
Mohit Khera is a world-renowned urologist with expertise in sexual medicine and testosterone therapy. In this episode, Mohit provides a comprehensive overview of male sexual health. He begins with an in-depth exploration of erectile dysfunction, shedding light on its prevalence across different age groups, diagnostic methods, and its intriguing connection to cardiovascular disease. He then ventures into Peyronie’s disease, penile fractures, penile enlargement treatments, prolonged erections, premature ejaculation, and anorgasmia. Shifting gears, Mohit delves into the intricate workings of testosterone, DHT, and estrogen, emphasizing their physiological significance and interplay. He explains blood tests for diagnosing low testosterone, the correlation between symptoms and blood levels in cases of low testosterone, and the pros and cons of different methodologies for increasing testosterone. He concludes with a thought-provoking conversation about the role of testosterone in patients with prostate cancer and addresses concerns surrounding DHT, finasteride, and post-finasteride syndrome.
Subscribe on: APPLE PODCASTS | RSS | GOOGLE | OVERCAST | STITCHER
We discuss:
- Mohit’s career path and interest in sexual medicine and infertility [3:00];
- The anatomy of the male genitalia [5:45];
- The prevalence of sexual dysfunction, its impact on quality of life, and the importance of seeking help [7:15];
- Erectile dysfunction (ED): definition, diagnosis, pathophysiology, and more [11:00];
- The history of medications to treat ED and the mechanisms of how they work [15:30];
- Relationship between aging and erectile dysfunction and Mohit’s approach to treating patients and prescribing medications [20:00];
- The impact of lifestyle on sexual health and the association between ED and cardiovascular disease [29:30];
- Causes and treatments for Peyronie’s Disease, penile fracture, and more [37:30];
- The value of ultrasound for ED diagnosis and management strategies [47:45];
- Various treatment options for ED: injections, penile prosthesis, and more [50:15];
- Priapism (prolonged erection): what is happening and when to seek treatment [57:15];
- Shockwave therapy as a treatment for ED [1:02:45];
- Stem cell therapy for ED [1:08:15];
- Platelet-rich plasma (PRP) injections as a treatment for ED [1:12:00];
- Premature ejaculation (PE): prevalence, pathophysiology, and treatment [1:14:45];
- Anorgasmia: causes and treatment [1:22:00];
- The interplay of sex hormones, the impact of aging, symptoms of low testosterone, and considerations for testosterone replacement therapy (TRT) [1:26:45];
- Methods for increasing endogenous testosterone [1:38:45];
- Testosterone replacement therapy: various forms of exogenous testosterone, weighing risk vs. reward, and more [1:52:30];
- The physiology and purpose of testosterone and DHT, why some men feel fine even with “low” testosterone, personalized approaches to treating low testosterone, and more [2:02:30];
- Post-finasteride syndrome [2:09:00];
- The role of testosterone in prostate cancer and addressing the notion that TRT could increase risk [2:16:15];
- The effects of testosterone as an adjunct to therapy for estrogen-sensitive breast cancer in women [2:27:15];
- Resources for those looking for healthcare providers [2:28:45]; and
- More.
Mohit’s career path and interest in sexual medicine and infertility [3:00]
Can you tell us about your background and what you did after medical school as it relates to your current work?
- Mohit went to Vanderbilt for college, after which he attended Boston University where he got his Master’s of Business Administration (M.B.A.) and Public Health (M.P.H.)
- After working as a healthcare analyst for two years and not quite enjoying it, he decided to change the course of his career path
- Mohit then went to the University of Texas, San Antonio for medical school, after which he did a one-year internship in general surgery at Baylor College of Medicine and spent five years in urology
- He then did a one-year fellowship in male reproductive medicine surgery, where he developed a keen interest in sexual health and infertility
- Mohit has been a faculty member at Baylor since 2007
What are the different aspects of urology, and could you share some insights on what the fellowship experience in urology is like, particularly related to reproductive and sexual health?
- Peter notes that from his experience, urology places a significant emphasis on urologic cancers such as prostate cancer, bladder cancer, and kidney cancer
- However, since his exposure to urology was limited, he wasn’t able to see much of the other aspects of the field, particularly those related to reproductive and sexual health
- Mohit explaines that urology is a diverse field with multiple subspecialties and areas of expertise in urology include stones, cancer, and female urology, among others
- However, sexual medicine and infertility are important subspecialties in urology as well
- Reproductive medicine involves procedures such as vasectomy reversals, varicocele repair, and sperm retrieval
- Sexual medicine focuses on addressing issues such as erectile dysfunction, premature ejaculation, Peyronie’s disease, and hypogonadism
- Mohit has dedicated his career and research efforts to sexual medicine
The anatomy of the male genitalia [5:45]
Can you briefly go over the anatomy relevant to the male sexual health?
- The penis is not a single organ, but rather a combination of three distinct organ systems: the urinary system, reproductive system, and sexual system
- The urinary system includes the bladder and urethra
- The reproductive system includes the prostate
- The ejaculatory ducts within the prostate receive sperm from the testicles and mix with seminal fluid from the seminal vesicles to form ejaculate
- The corpora cavernosa are smooth muscle bodies responsible for erections and are located above the urethra
- The urethra is responsible for urinary function
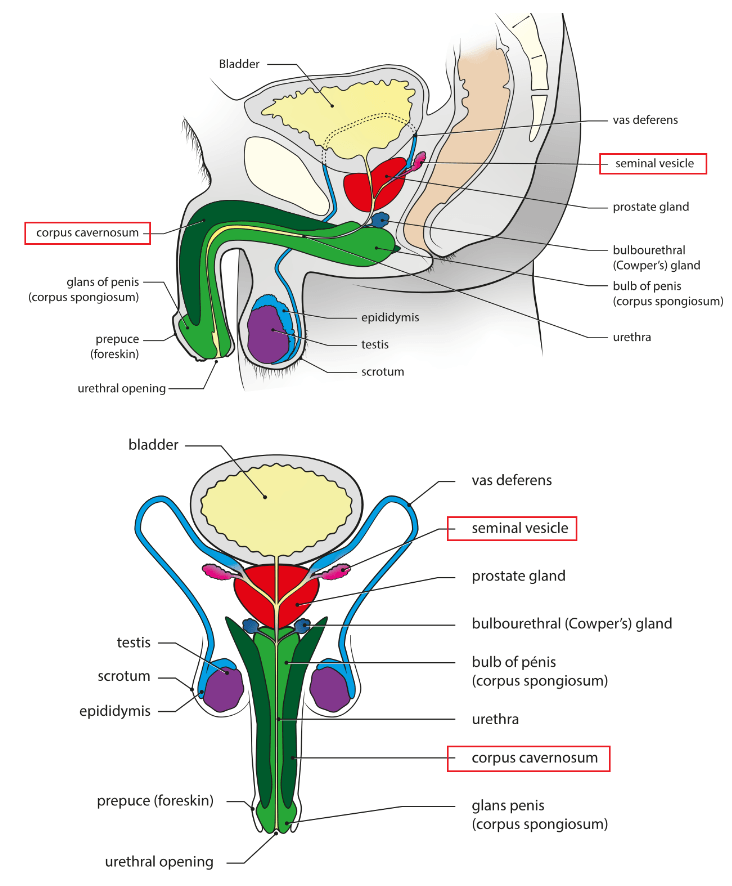
Figure 1. Anatomy of the male reproductive system, sagittal and frontal view. Image credit: Wikipedia
- This system is holistic, and each component has the potential to affect the others
- For instance, infertility and hypogonadism can impact each other
- Patients taking medication for benign prostatic hyperplasia (BPH) may experience retrograde ejaculation, which can, in turn, negatively impact both fertility and sexual function
{end of show notes preview}

Mohit Khera, M.D., M.B.A., M.P.H.
Mohit Khera received his Bachelor of Science from Vanderbilt University, and went on to earn his Master’s degree from Boston University School of Medicine. Dr. Khera then earned both a M.B.A. and a M.P.H. from Boston University. He then earned his M.D. at the University of Texas Health Science Center. Dr. Kera completed his internship in general surgery, residency in urology, and fellowship in male reproductive medicine and surgery, all at Baylor College of Medicine.
Dr. Khera is a Professor of Urology and the F. Brantley Scott Chair in Urology at Baylor College of Medicine, the Director of the Laboratory for Andrology Research at the McNair Medical Institute and serves as the Medical Director of the Executive Health Program at Baylor. He also serves as the President-Elect of the Sexual Medicine Society of North America.
Dr. Khera has dedicated his clinical and research efforts to three main areas: men’s health, sexual medicine, and hormone replacement therapy. Dr. Khera has conducted extensive research on various topics related to his specialty, including the effectiveness of botulinum toxin type A in treating Peyronie’s disease, genetic and epigenetic studies on post-finasteride syndrome patients, and testosterone replacement therapy. In addition to basic science research, he has initiated numerous clinical trials. His basic science and clinic experiences have allowed him to thus far give over 250 lectures at scientific meetings throughout the world, publish over 120 articles in peer reviewed journals, complete 15 book chapters, and edit and write two books in the field of sexual medicine and men’s health. In 2007 he was awarded the American Urologic Association (AUA) Research Scholars Award to study the correlation between ED and BPH. In 2013 he was elected to serve a 4 year term on the American Urologic Society Examination Committee. Dr. Khera has also served on the AUA Peyronie’s Disease and Erectile Dysfunction Guidelines Panel. For the past several years he has taught numerous courses in testosterone therapy and sexual dysfunction throughout the world. [Dr. Mohit Khera]
Instagram: @drmohitkhera
Twitter: @DrMohitKhera



Would have liked a discussion on long-term safety of vasectomies. Still need to listen, but seems like there’s nothing in the show notes.
interesting podcast as ever, Peter …
re ED as predictor of cardiovascular issues:
if i understood correctly your guest indicated that 39% of men having cardiovascular events were suffering from ED.
he also indicated that prevalence of ED is approx 40% at age 40 rising to 60% at age 60. roughly ED% = age.
given that the typical cardiovascular event occurs at age 60 ish (+/-10 yrs?) to me this suggests the ED is slightly _negatively_ correlated with cardiovascular risks. the ‘control group’ would ahve a 60% ish prevalence of ED.
Agreed?
Or have i missed something ?
thanks!
D
Great episode. On TRT for five years now. 27g insulin syringes are much more comfortable and affordable. Not sure why you guys insist on 25g. With the 27g I can draw 1ml in one minute. Easy to inject also. This may help new patients who fear needles.
Hi Dr. Attia and fellow subscribers,
What a wonderful informative discussion and so helpful to present a number of topics that can help men wade through this disruptive issue.
I am a physical therapist using Piezowave focused shockwave to treat ED. One detail I would like to correct is that GAINSWAVE does not produce any devices, they are likely the number one marketing and education company increasing awareness of shockwave. However, there is wide variance in devices and procedures used by professionals in the GAINSWAVE network. If anyone from the company sees this hope they can provide more detail as well.
Best,
Grant Headley PT, DPT
What is Dr Khera’s preferred compounding pharmacy for testosterone?
Hi Dr. Attia
You says “I have low T” – yet your numbers are double mine, and I’m ten years younger. We’re both reasonably fit and aside from stubborn body fat, I don’t suffer from any low T symptoms as far as I can tell, do you?
It also seems to suggest you realize TRT will be inevitable for you as you mentioned “holding out for as long as possible.”
Do you see ALL/MOST men heading into their later years of life requiring TRT or wanting TRT?
Informative as always. Would have liked to see at least some mention of porn addiction and it’s effects on the brain/erectile dysfunction.