
Check out more of my recent content on COVID:
- (January 3, 2022) COVID Part 1: Current state of affairs, Omicron, and a search for the end game
- (January 23, 2022) Why I’m for COVID vaccines, but against vaccine mandates.
- (January 24, 2022) COVID Part 2: Masks, long COVID, boosters, mandates, treatments, and more
- (January 29, 2022) A follow-up to my article on vaccine mandates
Tomorrow we’ll be releasing a follow-up discussion with Drs. Marty Makary, Zubin Damania, and Monica Gandhi on all things COVID. This episode was put together in response to the overwhelming, if not staggering, response to our first episode, released on January 3 (Monica was not on that one, but she is a brilliant addition to part 2). In this episode we aim to address most of the topics that so many of you have asked us to expand upon.
On the heels of this podcast, I want to write about something that we discussed on the podcast, something that is sure to upset some reading this or listening to the episode, whichever side you find yourself on: Vaccine mandates.
The goal of this article is not to irritate you for the sake of irritating you. My hope in writing this, first and foremost, is to invite you to think. In the heated debate over vaccine mandates, science and logic have often been lost amid politics and fear. Ever-evolving circumstances – such as the emergence of variants with radically different levels of infectiousness or virulence – have only further separated opinion from facts. (After all, if facts are changing, why haven’t opinions changed, too?)
Of course, I’d like to convince you of my point of view (denying this would simply be disingenuous—why else do we write or argue a point?). But if that fails, I hope, at least, that this newsletter may serve as a reminder that exchanging rational decision-making for fear and blind partisanship is a recipe for injustice, discrimination, and policies that may do more harm than good. Scientific policy must be based on scientific truth — otherwise it will be ineffective in the present — and damage credibility for the future.
Let’s start with my priors: COVID vaccines save lives.
COVID vaccines absolutely save lives. Full stop. My opposition to vaccine mandates does not in any way diminish my belief in the data supporting the efficacy of vaccines in preventing severe disease and death, particularly in people over 65 and in those with comorbidities. So, I’m not going to spend much time extolling the virtues of vaccines beyond sharing some data that should always be examined for any medical intervention: what is the benefit, in different risk groups, in both relative and absolute terms?
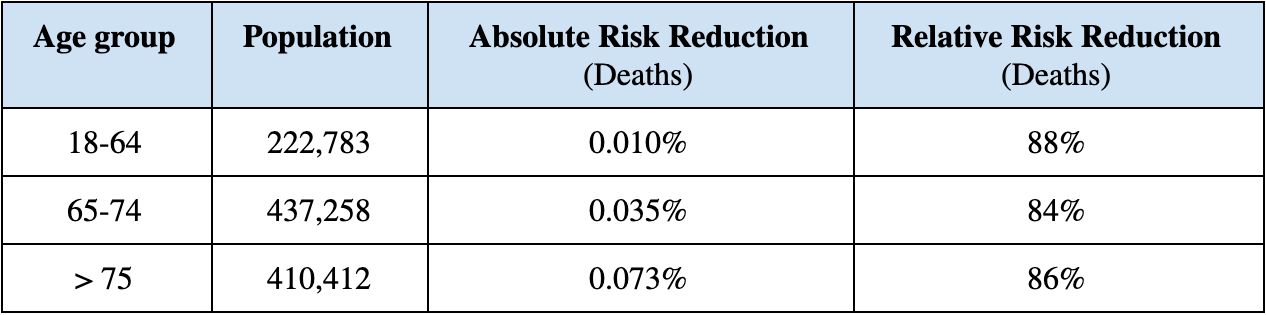 Deaths of Unvaccinated vs Vaccinated (mRNA vaccines only, at least 1 dose). Data collected from the Veterans Affairs system between December 2020 and March 2021.
Deaths of Unvaccinated vs Vaccinated (mRNA vaccines only, at least 1 dose). Data collected from the Veterans Affairs system between December 2020 and March 2021.
The data above show that for people over the age of 18, the relative risk reduction (RRR) of death is between 84 and 88%, regardless of age. This is very close to the 90% risk reduction that was touted at the time of vaccine approval a year ago. But if you’ve paid attention to anything I’ve spoken and written about for the past 10 years, you will recall that we should always pay attention to absolute risk reduction (ARR) also. If the relative risk reduction is 90% (to make the math easy), you still don’t know if the risk is being reduced from 100% to 10% or from 0.1% to 0.01%. And this matters greatly.
Consider the following example: Let’s say we faced a virus that killed 100% of those who contracted it. A vaccine with a 50% RRR (i.e., only “50% effective”), meaning it reduced deaths by half, would save over 150 million lives in the U.S. But if we faced another virus that killed 0.1% of those who caught it, even a vaccine with 99% RRR (i.e., “99% effective”) would “only” save about 300,000 lives (by lowering the death rate from 0.1% to 0.001%). In other words, in this scenario the vaccine that is 50% is far more valuable—and saves orders of magnitude more lives—than the one that is 99% effective that reduces deaths from 0.1% to 0.001%. How is it possible that a vaccine that is only 50% effective could save more than 150 million lives, while one that is 99% effective can only save 300,000 lives? Because of absolute risk reduction. The 50% effective vaccine is up against a virus that infects and kills every single person in a given population, so in absolute terms it is wildly effective, literally saving one out of every two lives of the people who take it. Conversely, the vaccine that is 99% effective is up against a virus that only kills 1 out 1,000 people who encounter it.
Returning to the actual data for COVID vaccines, take a look at the absolute risk reduction column. Here, two things stand out. First, the absolute risk reduction (ARR) increases with age. Why? Because the older you are, the more likely you are to die from COVID, so the benefit from the vaccine is greater. Second, the ARR numbers are very small, especially for people younger than 65. A quick way to get an intuitive understanding of this is to take the reciprocal of the ARR. This number is known as the “NNT” or number-needed-to-treat, which tells you how many people you need to treat to save a life. If the ARR is 50%, the NNT is 2 (1/0.5). If the ARR is 0.1%, the NNT is 1,000 (1/0.001). Based on this data set from the VA (which I chose because of the age stratification), the the number of people you need to vaccinate to save one life in the 18-64 group is 10,000, versus 2,857 in the 65-74 group , and 1,370 in the over-75 group. By comparison, the NNT for a statin is between 50 and 200, depending on the study and patient population studied.
This is not to imply that COVID vaccines are ineffective or somehow useless. Far from it. A quick glance at the recent CDC data, covering more than 1.2 million people who completed their primary vaccination between December 2020 and October 2021, bears this out. In this broader group, 0.015% had a severe case of COVID and 0.0033% died. Not surprisingly, the risk of death was highest among people over 65 and among those who were immunocompromised or had significant comorbidities. But overall, the risk of death among people who were vaccinated was infinitesimal.
In fact, the rate of death from COVID if you are vaccinated is on par with, and likely less than, that from influenza. According to CDC data from 2017 to 2018, there were approximately 41 million symptomatic cases of influenza that year. This resulted in over 710,000 hospitalizations and nearly 52,000 deaths, which means a fatality rate of 0.126%. Looking at the same data for 2018 to 2019, we can see the death rate was 0.095%. It is abundantly clear: If you are vaccinated, your risk of severe illness or death from COVID is very low, even compared to influenza.
So, why not mandate vaccines, then?
There are many reasons I have heard put forth for why vaccines should be mandated, but one dominant argument stands out: Mandating vaccines will protect vaccinated people from unvaccinated people. This argument assumes three things:
- Vaccines DO NOT provide complete protection to the vaccinated (or else why would we care about what the unvaccinated do),
- Prior infection DOES NOT confer immunity on par with vaccination, and
- Vaccines DO prevent transmission of the virus (which is why we want the unvaccinated vaccinated, even if we don’t care about their health, per se).
Well, we’ve largely addressed the first point in an effort to get our facts straight on vaccine efficacy, and as we’ve seen, the basic assumption fueling this concern is valid at its surface: vaccines do not provide complete protection to the vaccinated. That is, they are not 100% effective at preventing infection, hospitalization, and death. In fact, although vaccines significantly reduce risk of detectable infection in the few months after vaccination, this protection drops precipitously once circulating antibodies decline, though protection against severe infections and death persists. Still, the protection isn’t absolute, and some risk of death remains even among those who have been vaccinated. However, the good news is that the risk is very low today. This was not necessarily the case 18 months ago, but three things have evolved over the past year-and-a-half to compound the risk-reduction of vaccines:
- Novel therapeutics have been developed specifically to treat COVID, including monoclonal antibodies, paxlovid, and molnupiravir, all of which reduce the risk of hospitalization and death by anywhere from 50% to 90%.
- At least one existing drug (fluvoxamine) has been repurposed to treat COVID successfully, reducing both hospitalizations and deaths by 66% and 91%, respectively, based on per protocol usage.
- Far more sophisticated critical care knowledge has evolved, specifically, to address COVID, including the use of dexamethasone and better strategies of ventilation.
The net result of these advances, layered on the benefits of vaccination, imply that a vaccinated person infected with COVID today is in a far less risky position than they were a year ago. And this says nothing of the fact that when it comes to the Omicron variant, which today accounts for >99% of document cases in the U.S., the risk goes down much further. Why? Because the data are unambiguously clear that Omicron is much less virulent than Delta and Beta and Alpha.
How much less virulent is Omicron?
Well, if we look at the most up-to-date information at the time of this writing (still in pre-print), analyzing data from Kaiser Permanente in Southern California between November 30, 2021 and January 1, 2022, there were a little over 52,000 documented cases of Omicron in the patients in their medical system, compared with nearly 17,000 cases of Delta (today these numbers skew much more to Omicron, of course, based on the current distribution of Omicron in the U.S.).
- 235 (0.5%) of these Omicron patients required admission to the hospital, compared to 222 (1.3%) of the Delta cases;
- of the 235 Omicron cases, zero required mechanical ventilation, compared to 11 patients with Delta;
- one patient with Omicron died, compared to 12 patients with Delta; and
- 84% of patients hospitalized with Omicron left the hospital in less than 2 days, compared to 31% of patients hospitalized with Delta.
Of course, none of this should be surprising given what we know from the data out of South Africa, where Omicron originated, which demonstrated the reduced severity of Omicron relative to Delta, even in a country with very low vaccination rates. Omicron is a very mild infection, compared to Delta, Beta, or Alpha, and based on the emerging data I’ve presented above, it seems to be mild even compared to influenza.
Therefore, we can conclude that while the vaccinated are not immune to COVID infections, their risk of severe illness or death is very low because of the following:
- The vaccines greatly reduce hospitalization and death, and
- We have a slew of novel and repurposed drugs that are very effective at treating COVID, and
- Our hospitals and ICUs are far better equipped to treat COVID patients based on nearly two years of empirical and trial data, and
- The dominant variant, Omicron, is a very mild virus (even to the unvaccinated).
How does natural immunity stack up to vaccines?
Next, let’s examine the assumption that prior infections do not provide immunity on par with vaccine immunity. Of the three sub-arguments in the case for mandates based on protecting the vaccinated, I find this the hardest to understand. I am not aware of any other virus from which a recovery does not confer immunity (and yet a vaccine does). In other words, the null hypothesis around this point, at the outset, should be that natural immunity is indeed as good as vaccine immunity, pending data to prove that assumption false. Looking back at the close coronavirus cousins of COVID, SARS and MERS, the data are overwhelming that patients who survived those infections had lasting immunity, even 12 years after infection. Do data exist to suggest natural immunity doesn’t exist for this particular coronavirus? No. To the contrary, there is ample evidence that natural immunity is robust and durable. In fact, the data suggest that recovery from COVID provides longer lasting and stronger protection against subsequent infection, symptomatic disease, and hospitalization caused by the Delta variant, compared to vaccination.
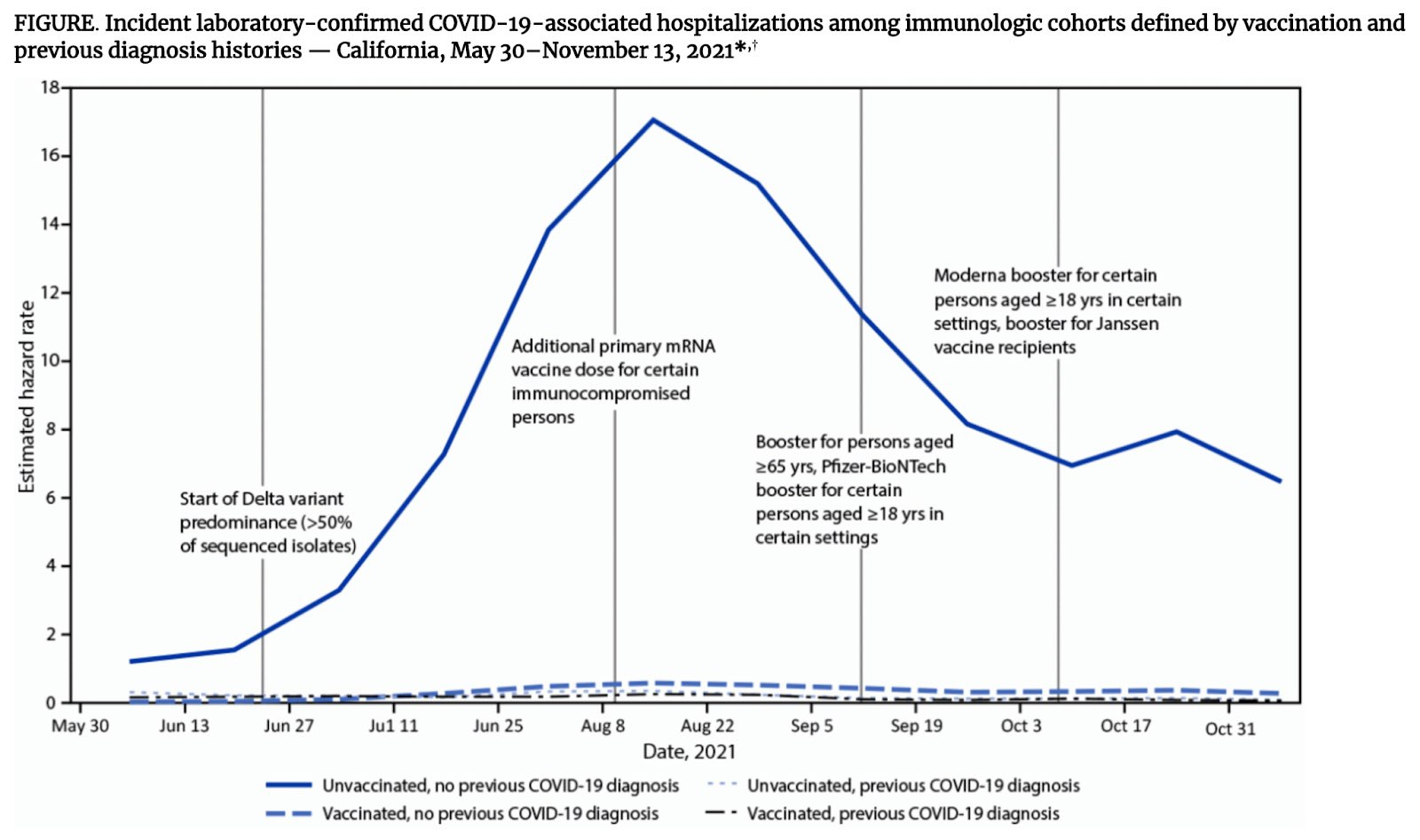
A quick examination of this figure from the CDC data released on January 20 shows that there is virtually no difference in hospitalizations from COVID between the vaccinated and unvaccinated, if a prior COVID infection took place.
In fact, if you look at Table 1 from the paper, and run the calculations yourself, you’ll see the risk of hospitalization is lowest in the group that was not vaccinated, but previously infected. I’ve summarized the data here for the fraction of each group that required hospitalization following a COVID infection:
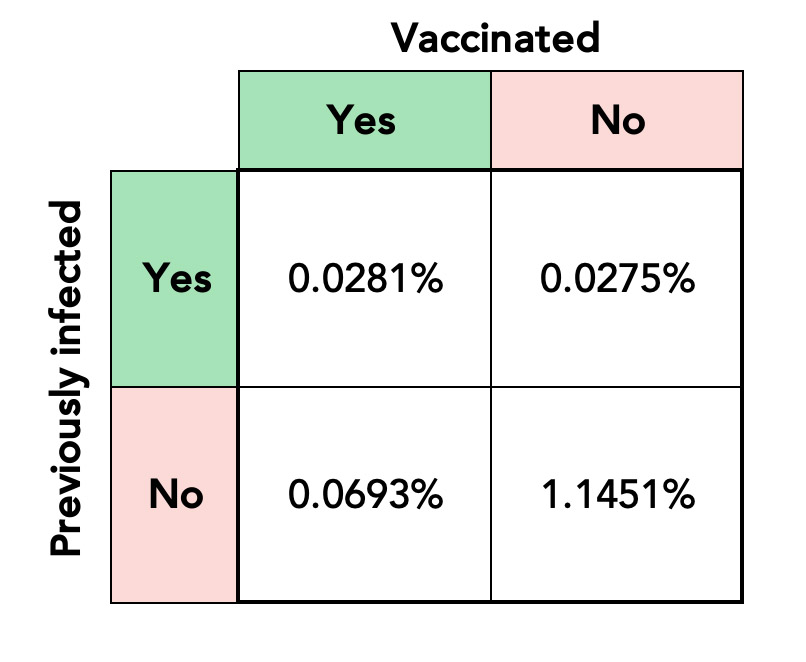
This simple table, based on data from nearly 22 million COVID positive cases in California between May and November 2021, makes three points so abundantly clear, it’s hard for me understand how there can be any vestigial ambiguity:
- Vaccines unquestionably reduce the risk of hospitalization in previously uninfected people (by a factor of 16.5x), and
- In people who are previously infected vaccines offer zero additional benefit with respect to hospitalization, and
- In vaccinated people, being previously infected reduces the risk of hospitalization by a factor or 2.5x.
Can the case be any clearer, simultaneously, for both the efficacy of vaccines and natural immunity?
How do vaccines affect virus transmission?
Finally, let’s consider the rationale for mandating vaccines to prevent the unvaccinated from transmitting the virus to the vaccinated. A perfect vaccine would not only completely abrogate the severity of the virus on the host, but it would also completely prevent the host from transmitting it to another person, vaccinated or not. This is clearly not the case for any of the current COVID vaccines. In fact, it seems that they only slightly reduce the risk of transmission, and that vaccinated and unvaccinated persons with detectable infection have the same viral loads, despite the reduction in disease severity for the former group. Using a metric called the secondary attack rate (SAR), it’s possible to look at infection rates in household contacts stratified by contact vaccination status and index case vaccination status, and based on such analysis, it seems that vaccination only slightly prevents transmission. Vaccination does not reduce the peak viral load in the infected (though it does appear to reduce the duration of viral shedding, which may translate to the reduction in SAR). An important caveat here is that such analyses have been carried out prior to Omicron’s arrival, but considering everything we know about the mild nature of Omicron, the risk of transmission to vaccinated people is, again, likely much less.
What about mandating vaccines to prevent hospitals from being overrun with COVID cases?
It’s true that hospitals are stretched very thin right now with the n-th surge of COVID. But a few things are worth keeping in mind. During a bad flu season in the U.S. (recent examples would be 2017-2018, 2014-2015, and 2012-2013) it is common for 50,000 to 70,000 patients to be hospitalized at any one time across the country. This is not very different from what we see today (which says nothing of the fact that roughly half of the hospitalized COVID patients have incidental infections. That is, they are there for another reason, but also test positive for COVID). The difference, today, is that the hospital workforce is greatly reduced, relative to a bad flu season. Why is that? According to a survey by Morning Consult, approximately 18% of healthcare workers have quit their jobs since February 2020, while another 12% have been fired or laid off.
Furthermore, many people fail to realize that hospitals routinely function at 90% capacity in their ICUs. A reduction in workforce of even 10% is horribly disruptive to a system flying so close to the sun. It’s kind of like what happens when one of the OPEC nations, even if “only” producing 3% of the world’s oil, goes offline. Complete and total breakdown of the world’s energy markets ensues. It’s called a marginal supply problem.
Perhaps there was a rationale to mandate vaccines in healthcare workers 12 months ago, but given how many of them have quit or been fired for not being vaccinated, despite the fact that they undoubtedly have the highest rates of natural immunity of any profession, it seems illogical to continue to keep unvaccinated healthcare workers away because their immunity came from the actual virus, and not a vaccine.
So where does this leave us?
- We have a virus that is far less lethal than the one that started the pandemic two years ago.
- We have very effective vaccines that reduce the severity of illness and death by about 90%.
- We have ample treatments to further reduce severity of illness in death (in vaccinated and unvaccinated alike) by another 90% or so.
- We have better methods of providing in-hospital care to the infected.
- For all their benefits, vaccines are not very effective at preventing transmission.
None of this is opinion. These are simply the facts upon us.
Politics and healthcare will always interconnect to some extent. So, the right question to ask at this time is not why are they’re intertwined, but rather: to what extent should they be?
As some of you heard me outline in my recent interview on Joe Rogan (#1735) and again during my podcast with Drs. Makary and Damania on January 3rd, there is an important distinction to be drawn between Science and Advocacy. Clear lines should be drawn between those two concepts. Vaccine mandates are a prime example of how those lines are often blurred.
Science is not a noun. It is not a person, or group of persons. It is a process. And it’s a process by which you perpetually adapt and evolve through the rigor of always testing your best guesses and seeking to disprove your own assumptions and firmly held beliefs. You welcome uncertainty in the interest of getting just one inch closer to the truth. Speaking in absolutes is not the aim.
Politics, one could argue, is radically different. Political leaders are criticized for speaking with uncertainty and punished for changing their minds. In that sense, politics is the antithesis of the scientific process.
None of the above is a new phenomenon, and little about this dichotomy is likely to change. However, the crux in which we now find ourselves is the present impact of this divide, manifested strongly in our current political policy and juxtaposed with our current scientific knowledge.
Another question that we don’t seem to be asking ourselves is, what, exactly, is the definition of unvaccinated? It’s becoming more and more subjective each day. Today, unvaccinated apparently applies to an 18-year-old college student who “only” received the full 2-shot vaccine dose, but did not receive a third booster shot. Such a student can’t attend a college for which their tuition has been paid. If they concede to the third dose, when will they require a fourth? A fifth? If we’re using circulating antibodies as our metric of immune success, we’ll need to give boosters every 3 months to keep antibodies high. And for what? Certainly not to help us avoid severe disease, hospitalization, or death. For that we can rely on the memory B-cells and T-cells we developed in response to an actual infection or to our first vaccination.
What is the impact of vaccine mandates?
Let’s consider the following examples of the impact vaccine mandates are having right now:
-
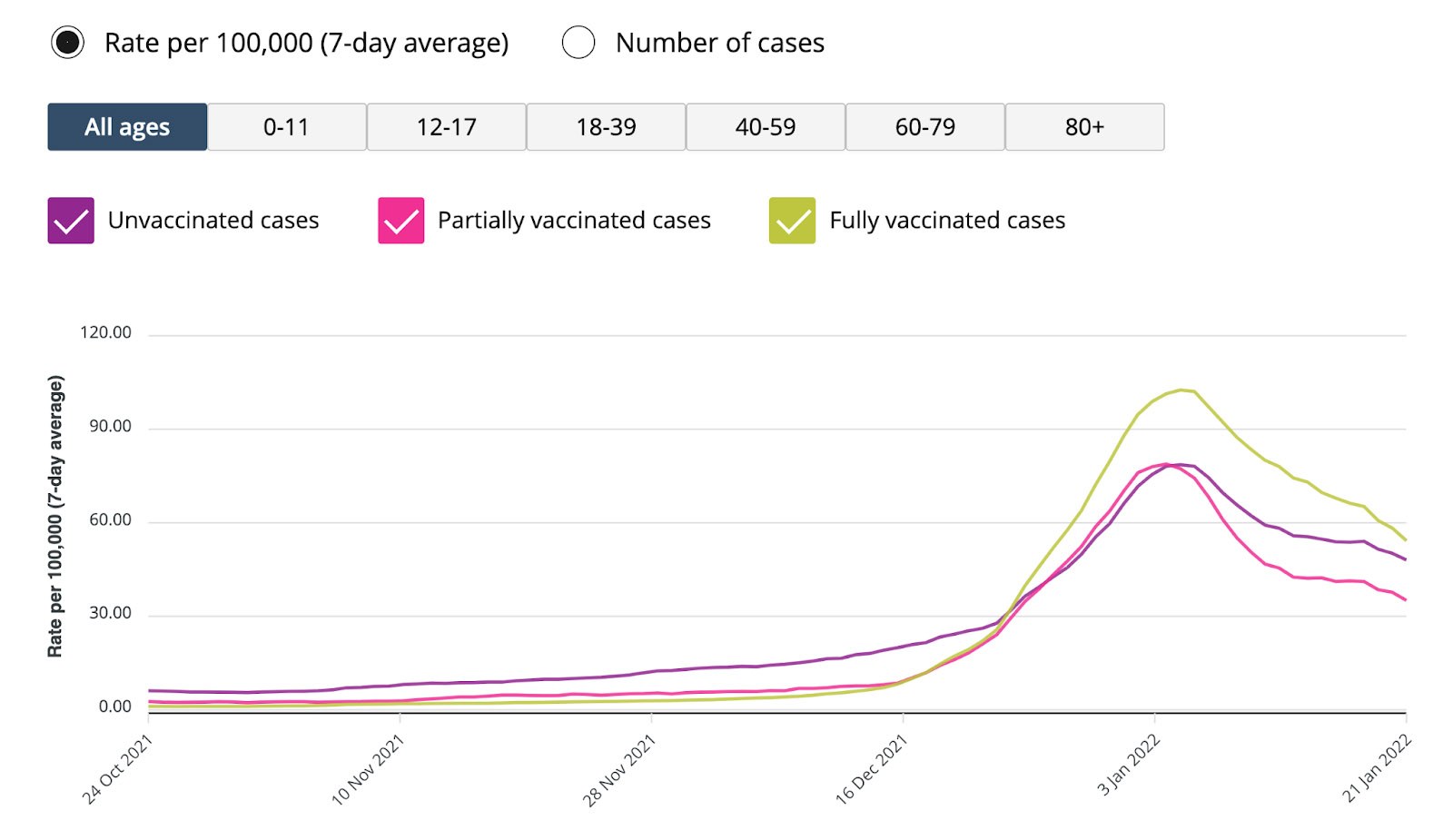
- In my birthplace of Canada, an unvaccinated person cannot board a plane or a train, let alone go into a restaurant, gym, or skating rink. This is especially interesting, given that the rate of infections in Ontario is now higher in vaccinated than unvaccinated persons, a transition that occurred with the arrival of Omicron in late December. This finding presumably speaks to the low efficacy of the current vaccines at preventing Omicron infections.
- A Canadian friend of mine, this week, was prohibited from seeing a medical doctor for a corneal abrasion because the doctor refused to see unvaccinated patients (including those with natural immunity from a prior COVID infection). Bear in mind that this is occurring in Canada, a country with universal access to healthcare—a hallmark of Canadian values.
- A Virginia man in need of a kidney transplant was removed from the transplant list, denying him a life-saving procedure, because he was not vaccinated (though he was previously infected with COVID).
- In September, Canada’s Prime Minister, Justin Trudeau said that the unvaccinated are part of an extreme group that also included misogynists and racists.
- Here in the U.S. some are even calling for the deployment of the National Guard “to ensure that people without proof of vaccination would not be allowed, well, anywhere.”
- A previous guest on my podcast, who asked to remain anonymous, was recently fired from their job as a professor at a very prestigious university for not being vaccinated. This person was fired with cause, which meant they were not even able to apply for unemployment insurance.
The bottom line.
I have been clear about my support for vaccinations. They are an excellent tool to protect us against severe infection and death from COVID. What they are not, however, is a monolithic tool to be used as a sword against our citizens, rather than a shield against a virus. When we call the unvaccinated misogynists and racists as Mr. Trudeau has, or when we make it our goal as a society to make the lives of the unvaccinated as miserable as possible, as French President Emmanuel Macron has said, what are we hoping to achieve? Is this a strategy to increase vaccination rates, or to exact a vengeance?
Even though the U.S. Supreme Court last week struck down the federal government’s proposed vaccine mandate for large corporations, hundreds of U.S. companies and universities are still putting in place mandates of their own, which come with stiff financial penalties and even job losses.
As you consider this thorny issue, I urge to consider the following questions:
Even if you felt vaccine mandates made sense one year ago, when the Beta and Delta variants were raging, when it was too soon to say how well the vaccines would work in the real world, when we had few excellent treatments for infected, and when ICUs were still struggling to understand how to treat COVID, can we really say with a straight face we’re in the same difficult situation, today, especially with the Omicron variant?
What is the scientific evidence to support vaccine mandates today? Today, we have vaccines that are very effective at preventing severe disease in the vaccinated. Today, we have many treatments to further reduce the severity of illness, if infected. Today, we have enormous expertise to treat infected patients in hospitals. Today, we have a dominant variant in Omicron that is nowhere near as virulent as its predecessors. If this were really about science, why would we not allow previous infection, which confers all the benefits of vaccination, if not more, the same rights? Does it not seem that mandates are having the opposite effect to what is desired? Instead of increasing vaccination rates are mandates instead hardening and alienating the unvaccinated further?
If we are being honest with ourselves, are the mandates truly for the protection of the vaccinated, or do they exist to punish the unvaccinated?
How will history evaluate these mandates?
How will history evaluate us for how we have treated the unvaccinated?
And as we look at future science-based policy discussions, even beyond COVID, we need first to agree on the questions we are actually trying to answer. From there, we can begin to explore different possible solutions and debate their costs and benefits in a rational and civil manner. And always, we need to ask ourselves honestly: are we picking sides based on assertions and talking points (Advocacy) or testable hypotheses (Science)?
injecting injection vaccine vaccination medicine flu man doctor insulin health drug influenza concept - stock image

Great article. Next up: Why I’m for COVID vaccines, but against lockdowns”
Clear and concise. Thank you so much!!
I agree with all your comments, for me, if we allow people to risk illness and hospitalization, fine, the problem is is that there is no room in hospitals to keep this up! As a doctor, you understand the stress of endless hours, no break. As a nurse it is mentally and physically exhausting. We are loosing medical professionals left and right. How can you argue this?
What about bogging down hospitals with the stupid people? That impacts us all.
I think you are saying we should be vaccinated but not mandated to be vaccinated.
What about mandates for school entry for all the other vaccines who’s diseases have been almost wiped out.
Hi Peter,
I was eagerly awaiting your section on hospitalization. I’ve always understood the most important aspect of a vaccine mandate to be reducing hospitalization and the burden on the health care system. You showed the 2×2 table, which showed the vaccination decreased hospitalization by 16.5x for those previously uninfected. Because of our health care system’s marginal supply problem, this reduction in a population that has still has a large portion uninfected is a big deal. A vaccine mandate is the most efficient way to reduce hospitalization. It’s an unnecessary burden to ask organizations, etc. to test the vaccine refusers for prior infection. Mandating the vaccine is efficient but imperfect public health policy.
I tested positive for Covid in early January. I am 66 and had what I would compare it to a very bad case of the flu. I specifically asked about paxlovid at an urgent care center in Fort Myers, FL. The doctor told me there is nothing they can prescribe for Covid, but did give me a 3 day prescription for prednisilone. My point of this comment is that unfortunately the novel therapeutics were not yet available to me, and apparently are not widely distributed yet.
One of, if not the BEST article I have read in the past year on this topic. Thank you for your logical, always science based approach. I also appreciate that you are willing to speak out on this topic in the face of unprecedented censorship, black listing, and the increased potential for attempts to be made to discredit you because you have an opinion that doesn’t fit the “ mainstream narrative “. Please continue to do what you are doing.
Great points all across. I am curious regarding the comorbidities and increased death rate. For those that have co morbidities (lifestyle induced or not, but for the sake of argument let’s say they were born with them) this argument feels like we don’t value the lives of those with comorbidities by not requiring vaccines. How do you think we should think about the small percent of folks that their best chance of survival is to never be exposed?
Great article. As always, very balanced and logical. The only point with which I take issue is that Omicron “originated” in S.A. If by that word you mean “first detected and named”, then no issue at all.
Peter, this is cutting edge thinking, and I for one, appreciate your slicing through the noise, and being willing to update us as scientific findings change. What’s missing for me here is long COVID. My brother-in-law, a (previously healthy athletic 55 year old) dentist, had COVID in March 2020, and he is still quite sick. At this point, it’s uncertain if he’ll ever be able to work again. This actually terrifies me more than death. If you get COVID after vaccination, do you get long COVID? What about if you get it a second time after you have natural immunity? Does the omicron variant lead to long COVID? Do kids get long COVID? There are so many unanswered questions here, and I don’t expect you to know the answers. But for a lot of us—those of us who are not elderly and don’t have co-morbidities— the fear of long COVID is real, even if the possibility of death is vanishingly small. Thank you for all the good work you do.
Great read. Thanks, Peter. One question regarding the data sample in the first chart: “Deaths of Unvaccinated vs Vaccinated (mRNA vaccines only, at least 1 dose). Data collected from the Veterans Affairs system between December 2020 and March 2021.”
Is Dec 2020 – March 2021 a sufficient sample? Why not more and why not data that includes the Omicron variant?
Good article, pointing to the demonstrated benefits of vaccine in view of the newer viral strain and better therapeutics.It is time to abandon political postures and have a little critical thinking.
However, an important point is missing, at the core of each decision, medical or not lays the benefit/ risk balance. The known and even more important, the unknown future adverse reactions from vaccines are to be balanced against the diminishing benefits. In young healthy people, the risk of severe disease is virtually none, so exposing them to adverse reactions for nothing is very close to a non ethical decision.
Thank you for the fact based approach. Should the following be considered as part of the viewpoint?
Does vaccination reduce the likelihood of future variants? Variants could impact the vaccinated. Apologies if I missed this.
You seem to treat the unvaccinated-previously-exposed as a known, static population. Isn’t it really a trial and error population? You don’t know how the unvaccinated will respond to infection until they are infected and recover. Once infected – and confirmed – the argument could be made for vaccination-like status. However waiting for that to play out can be a long road with unecessary strain on medical services. The strain could take services away from the vaccinated.
Thank you. Excellent, reasoned and much appreciated. I don’t have as much time to dive into the evidence as I’d like so to have it more clearly spelled out is welcomed. A day in the clinic does not go by without patients asking me questions about the current state of things related to the virus. Your analysis will aid me in providing thoughtful dialogue when asked.
What is your take on vaccinating children at age five? I live in Marin County, California and they are really pushing all parents to vaccinate their children as soon as they turn five years old.
I do not see any reason to do this.
Thanks for everything you do Peter!
Your analysis certainly makes sense. However, the data comparing deaths of vaxxed vs unvaxxed is likely skewed by causation, ie dying because of covid vs dying with covid. Secondly, it assumes that people beat covid because of the vaxx versus having been fortunate enough to escape medical protocol of intubation/ventilator. In other words, if medical protocols had allowed life-saving treatments such as ivermectin and hydroxychloroquine, would the death be lower?
Aside from the questionable death rate of Covid, you haven’t considered the risk of an adverse event from the vaxx and booster. When one makes the decision, one must necessarily do a cost/benefit analysis. The cost would be the risk associated with the vaxx vs the relative benefit. Especially for those who are at low risk of covid.
Hi Dr Peter Attia,
Thank you for this article. I’m afraid I’m from Canada so maybe things are a little different here, but I’ve always understood the vaccine mandates are to protect the ‘unvaccinated’ (especially those who cannot get vaccinated), plus it’s a form of ‘stick’ to people who could get vaccinated but are unwilling, as hospital systems were under threat of being overwhelmed and, in many cases, are being overwhelmed. Here for sure. Maybe in your country too? I’ve never heard of a vaccine mandate to ‘protect the vaccinated from the vaccinated’ so when I saw this in your article it almost struck me as a straw-person argument and I had to make myself continue reading through to your more detailed points about the vaccine and natural immunity both being very protective. Is it true that mandates are sold (in your country) as protecting the vaccinated from the unvaccinated?
That should read ‘I’ve never heard of a vaccine mandate to protect the vaccinated from the unvaccinated.’
You are lucky then Desiree, but I think if the vaccine mandate is to protect the “unvaccinated”, to be in line with the science it wouldn’t make sense to mandate those previously infected, and for age groups to whom the vaccine would have no measurable benefit (children <18 with no co-morbidities), basically any demographics for whom there is no evidenced benefit from the vaccine.
At least in the U.S. the narrative is very much so "to protect the vaccinated/at-risk" population, which as this article points out quite well, is not backed by the data we currently have.
Thank you Peter for speaking the truth!
Great summary and thank you. In our office (I am an Orthopedic Surgeon) we went the rout of education and open discussion rather then mandate and have achieve 100% vaccination for those who have not had covid-19 and we did not recommend vaccine for those had been infected and we have not loved a single employee.
How can you have a conversation about effectiveness of the vaccines and the issue is of mandates without also including a conversation about safety, both short-term (debatable – as in there are many people debating it) and long-term (for which there is still no data)?
Surely the possibility that the vaccines are increasing all-cause mortality, or that in 5 year’s time we’ll see a sudden increase in kidney/liver disease/cancer (or whatever else) is a serious question to be addressed in the context of new MRNA vaccines and vaccine mandates.
You bring such a great level headedness to these issues, it would be a shame for you not to address this part of the discussion.
Hey Adam, many of those points were brought up in the recent podcast (referenced in those article).
This medium has limitations and not every single pertinent point can be addressed in a timely manner in a single article.