fix to address icu shortages or staff shortages in Canada, but don’t mandates still help slow down the tsunami?
Will finish reading after noting that “not taking care of lipids” does not “cause” CVD. There is a very long list of “things” associated with CVD, as you well know, and LDL molecules are not among them. (cf: “The Clot Thickens”, Malcolm Kendrick, M.D.)
Thank you, Dr. Attia. The courage it took you to speak up and take an honest and fair look at all this will be my measure of trust in any doctor I work with in the future. I am more suprised than I would like to be that you have had to point these facts out to folks, especially doctors who are supposed to be among the greatest thinkers. Maybe, just maybe, some of us put two and two together long ago at the risk of being called every name in the book. At best, this issue is worthy of debate – nowhere near as clear as the entities make it sound. Signed, a geologist with integrity from Nebraska.
Thanks for this. I’ve long believed that the best decisions made/conclusions reached are based on a combination of perspectives. I always try to make the fairest, most carefully considered assessment I can based on the information available to me at the time, but am always keen to hear/respect the constructive views of others & adjust my thinking in the light of new/better information as I feel appropriate. Getting the best outcome with organ transplantation is clearly a more complex issue than I’d originally thought. The change I’d make to my original opinion would be in terms of optimising clinical outcome by minimising/avoiding factors which potentially limit this, whilst balancing doing so against clinical need. I’m not sure a ‘perfect’ decision is possible. If it was, what would we have to strive for? However, by rationalising expectation, we can hopefully realise that we can only make ‘best choices’. We’ll never be able to ‘play God’ but being as astute a ‘sub-contractor’ as possible should be/is a surely a worthy goal!
Thank you for clear, thoughtful, and digestible content for the lay person like myself. Indeed, if more of us would be patient and think the world would be a better place.