
Before I get into this post I want to lay a few things out.
- This post is written mostly for doctors, but also for patients who really want to understand this topic, if for no other reason than to help them choose the right doctors. I don’t go out of my way to simplify the terminology and I assume the reader is familiar with the topics covered in the cholesterol series I wrote. If you encounter a term you don’t understand, Google is a pretty good place to find the definition.
- I will not use this post to in any way get into prescriptive strategies, which involve modifications of nutrition, hormones, and yes, lots of drugs across four or five classes (i.e., much more than just statins) depending on the specific situation at hand and the risk appetite of the patient and physician, as well as the other comorbidities that must be co-managed. Even if I wanted to write out all of my prescriptive leanings I could not do it briefly.
- Please do not email your lab results or ask me to weigh in on your case. You know the disclaimer: I can’t practice medicine on a blog or over email.
There was a day when the only thing I argued about was who the greatest boxer of all time was. (I’m fighting all urges to turn this post into a manifesto of 1965-67 Muhammad Ali vs. 1938-41 Joe Louis vs. 1940’s Sugar Ray Robinson vs. 1937-42 Henry Armstrong.)
Today, however, I find myself arguing about so many things—some of them actually important—from why symptomatic women should receive hormone replacement therapy after menopause (and, by extension, why the Women’s Health Initiative tells us so, if you know how to read it) to why monotherapy with T4 for hypothyroidism is a recipe for disaster for most patients. But there is nothing I find myself debating more than the misconceptions most doctors have about heart disease. This is especially troubling since heart disease kills more Americans than any other disease. To put this in perspective, a woman in the United States is 7 to 8 times more likely to die from heart disease than she is from breast cancer.
Here are the typical arguments put forth, almost always by doctors, which invariably result in my need/desire to counter:
- Heart disease is caused by too much “bad” cholesterol (LDL-C).
- LDL-C is the only target of therapy you need to worry about.
- Calcium scores and CT angiograms (CTA) are great ways to further risk-stratify (the corollary: when these tests are negative, there is no need to treat the patient).
- Atherosclerosis is a “pipe narrowing” disease (ok, nobody uses these words, but they imply this by saying it’s a luminal narrowing disease).
- There is no role for preventatively treating young people, except in very rare cases like familial hypercholesterolemia.
Briefly, here are my counters:
- Atherosclerosis is caused by an inflammatory response to sterols in artery walls. Sterol delivery is lipoprotein-mediated, and therefore much better predicted by the number of lipoprotein particles (LDL-P) than by the cholesterol they carry (LDL-C) [Bonus point: always measure Lp(a)-P in your patients—but we’ll have to save Lp(a) for another day; it certainly owns its own blog post].
- Ditto point #1. And don’t ever bring up LDL-C again.
- Calcium scores and CT angiograms of exceptional quality (the operative word being exceptional—most are not) are helpful in a few settings, but this assertion is patently false, and I will leave this discussion for another blog post as the topic is too rich in nuance for a few lines.
- We’ll discuss this today.
- By necessity, we’ll be forced to confront this today, also.
Before diving into this topic it’s really important for me to acknowledge the person who has taught me almost everything I know about this disease, beginning back in 2011 when I first became aware that I basically had no idea what atherosclerosis was. For many years Dr. Tom Dayspring’s generosity has been remarkable and I’m humbled to be his most sponge-like student. Tom has not only given me an on-the-side lipidology fellowship, but he has also introduced me to the finest lipidologists and cardiologists in the country who have, in turn, been incredibly generous with their time and knowledge. I’m not the only one to benefit from Tom’s wisdom and generosity. I had dinner with Tom’s son and his wife once and I described Tom to them as a national treasure. That’s really how I feel about him. He is a nationally-recognized educator and his writing and presentations are devoured by fanatics like me across the globe. With Tom’s permission, I’ve deconstructed a video he put together into a series of figures which I’ll use to begin this discussion of how atherosclerosis actually takes place.
The physics of luminal narrowing
Traditionally, the atherosclerotic process was believed to involve plaque accumulation that prompted the gradual narrowing of the lumen, with the eventual development of stenosis. Stenosis then caused impaired control of flow (stable angina) and plaque rupture and thrombosis (unstable angina and MI). Consequently, prevailing opinion held that coronary angiography would be able to gauge the atherosclerotic process at all stages of disease.
However, in 1987, Glagov and colleagues proposed an alternative model of atherosclerosis development. After performing histological analyses of coronary artery sections, Glagov et al. reported that early atherosclerosis was characterized by plaque accumulation in the vessel wall and enlargement of the external elastic membrane (EEM) without a change in lumen size.
As atherosclerosis progressed, they found that plaque continued to accumulate in the vessel wall until the lesion occupied approximately 40% of the area within the EEM. At this point, the lumen area began to narrow. These findings have since been confirmed by intravascular ultrasound (IVUS). Due to the complex remodeling that occurs in the earlier stages of atherosclerosis, coronary angiography, which only visualizes the lumen, tends to underestimate the degree of atherosclerosis. In other words, atherosclerosis is well under way long before angiography is able to identify it.
I was reminded of the words of my Pathology professor back in the first year of medical school, “The only doctors who actually understand atherosclerosis are pathologists.” I would add lipidologists to that list, but I saw his point.
Most people, doctors included, think atherosclerosis is a luminal-narrowing condition—a so-called “pipe narrowing” condition. It’s true that eventually the lumen of a diseased vessel does narrow, but this is sort of like saying the defining feature of a subprime collateralized debt obligation (CDO) is the inevitable default on its underlying assets. By the time that happens, eleven other pathologic things have already happened and you’ve missed the opportunity for the most impactful intervention to prevent the cascade of events from occurring at all.
To reiterate: atherosclerosis development begins with plaque accumulation in the vessel wall, which is accompanied by expansion of the outer vessel wall without a change in the size of the lumen. Only in advanced disease, and after significant plaque accumulation, does the lumen narrow.
Michael Rothberg wrote a fantastic article on the misconception of the “clogged pipe” model of atherosclerosis. He opens with the following story:
A recent advertisement on the back cover of a special health issue of the New York Times Magazine section read “Ironic that a plumber came to us to help him remove a clog.” The ad referred to doctors in the cardiac catheterization laboratory as “one kind of pipe specialist,” and noted that the patient in the ad returned to work “just 2 days after having his own pipes cleaned out.” Although the image of coronary arteries as kitchen pipes clogged with fat is simple, familiar, and evocative, it is also wrong [emphasis mine].
Dr. Rothberg goes on to explain that for patients with stable disease, local interventions can only relieve symptoms; they do not prevent future myocardial infarctions. To be clear, at least 12 randomized trials conducted between 1987 and 2007, involving more than 5,000 patients, have found no reduction in myocardial infarction attributable to angioplasty in any of its forms. And yet, despite this overwhelming evidence, the plumbing model, complete with blockages that can be fixed, continues to be used to explain stable coronary disease to patients, who understandably assume that angioplasty or stents will prevent heart attacks—which they patently do not.
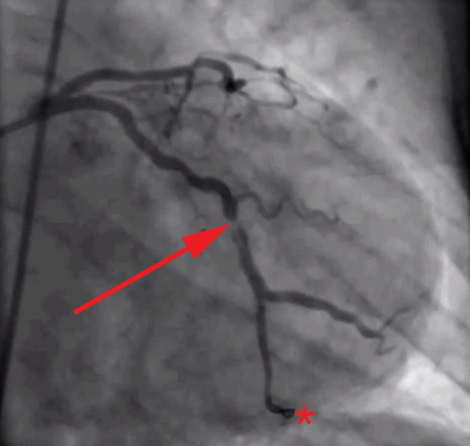
The root of the problem, in my view at least, is that we as doctors—and by extension, our patients and media—spend too much time looking at images like this (angiograms of coronary arteries complete with “clogged pipes”):
And not enough time looking at images like these (the histological, i.e., pathology, sections of coronary arteries):
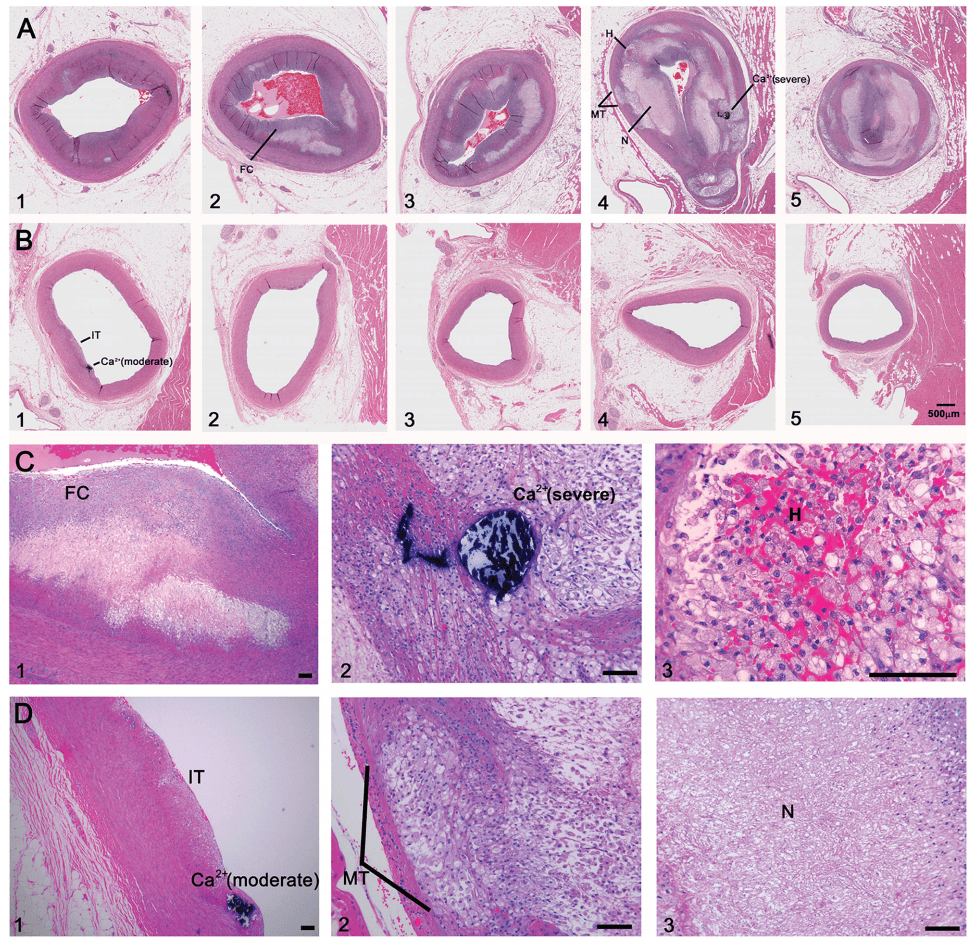
But who can blame us, I mean, angiograms are cool! But, alas, it’s time to get serious about understanding this disease if we want to prevent/delay it.
Atherosclerosis, for the cognoscenti
Ok, so now let’s get rigorous about the pathology that kills more Americans than any other disease. To understand this, as Frederic Bastiat wrote long ago, we must resort to “long and arid dissertations.” Buckle up.
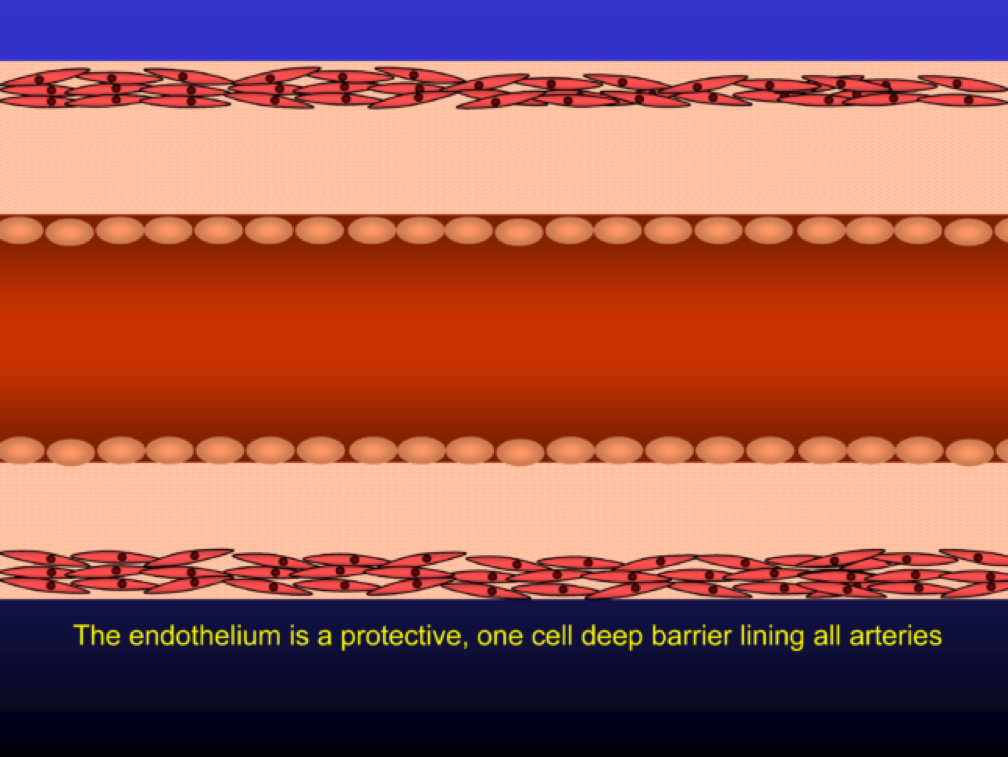
The following figures were constructed from a video Tom Dayspring produced in one of his stellar lectures on the development of atherosclerosis. I’ve broken the video down into 20 or so steps which show the transition from a completely normal endothelium (i.e., at birth) through myocardial infarction. Each figure is preceded by a brief explanation of its content.
The endothelium is a protective one cell layer lining the surface of the artery lumen. Endothelial cells perform many complex functions and are capable of modulating vascular tone, as well as inflammatory and thrombotic processes. Their function depends on many circulating and local factors.
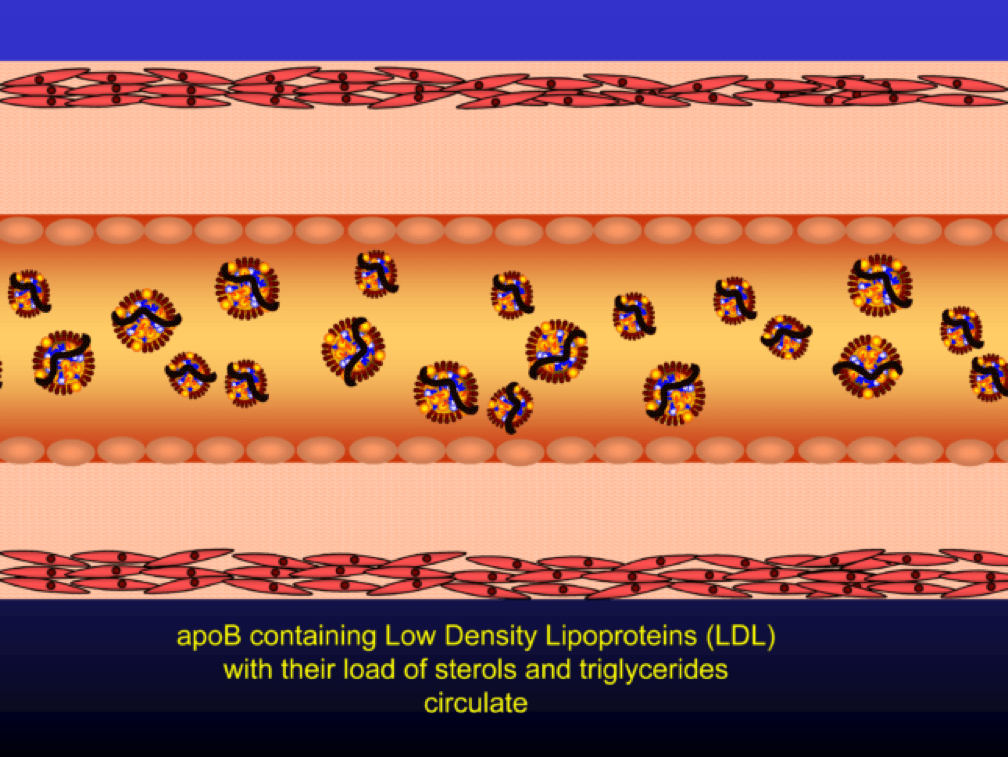
Low density lipoprotein (“LDL”) is a lipid (the bulk of which is cholesterol) transport particle. Please re-read this sentence. It is not “bad cholesterol,” a term that has no meaning. LDL—the particle—allows lipids (cholesterol, but also triglyceride, phospholipid) to be delivered through the aqueous medium of the blood, since lipids are hydrophobic (i.e., repel water) and a “carrier” is needed to transport them in blood (which is mostly water).
If LDL particles are present in physiologic (i.e., normal) concentrations, they effectively deliver cholesterol to those tissues that require it (recall: all tissues make cholesterol but some don’t make enough for their own needs and therefore cholesterol needs to be trafficked around the body).
The term LDL particle, LDL-P, and apoB are used interchangeably (the latter, because LDL particles are defined by the wrapping of a lipoprotein called apolipoprotein B-100).
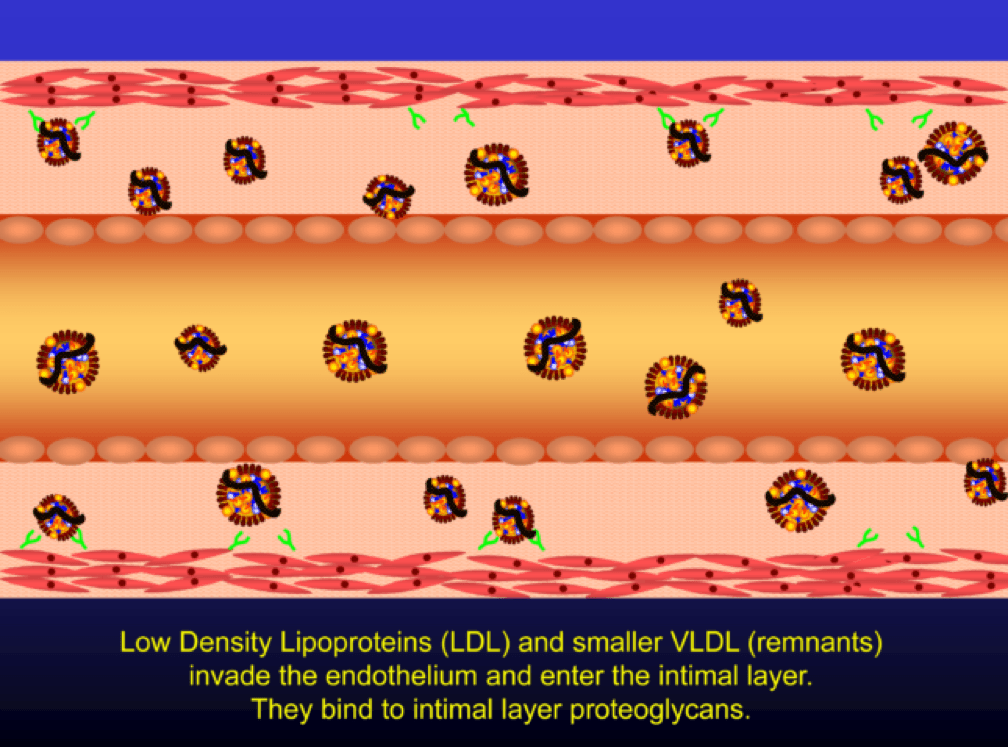
When LDL particle concentration is elevated, the lipoprotein penetrates into the subendothelial space. Once in the intimal layer, they are securely attached to intimal proteoglycan molecules. The first step in atherogenesis is surface phospholipid (PL) exposure to reactive oxygen species and oxidation of the PL. LDL particles that are not oxidized are not atherogenic. To be clear, it’s not the “getting in there” part that is the problem (HDL particles do this all the time and so do LDL particles, for that matter), it’s the “getting stuck and oxidized in there” part, formally known as retention and oxidation.
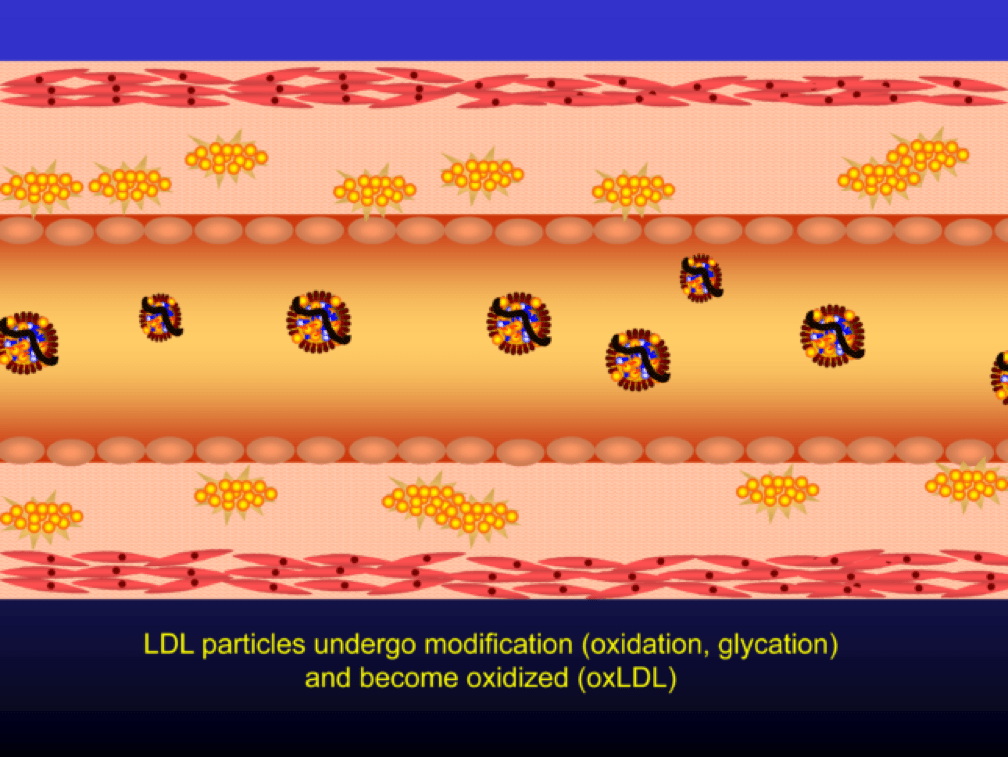
Once retained in the subendothelial space, the LDL particle may be modified, or oxidized (the clusters of yellow circles in the subendothelial space, below).
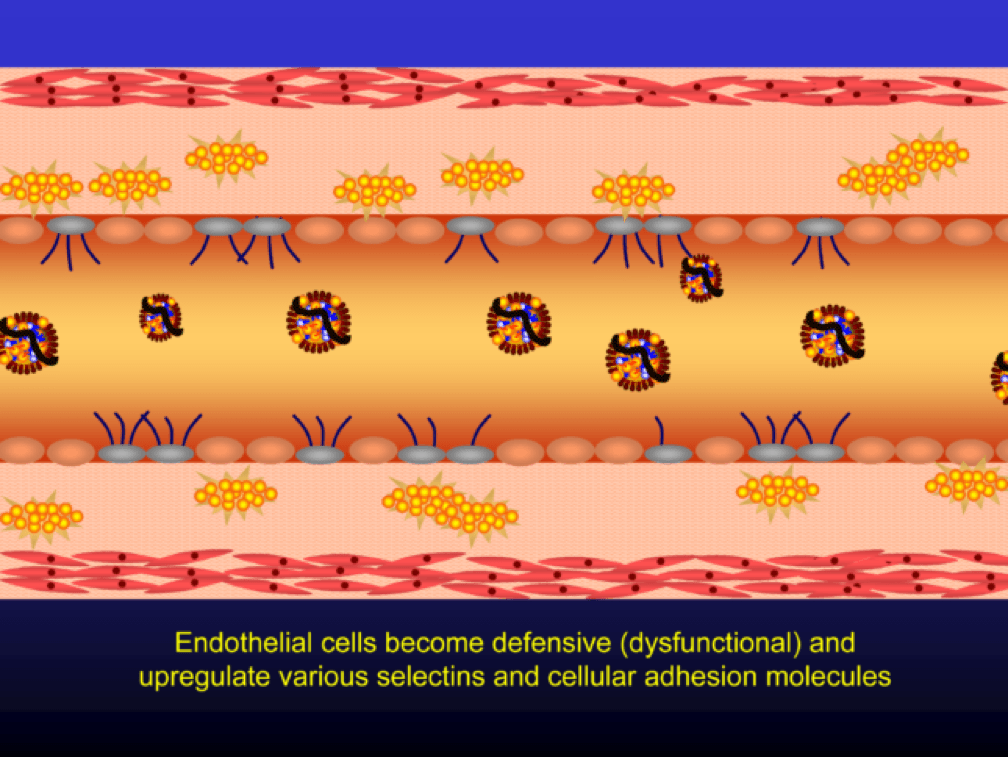
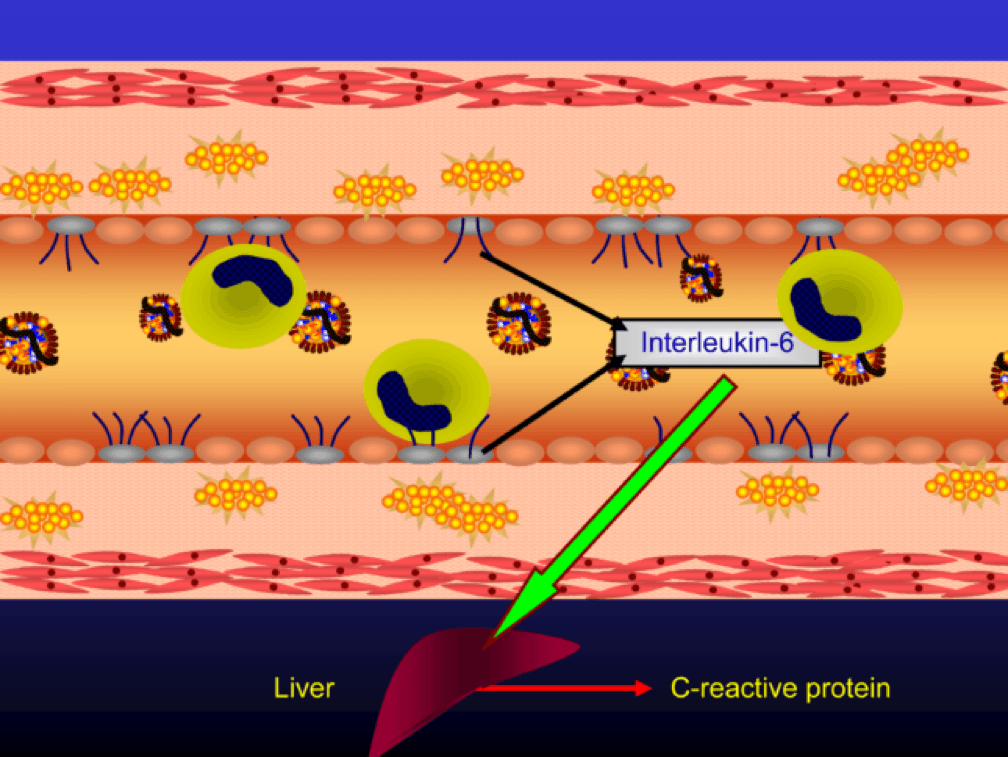
Oxidized LDL particles are toxic to the endothelium. Now-dysfunctional endothelial cells express selectins and vascular cell adhesion molecules (VCAMS) which mark the injured areas of the vascular wall. It is worth pausing here for a moment. This step is kind of the turning point in the story. It’s also a perfectly “normal” thing for the epithelium to do. They sense a problem and like any law-abiding tissue, they ask for help from law enforcement. Think of the selectins and VCAMS as 911-calls. The police, who show up shortly, are the monocytes.
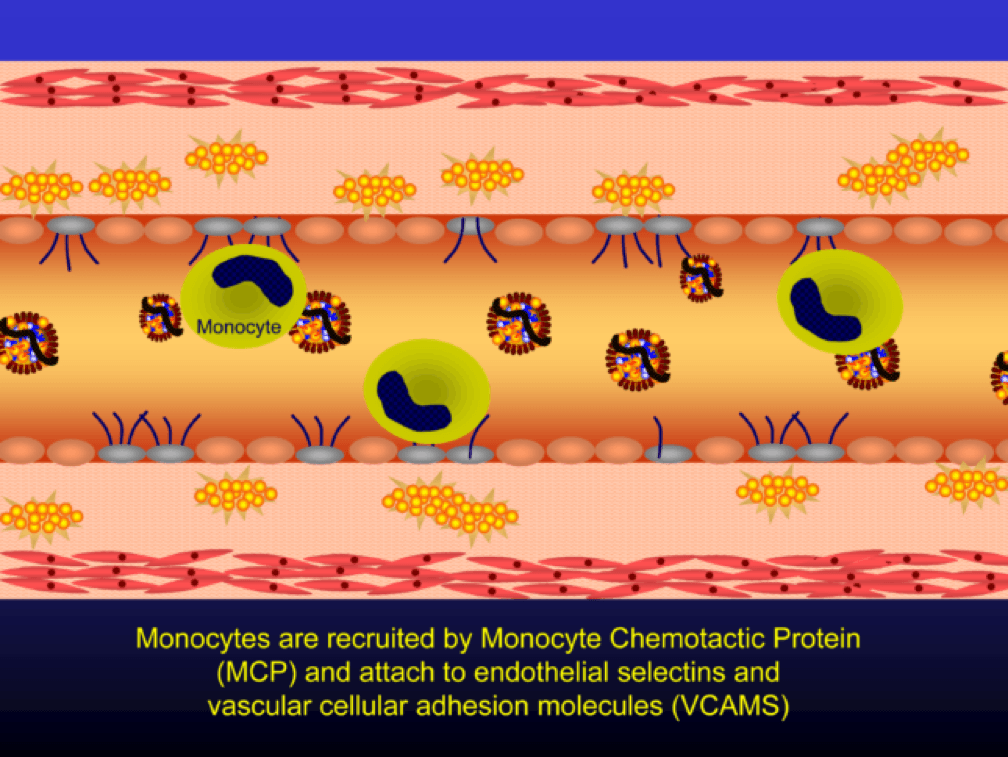
Selectins and VCAMS increase monocyte adherence to the endothelium.
The endothelial cells also express messenger cytokines such as interlukin-6 (IL-6) and tumor necrosis factor (TNF) which circulate to the liver and induce the production of C-reactive protein (CRP).
Monocytes penetrate the subendothelial space…
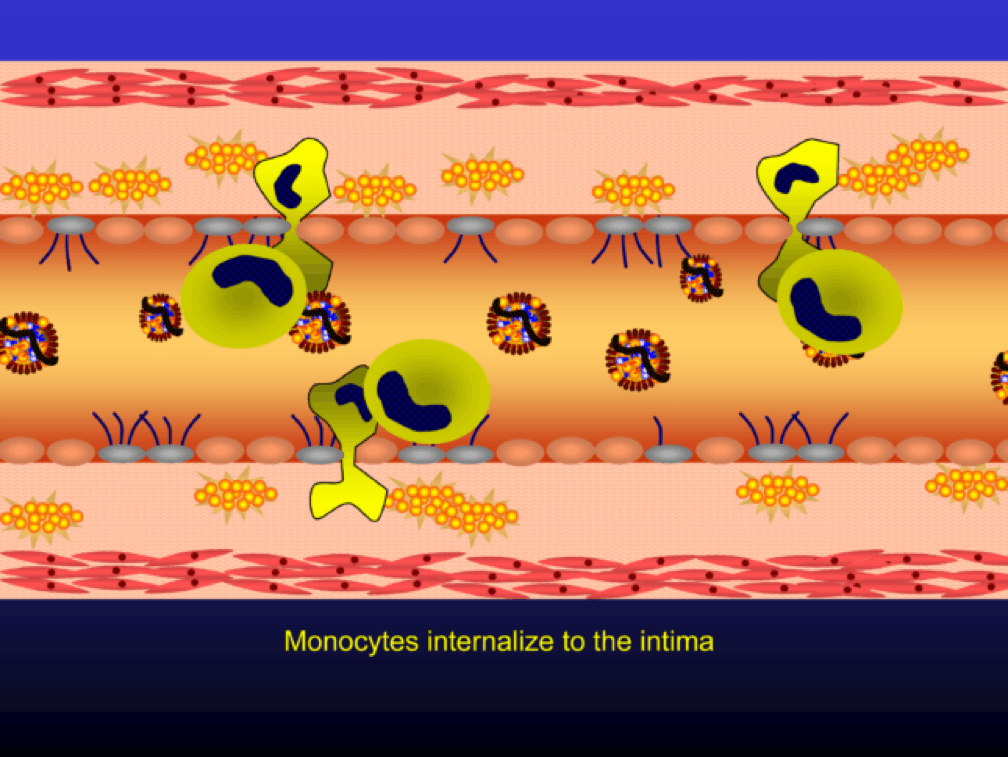
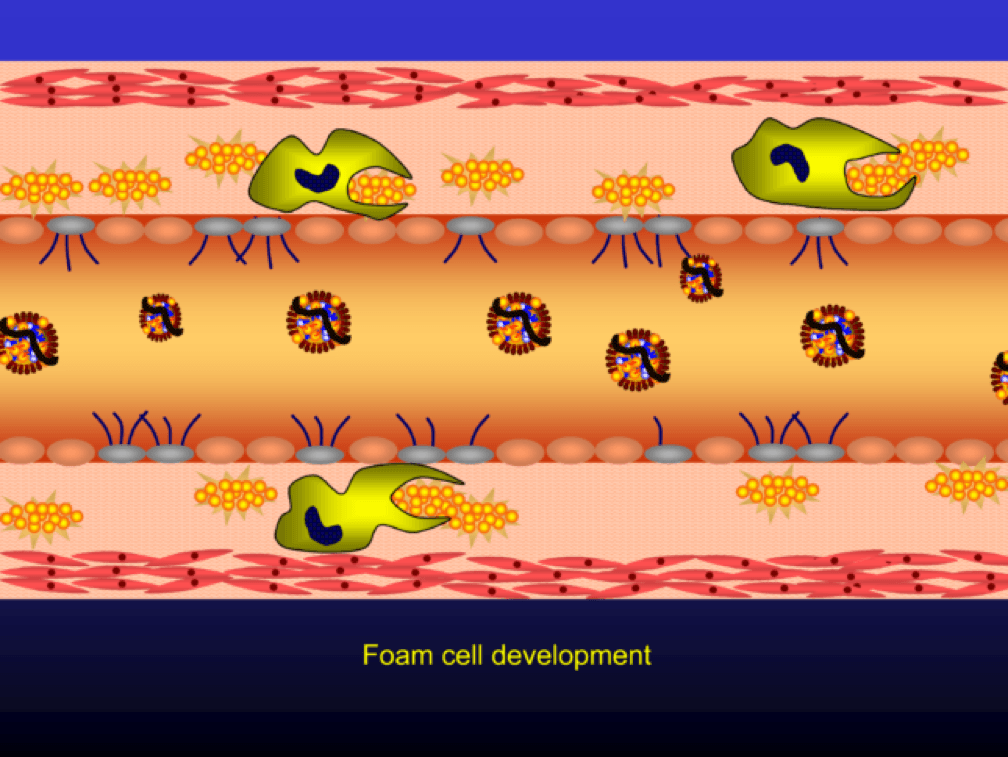
…and when they do, the monocytes differentiate into (i.e., “become”) macrophages (a more specific type of immune cell). Macrophages phagocytize (basically “ingest”) the modified or oxidized LDL particles.
The phagocytosis of oxidized LDL particles (oxLDL) and accumulation of lipid in the macrophage creates something called a foam cell.
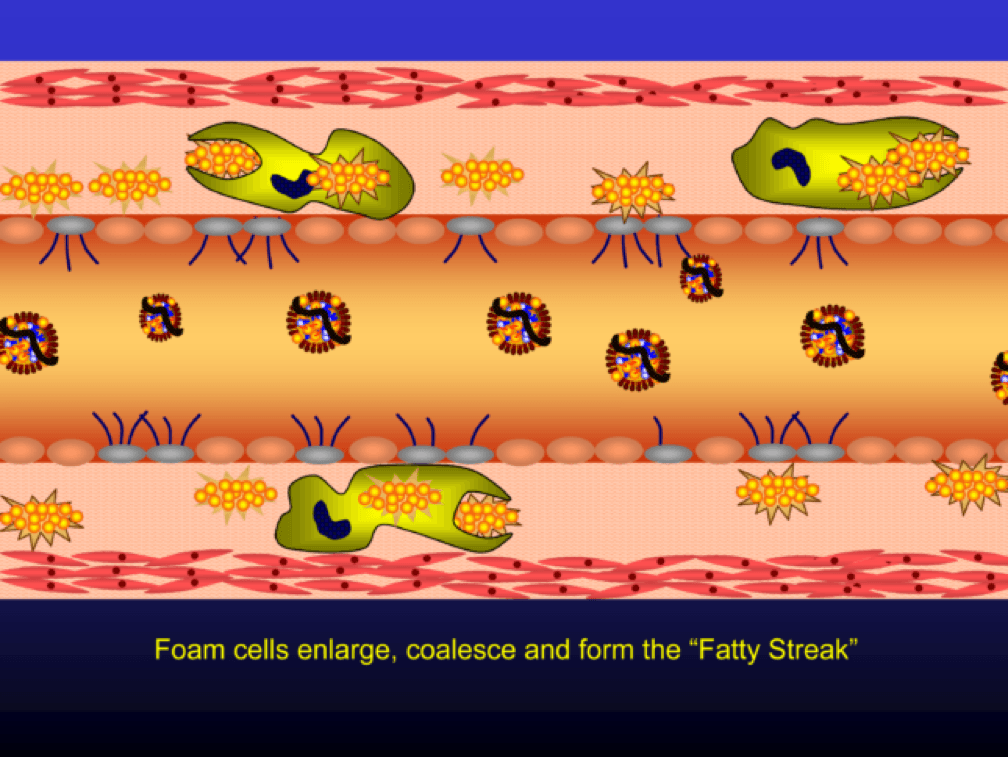
Multiple foam cells coalesce to form the characteristic fatty streak, the hallmark of an early atherosclerotic plaque. Keep this in mind. Later in this post we’ll come back to “fatty streaks” and I want you to remember how much has taken place to get us to this stage. I will posit that no one reading this post does not have fatty streaks unless there are some brilliant 5-year-olds reading this during recess..
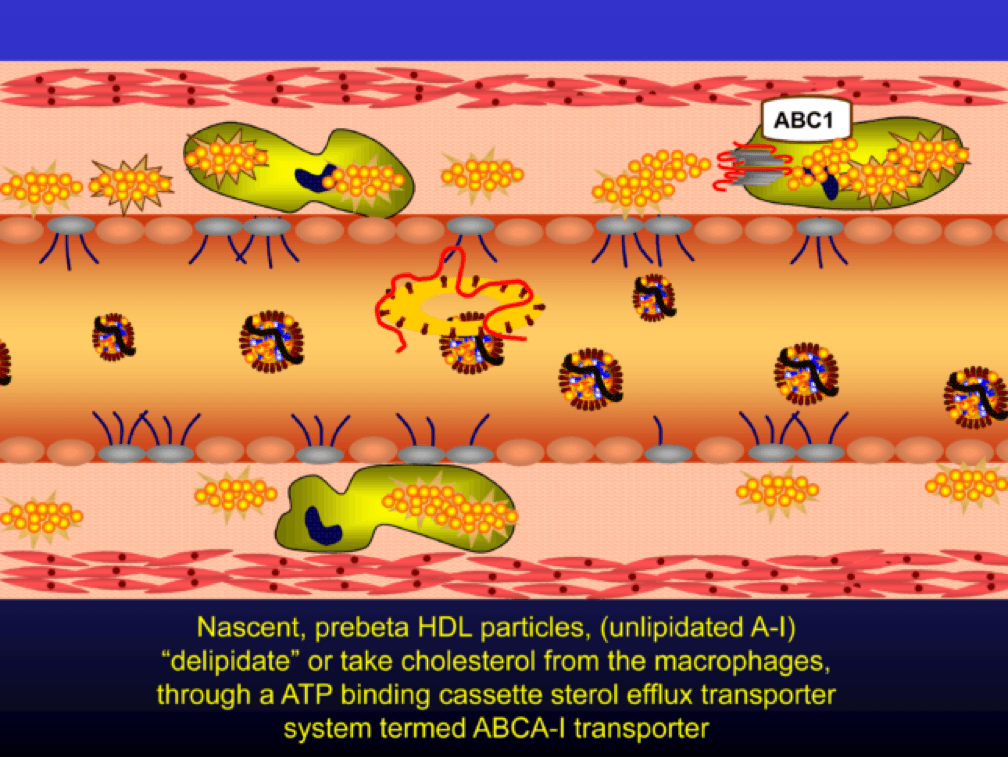
Nascent Apo A-I containing particles (also known as prebeta-HDL particles) accumulate free or unesterified cholesterol from the macrophages using ATP Binding Cassette Transporters A1.
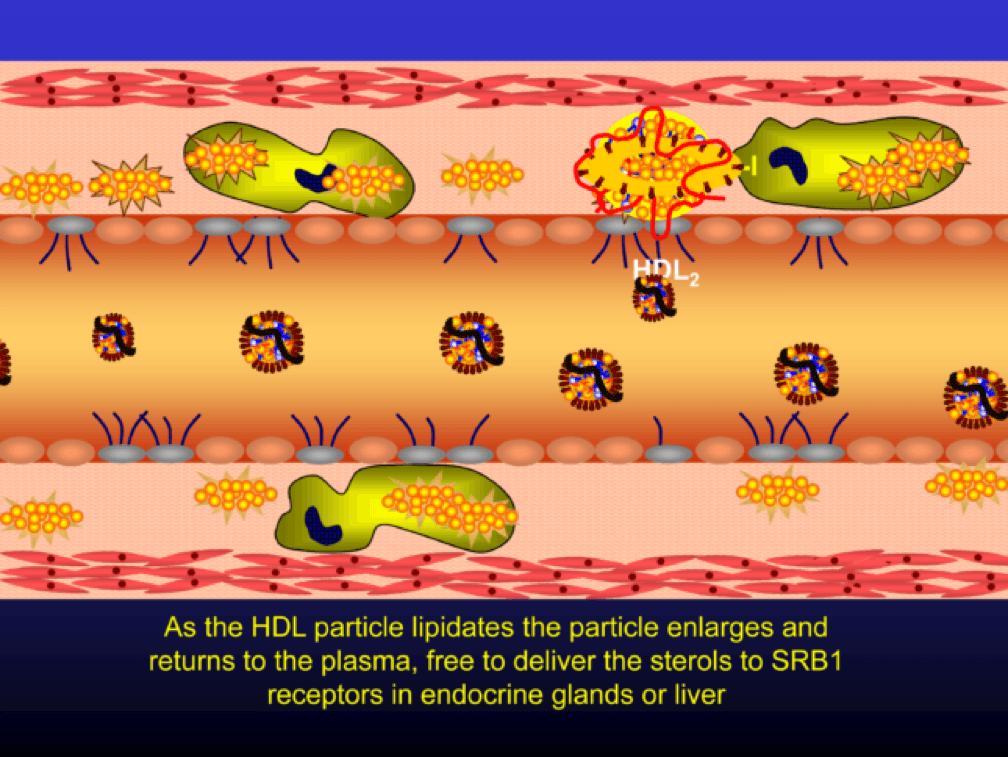
As the HDL particle lipidates itself by delipidating the macrophage (i.e., takes lipid out of the foam cell), the HDL particle, utilizing an enzyme called LCAT, esterifies the free cholesterol forming cholesteryl ester (CE). As a result, the HDL particle enlarges and is free to be delipidated at a variety of tissues. HDL delipidation occurs through multiple mechanisms using Cholesteryl Ester Transfer Protein (CETP), aqueous free diffusion, SRB1 receptors in endocrine glands or gonads (e.g., to make hormones), adipocytes (a major cholesterol storage organ) or the liver (e.g., to package for biliary delivery). HDLs can also be internalized as entire particles by surface liver receptors.
A brief, but important, digression: the complexity, above, is probably the reason why every trial that has tried to increase the concentration of cholesterol in HDL particles (i.e., raise HDL-C) has failed, and failed epically, to reduce events. The value in HDL particles (the so-called “good cholesterol”—my god I hate that term as much as I hate the term “bad cholesterol” when referring to LDL) is almost assuredly in its functional capacity—what it is doing that might be cardioprotective (very hard to measure) rather than its cholesterol content (HDL-C), which is relatively easy to measure, but probably offers zero insight other than its positive epidemiological associations. In other words, measuring HDL cholesterol content tells you little about its cholesterol efflux capacity or any other of the numerous HDL functional properties.
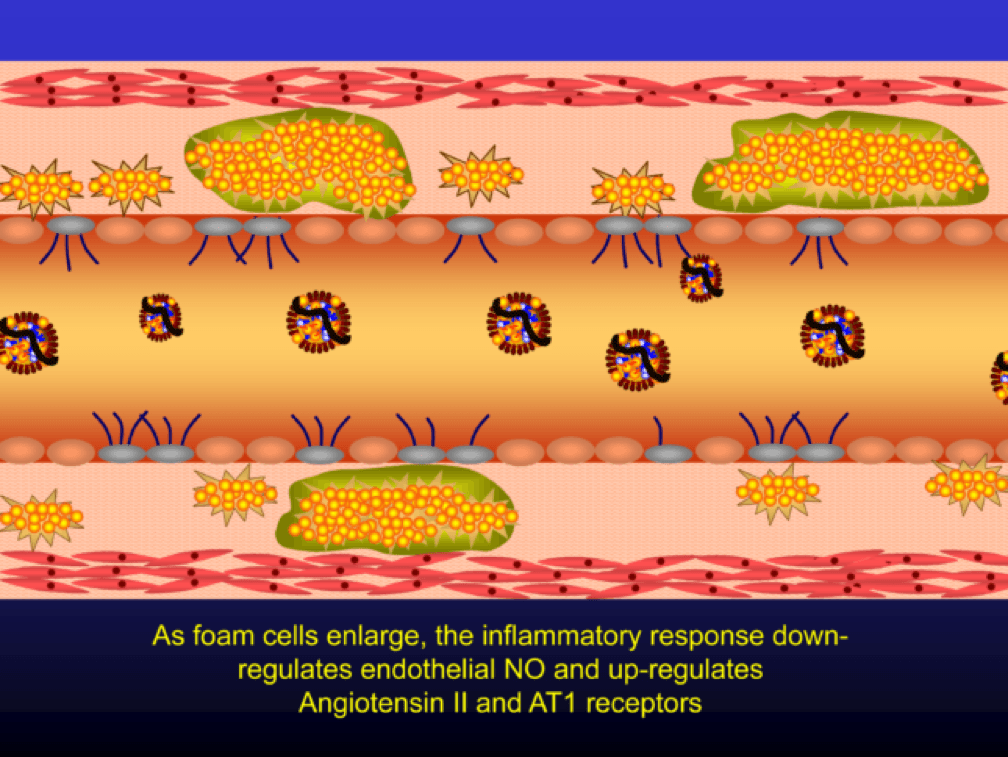
Macrophages that become engorged with oxLDL remain full-fledged foam cells. Foam cells produce Angiotensin II, metalloproteinases, collagenases, elastases, and other proteins, which undermine the integrity of the arterial wall, causing more endothelial dysfunction. This is where the process goes to hell. Now you’ve got a damaged barrier and the looting begins. Oh, by the way, the process to date goes unnoticed by the calcium scan and CTA.
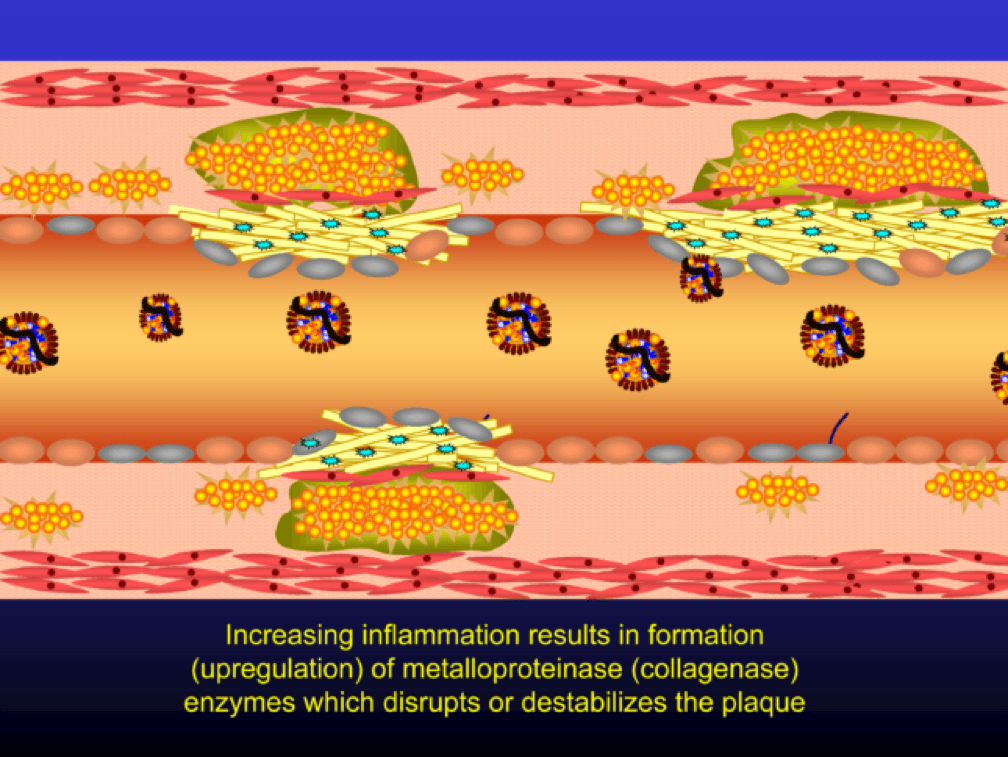
Chemotactic factors (i.e., chemical signals) trigger migration of smooth muscle cells to the area of injury in an attempt to repair the damage and pervert further disruption. Again, all of this is taking place in good faith on the part of the immune system. The smooth muscle cells are transformed into secretory cells that lay down a matrix to heal the injured wall. This matrix becomes the fibrous cap of the atherosclerotic plaque. Only now is the arterial lumen becoming encroached.

Metalloproteinases and collagenases are upregulated and they start to dissolve or weaken the plaque cap, typically at the shoulder regions where the diseased endothelial cells meet healthy endothelial cells. Some have used the term “vulnerable” to describe such plaques, which may be a correct term, but it also gives a false sense of confidence that we can treat atherosclerosis on a lesion-by-lesion basis. History has taught us that such hubris is unwarranted. Until proven otherwise, atherosclerosis should be viewed as a systemic condition of the arterial system. To see one of the best (and my favorite) papers on this topic, look no further than to this paper by Armin Arbab-Zedeh and the venerable Valentin Fuster, aptly titled “The Myth of the Vulnerable Plaque.”
The plaque can become obstructive—i.e., it can obstruct the lumen—over time. Lipid rich plaques are unstable, and can rupture. Platelets adhere to the ruptured surface of the plaque through electrostatic factors and through binding to specific ligands.
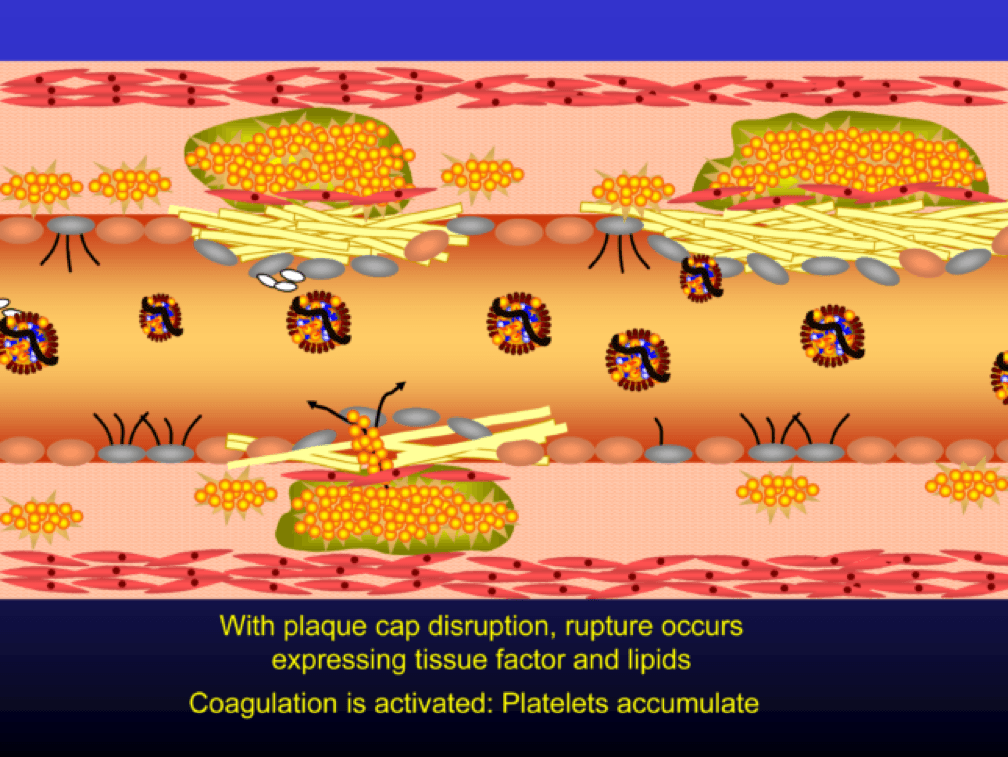
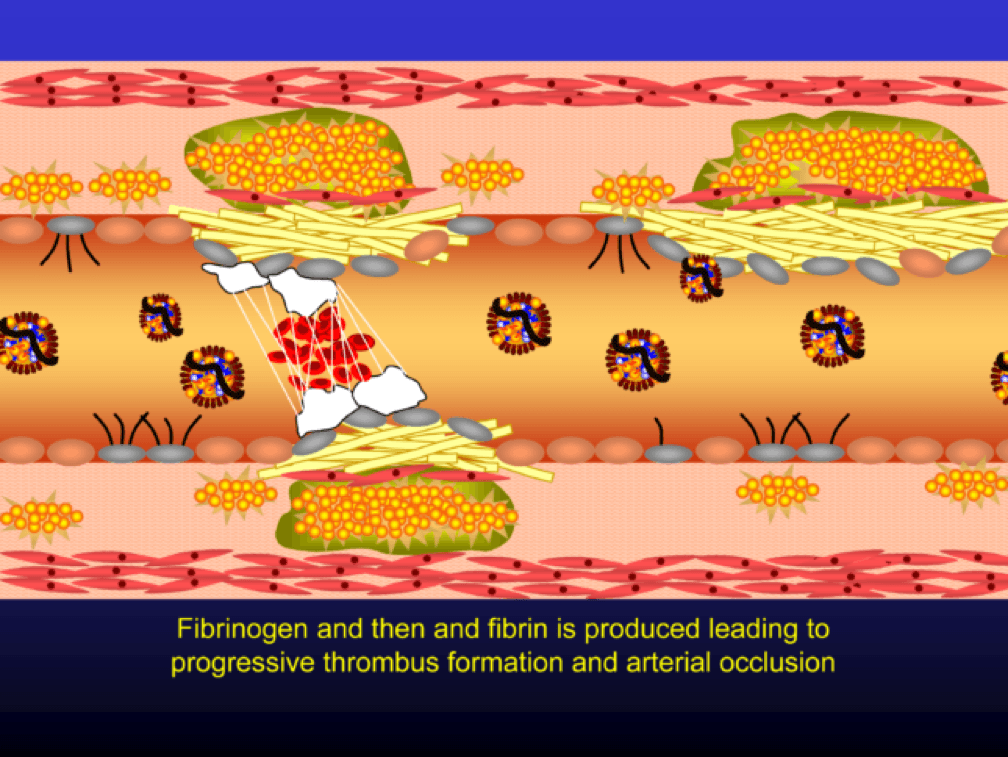
The platelets then serve as a cradle for the coagulation cascade to produce a net of fibrin (the white “net” in the figure), leading to a red clot, as red blood cells are caught in the net. A non-obstructive plaque can lead to a clinical event after the superimposition of red and white thrombus, which can occur quickly and without warning. The degree of stenosis (luminal narrowing) does not predict when this will happen.
Why all of this matters
So back to this impetus for this post—Allan’s editorial. When I first met Dr. Allan Sniderman, we immediately hit it off. Like Tom, Allan has been a remarkable mentor and teacher. In fact, one of the gifts Allan gave me a while back was his personal copy of Herbert Stary’s legendary pathology textbook on atherosclerosis, Atlas of Atherosclerosis Progression and Regression. I devoured this textbook and have since purchased additional copies to always have one on hand. Ask my patients…most of them have had to sit through viewings of it like it was a vacation photo album.
Allan and I were having dinner and discussing our favorite topic. Allan asked me to guess what fraction of cardiac events (“event” is a pretty common word in the vernacular of cardiovascular disease and basically refers to a Q-wave MI, the need for re-vascularization, or cardiac death) take place in North America in those younger than 65. I knew it was a loaded question, so I rounded my guess up to 25%. I was wrong. How wrong I wouldn’t find out until Allan and his colleagues completed their analysis which formed the basis for their editorial recently published in JAMA Cardiology. Add it to your weekly reading list.
You don’t have to be a lipidologist or a pathologist to understand this paper, but it helps to understand the basics of math—big denominators can drown out even modest numerators. The aggregate figure from this paper is one of the most elegant representations of a dot product. The subfigure on the left is how most doctors (myself included until the 2nd decade of the 21st century) and authorities think of coronary heart disease (CHD)—it’s virtually silent until the 7th or 8th decade of life. What folks who think this way miss is the middle figure—the population base (the “denominator”) is shrinking while the incidence (the “numerator”) is rising. In a situation like this, the only way to really see what’s happening is to do what Sniderman et al. did—calculate the absolute event rate, as shown on the right.
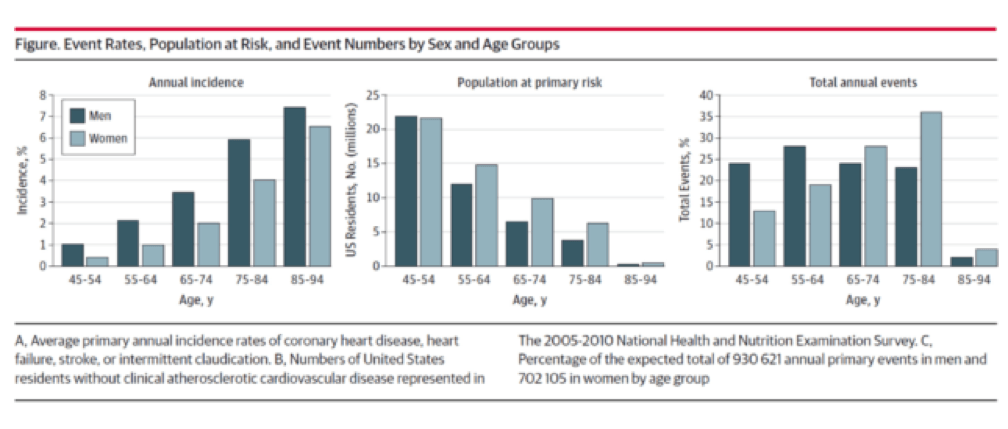
Yes, you’re reading this graph correctly. A little over half of all events in men (24% + 28%) and a little less than a third of events in women (13% + 19%) take place below the age of 65.
Tying these two insights together
Insight #1: Atherosclerosis takes a long time to evolve, and involves many steps.
Insight #2: Many cardiovascular events—half in men and one-third in women—take place in young people (i.e., those 64 or younger)
How do we reconcile these findings? Enter the pathologists. As I mentioned above, my first year pathology professor in med school insisted that pathologists were the only doctors who really understood heart disease, because they actually did the autopsies and examined the coronary arteries under microscopes.
And this brings me to my point. The only way Insight #1 and Insight #2 can be correct is if atherosclerosis takes a long time to develop. Any guesses as to what the greatest single risk factor is for heart disease? Smoking? Nope. High blood pressure? Nope. The wickedly deadly particle I have yet to write the most deserving post on, Lp(a)? Nope. LDL-P or apoB? Nope. LDL-C? I thought I told you to never say that again. CRP? Nope. None of these things. It’s age. Age trumps everything. In this sense, atherosclerosis is an “integral” disease (in the calculus sense of the word)—meaning it’s a disease of compounding injuries, as I painstakingly went through above. Age = persistent exposure to LDL-P/apoB.
Just like wealth is compounded in a highly non-linear way, so too is illness and no disease to my knowledge does so more clearly than atherosclerosis. So the jugular question is when do we need to start treating patients? That is a question I can’t answer for you. Not because I don’t have a point of view, which I most certainly do, but because it comes down to risk tolerance. I can no more impart my world view of this problem on you (though the answer seems painfully obvious to me) as I can my world view of how to raise kids or combat ISIS. But I do hope to leave you with a clear picture, at least of the disease process.
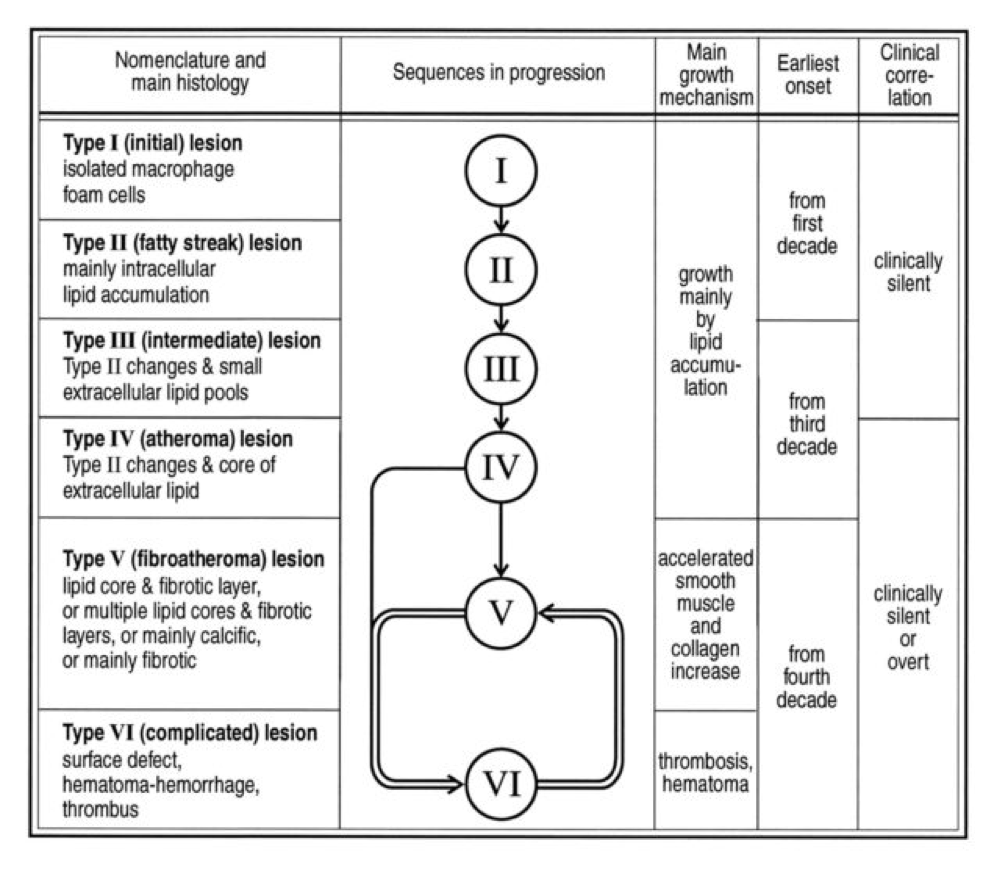
Perhaps the greatest insights into the pathogenesis of atherosclerosis, especially as they pertain to age, comes via autopsies of two variants: those of people known to die of some cause other than heart disease and those known or suspected of cardiac death. The table, below, taken from this paper, summarizes the six stages of atherosclerosis. Stary’s stages are identical, except that he further divides the sixth of these stages into three stages, for a total of eight stages, but the points remain the same. The points being, of course:
- In the first decade of life fatty streaks are being formed. That’s right, before the age of 10.
- Atheromas are present by the time most people are in their 20’s.
- By the time you are in your 30’s you are quite likely to have fibroatheroma formation.
- The vast majority of atherosclerosis-initiating sterols get into the artery as “passengers” in apoB-containing particles most of which (90%) are LDL particles.
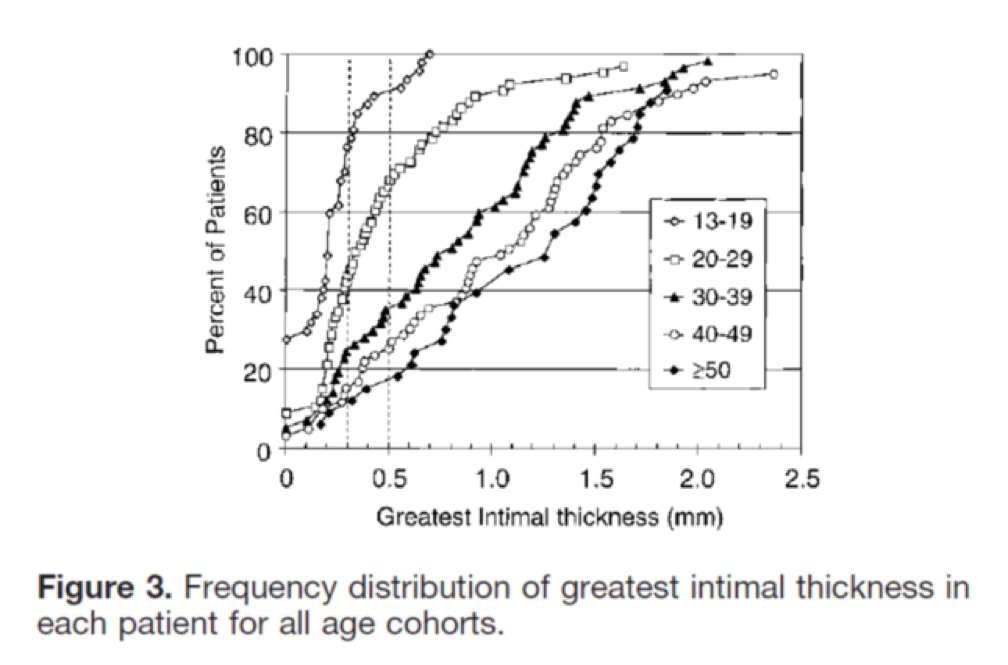
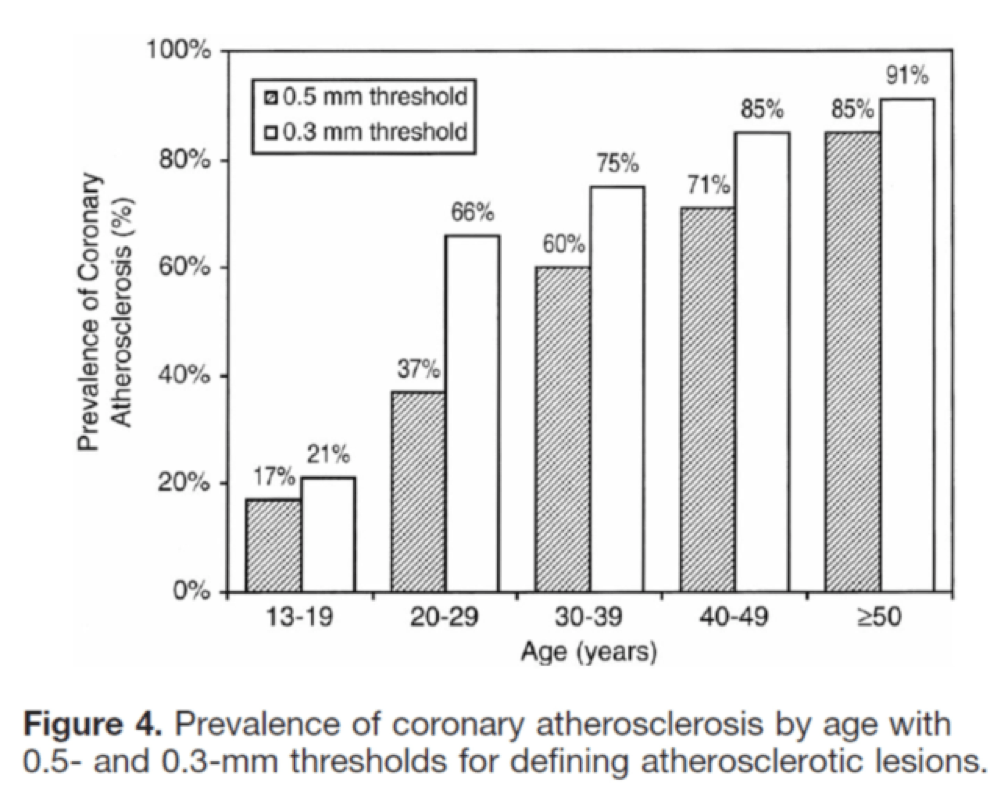
I’ll close with another interesting study, published in Circulation in 2001. The title of the study—High Prevalence of Coronary Atherosclerosis in Asymptomatic Teenagers and Young Adults—pretty much tells you what they found. The authors performed intravascular ultrasound (IVUS) on 262 heart transplant recipients about a month following their transplant. Before going any further, it’s worth pointing out that IVUS is not as sensitive as pathologic sectioning so this study is likely underestimating the degree of disease present in the hearts (but obviously one can’t section the coronary arteries of donor hearts). By doing the IVUS on the recipients so soon after they received their transplant the authors were able to study the hearts of the donors, many of whom were quite young.
The figures below, both taken from the paper, show the frequency distribution and prevalence of intimal thickening for each age cohort of donors. Consistent with the pathology studies, which actually cut open the arteries and examined them histologically, the IVUS study found a similar trend. Namely, atherosclerosis is starting much sooner than previously recognized. In this series of 262 heart donors, one out of six hearts donated by a teenager was found to have clinically measurable atherosclerosis. The authors conclude: “These findings suggest the need for intensive efforts at coronary disease prevention in young adults.”
Final thoughts
I was 35 years old, the year my daughter was born, when I first confronted my own inevitable demise which, based on my family history, was likely to be a cardiovascular one. I’m sure I’d be better off if I had that epiphany when I was 25 or possibly 15, but I’m glad it happened when it did. Today, I manage all modifiable risk factors to the level of my risk appetite and interpretation of the most nuanced scientific literature on cardiovascular disease. Does this mean I won’t succumb to heart disease? Of course not. But this is a stochastic game and the objective of the game is to increase the odds in your favor while delaying the onset of bad outcomes. It’s up to each person, and his or her doctor if necessary, to determine how aggressively he or she wants to confront the inevitable—we all have atherosclerosis at some level.
Addendum
Let me add another thought that may address some concerns.
Clearly there are factors here we (at least I) do not understand. Why do some people just stop with fatty streaks and stay that way for decades, while others progress to clinically significant heart disease? I’m sure if one normalizes for LDL-P, Lp(a)-P, and even particle size, the answer will still elude us (me). I think what people are missing here is that there is a difference between what we can infer from population-based (i.e., heterogeneous) statistics–clinical trials with drugs, epidemiology, ecology, hundreds of autopsies–and what happens at the individual level. Furthermore, the only probabilities that matter when it comes to an individual are “0” and “1”–in other words we go from the most heterogeneous to the most homogeneous.
I’m reminded of an analogy Allan Sniderman shared with me: If you’re a parent, with kids in your home, and want to know the probability that your child (or any child in your home) will die from an accidental gun shot wound, you can look at the stats, which are readily available. They will say the risk is actually pretty low–which it is on average. But what if we now adjust the information (in the Bayesian sense of the word) and note that you have a loaded .45 under your pillow (you know, for home protection). Now what happens to the risk? Of course it goes up dramatically. Why? Not just because we have “more” information–we actually have very specific “new” information. We have information about the causative agent, the gun. LDL-P and Lp(a)-P are the causative agents, and while other forces matter (e.g., inflammatory response), there is no getting around the fact that high LDL-P and Lp(a)-P are stacking the odds against you. The gun won’t pull the trigger on its own, but it’s still the causative agent. People are too quick to confuse “necessary and sufficient” with “necessary but not sufficient”–in both cases reducing the “necessary” component helps.
While I do not doubt that some people with high LDL-P and Lp(a)-P may be immune to the typical “rules” of atherosclerosis, we don’t have good enough tools to predict this, especially non-invasively. Ergo, the risk of doing something to lower these modifiable risks, even if that means taking drugs, must be weighed against the risk of doing nothing. This last point is often dismissed.
Most kids in homes with loaded guns will not die from those guns, but to ignore the loaded gun in that setting is crazy, in my opinion.
I’m going to remove the gun and put the odds back in my favor.
Image credit: Dr. Edwin P. Ewing, Jr. Gross pathology of atherosclerosis, aorta. Autopsy specimen of aorta has been opened lengthwise to reveal luminal surface studded with lesions of atherosclerosis.

Dear Dr. Peter,
Thanks for your wonderful post.
I am heartened by your reply to Carol on how to control LDL-P particle number: “… do not discount the ability of diet to control this process.” I sincerely hope you will go deeper into the dietary aspects of LDL-P control in future posts.
I have been doing great on LCHF for several years – also lost significant weight. But a recent lipid test (unfortunately can’t get NMR test in Singapore) showed that my conventional numbers are through the roof. Even though I do not know what my LDL-P number is, I am assuming that my LDL-C is concordant with it, and have stopped eating SFA as much as possible, use MUFA whenever I can, and reintroduce reasonable amount of carbs back to my diet. Hope to do a conventional lipid test again in 2 months to see how the numbers are trending, before exploring other options – I guess including pharmacology.
You have posted previously that dietary cholesterol have very very little to do with serum cholesterol. Are there individuals that respond differently? Do you think it makes sense for someone with high LDL-P after LCHF to experiment by cutting out eggs from their diet, for example?
Once again, thanks for your wonderful blog.
I alluded to this very briefly in a previous post, but I don’t recall which one. Definitely in the past 3 or 4 posts. I think some time in 2015.
Leung,
If you find the post that Peter is referring to, would you mind sharing a link as a follow-up comment here?
I too am interested in the answer to that question.
Thank you!
Hi Naren,
I could not find specific comments about eggs, but I did find one concerning tolerance to dairy. The question was whether there is a lab test to prove dairy tolerance.
Dr. Attia’s reply:
“Not that I know of, and even if there was a way, I wouldn’t trust it. The gold standard is elimination. Knock it completely out for a month and see what happens.”
I guess we need to do the same if we want to know if eggs can affect our LDL-P, eliminate and see what happens?
(Dr. Attia, is this the post you meant? Thanks)
The question was asked by Aubrey under “Random find (plus pi)”, about half way down the comments section.
Thank you for digging this up, Leung.
LDL particles pass through endothelial pores in all tissues including arteries, they are ever present and a low level risk factor for atherosclerosis. How they become oxidized along with foam cell function and integrity is a far more worthwhile field of study regarding early CVD events: https://link.springer.com/article/10.1007%2Fs00109-016-1385-4
Liver cell production LDL is promoted by insulin and would explain a marginal association between LDL and atherosclerotic events. Insulin also inhibits autophagy and promotes foam cell apoptosis and type 1 macrophage transformation. Dramatic reductions in insulin levels is possible by avoiding carbs, ketogenic diets and fasting and will reduce LDL levels as well as obesity, diabetes, inflammation, cancer risk, etc.
“LDL particles pass through endothelial pores in all tissues including arteries, they are ever present and a low level risk factor for atherosclerosis. How they become oxidized along with foam cell function and integrity is a far more worthwhile field of study regarding early CVD events”
That’s been done.
“One of the characteristics of oxidized LDL is the production of such reactive aldehydes as MDA and HNE by
the decomposition of lipid hydroperoxides (5, 9, 10). That both MDA and HNE become incorporated into the oxidized (ox-) LDL particle by covalently coupling to amino acid residues on apoB-100 is suggested by the result that monoclonal antibodies directed at LDL modified with MDA or with HNE cross-react with oxidized LDL (11). That one of the adducts formed between apoB-100 and HNE in ox-LDL is a Schiff-base is suggested from the similarity in fluorescence at 360 ex/430 em between HNE-modified LDL and Cu2+-ox-LDL (8, 10, 12). Thus, it is conceivable that LDL modified with both HNE and MDA might mimic ox-LDL in several structural and functional properties. Recently, we and others have shown that an LDL-sized fraction isolated from human atherosclerotic lesions demonstrates several characteristics of ox-LDL, primary of which are the reactivities with anti-MDA-LDL (13, 14), anti-HNE-LDL (14), and fluorescence properties characteristic of HNE-modified LDL (10). Thus, lesion-derived LDL appears to be modified by both HNE and MDA.”
“Structural and functional changes in LDL after modification with both 4-hydroxynonenal and malondialdehyde”
https://www.jlr.org/content/34/7/1209.long
Remember, the precursor to both HNE and MDA has risen dramatically in the last 100 years, and is not a normal part of the human diet in the high doses currently consumed…
Hi Peter –
Thanks for starting to post more regularly. I’m a big fan of Dr. Dayspring’s and always feel like reading you is having someone who can communicate to mortals help us through the wilds of biochemistry.
Always love your take on things – I’m Lowish Carb but very mindful of all clinical markers- including good ol’ LDL-P.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4061377/
Am I reading the above article correctly that fasting could reverse atherosclerosis? Do you think there are some potential benefits to CVD risk from fasting?
Keep up the excellent work – looking forward to it.
Michael
If you buy that your fasting regimen (fasting a pretty broad term) induces enough autophagy to reverse the process I describe.
Hi Peter! Great article!
I’m curious to learn more about the interplay between carbohydrate consumption and changes in LDL-P, as insulin and glucose relate to particle clearance, inflammation, and the potential for oxidized & glycated lipoproteins, which drive atherosclerosis.
I’ve read that brief periods of hyper-caloric starch intakes in the post-workout window increase insulin production to raise leptin / thyroid hormones which in turn promote increases in LDL particle clearance, lean body mass, muscle growth, energy production, fat burning, and quality of sleep.
I’m curious if it would be wise to remain in uninterrupted HFLC territory, or if it might be wise to have a post-workout “high-carb re-feed day” a couple times a week or some other strategic injection of carbohydrates for the purposes of increasing lean mass / balancing hormones. Or, if moderation is the key, somewhere in that consistent ~50-100g carb per meal low-carb diet. Which eating strategy do you tend to lean more toward with health+fitness in mind? (Or, is there a better, more nuanced approach?)
Dear Dr. Attia,
Oops. Will go back to re-read your 2015 posts again. Thanks
I came across a recent talk by Dr. Sarah Hallberg where she hypothesized that very low insulin level from LCHF could be a possible reason for raised LDL-P:
https://www.youtube.com/watch?v=w8jUmCe3zDs&spfreload=10
(from about 14:50)
Can I get your views on the possible mechanisms she described?
Thanks again,
Hon Yew
Hi, Peter, your posts are always a treat. Here’s a summary I (and the rest of the medical world) received today, which will certainly cause much new controversary:
Study Cites the Fats That Could Shorten Your Life
TUESDAY July 5, 2016, 2016 — Hold the butter, margarine and high-fat dairy: A new study supports the notion that these “saturated” fats are bad for you.
The study, which followed more than 126,000 people for three decades, found that people who ate higher amounts of saturated fats and trans fats died earlier than those who stuck to healthier unsaturated fats.
Unsaturated fats include plant-based, unprocessed fats such as those found in olive, canola or soybean oil, the study authors explained.
“These findings support current dietary recommendations to replace saturated fat and trans fat with unsaturated fats,” concluded a team of researchers led by Dr. Frank Hu of Harvard School of Public Health in Boston.
Source: The study was published online July 5 in JAMA Internal Medicine.
We should probably stop using the word “study” to describe epidemiological exercises with low hazard ratios.
The majority of people in these large cohort studies would be eating grain-fed meat which has a different and more inflammatory composition of saturated fatty acids compared to grass-fed. I’d like to see a study following people that only eat animals that are fed their natural diets, I bet the slight risk would disappear.
Hi Dr. Attia,
Can CT scan Coronary Calcium scoring detect or distinguish from Mönckeberg’s arteriosclerosis and the type of atherosclerosis you are discussing?
Thanks for the blog..it is a great resource.
You’d have to ask a radiologist, which I’m not, but my guess it that a CAC probably would NOT but with a CTA you would have a better shot at differentiating.
An excellent overview of the gory details of LDL oxidation and damage that is intimately involved, if not causative, of atherogenesis. I’d wager high LDL-P count is the result of LDL that is so damaged the body can’t clear it. Remove the cause, remove the problem?
“Oxidized LDL: Diversity, Patterns of Recognition, and Pathophysiology”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2877120/
Remember, both HNE and MDA have the same precursor. Peter, perhaps you can pass this along to Dr. Dayspring?
Hi Peter, Dr. Attia,
I am a 35 y/o Taiwanese American woman, based in Los Angeles (went to school down in San Diego), who was diagnosed with Type II Diabetes a few years ago, out of the blue. I have always been careful (aka wary) of diabetes since my mother has been a diabetic all my life (and is one of the most disciplined diabetics I’ve known), and has always been a nazi about “preventative measures” with her kids. My glucose levels were in the 70-90 range all my life, so I was never worried, but a few summers ago it suddenly jumped from one summer of 70-90 range, to the 150-180 range. And hence, my journey with battling Diabetes II began.
The doctor I was working with then had suggested that the sudden increase may be due to my anxious personality, and workaholic lifestyle and after procrastinating for a year, I quit my executive corporate position 3 years ago, and took a very long, needed sabbatical. Experimenting with different things, as the case with many diabetics, I have been through highs and lows, and am now happy to say that I am hopefully on the road of managed, type II diabetes.
I came across your TedMed Talk about your research, and am so so so so SO (you get the idea) moved, and touched by your talk, as well as the work you do, the passion you convey, that I had to essentially google-stalk you (sorry) in hopes to just see where you are at as of this year. I am so impressed by the incredible impact of your obvious genius and yet simultaneous humility, and clearly, the topics you speak of hit close to home.
Seeing that I go to San Diego all the time and that you mention you have a practice there, I was wondering if there is any way I can work with you (as a patient, as a marketing professional pro bono simply because I believe in what you do, as a friend), or at least follow your work so that I can work on trying to make those changes in my life too. Doctors tell me all the time how “young” I still am, and have to really get on things, and I know it’s an impending doom if I don’t “get with the program.”
Hope I haven’t completely creeped you out with my comment here, and sorry it is so personal and yet so public– I also find it SO AWESOME, that you personally respond to comments here.
Thanks, and hope to connect with you,
Lillian
Question: why do some macrophages get de-lipidated whilst others go on to become foam cells? Do all foam cells end up as fatty streaks? Any of this process able to be halted or reversed? Thanks
Peter – What about the issue that LDL-P only contributes partially to the CV risk burden ? I have several 8th decade patients with extremely high LDL-P yet no major CV event has occured. Surely they have a fairly high AUC for overall CV risk . Yet no events . Perhaps their early life was very active and their early nutrition was whole food oriented . That would have delayed the progression of CV risk and reduced the AUC ( especially if there is some sort of critical “window ” effect on developing lesions ) I am speculating here but I do worry much about spending resources on tests that make little substantive difference.
Did you ever run across this article?
https://circ.ahajournals.org/content/119/17/2396
From Dr Samia Mora – it argues against too much use of LDL-P over nonHDLC .
Thanks for your blog . Appreciate the thought provoking nature it exudes.
Everything only contributes partially, including smoking and hypertension. The HRs are all individually quite small.
I wonder if anyone has thought about the following: smaller LDL particles have a fundamentally harder surface than larger LDL particles, and are more likely to penetrate deeper into sub-endothelial spaces. Why do I imagine this: oil and water do not mix; oil has a cohesive energy that decreases when it meets water. So it forms a sphere to maintain cohesion. That sphere has a surface tension. I rarely see this mentioned in the literature around atherogenesis. The outer layer of any lipid sphere in water is like a drum skin. The larger the particle size – the looser the drum skin. The smaller the particle size the tighter the drum skin – i.e. the more desperately the small particle is trying to maintain cohesion. The small particle will have a ‘drum skin’ so tight it will actually be overpressurized relative to the water around it. So what’s more likely to penetrate past the endothelium – a large, floppy, liquid-like sphere or tiny hard pellet? Once in the subendothelial space this collection of small spheres has a very high surface area-to-volume ratio for oxidation reactions. The rate at which the lipid within oxidizes should be faster than for a larger sphere. Having high blood pressure only makes “all of the above” worse because it forces lipid spheres to be smaller (and therefore harder) as a response to high-arterial pressure.
Hi Peter !
Thanks for your reply on Lp(a) – agreed there’s a lot more going on here – with Lp(a) kinda carried along for the ride perhaps. ???? Multi-factor fun I guess.
Anyway, on to more serious matters. I thought a little at the weekend while preparing slides for an upcoming talk I’m giving (to big group of Paramedics). I drifted down the ApoB hole whilst doing a simplified Root Cause Diagram (to help them understand the basics of CHD driving mechanisms).
My thoughts on ApoB as an independent driver surfaced as I drafted. There are lots of comments already on this post (unfortunately they are chronologically ordered from the bottom one up – Squarespace, eh?). Anyway, would be interested in your thoughts – although I will understand if you are too busy to run through the content…
https://www.thefatemperor.com/blog/2016/7/9/atherosclerosis-high-level-root-cause-the-apobldlp-question
Thanks as always for your assessments
Best
Ivor
https://www.thefatemperor.com
Ooops nearly forgot – I have some contrasting views on CAC too, which would be cathartic to air and have assessed. Angiograms are questionable I think – they look at narrowing, an aspect of the disease by all means. But can be misleading in terms of plaque rupture likelihood (i.e. most MI’s). But CAC looks at the disease process itself. Far more satisfying to an engineer (in my case anyway). I only show snippits of the myriad studies here – but all tend to agree. I’m not sure what I’m missing – honestly. And cardiology giants Brundage, Rumberger, Hecht, Budoff, Agatston, Davis and others all agree. Also the extraordinary physicist Doug Boyd, whose genius created the method, has been very clear on the fundamentals.
https://www.thefatemperor.com/blog/2016/7/11/the-power-of-calcium-score-because-it-sees-the-disease
My recent interview with Bruce Brundage is here. From 20mins onwards, he hits on some fundamentals. I would be interested in why CAC comes up in a very negative light in this post – I’m not sure you mentioned it before?
https://youtu.be/a7N6i1_uGqQ?t=20m25s
Best
Ivor
Hi Dr.Attia,
I want to congratulate you on your success via the eating academy and the other project you are excelling in.
I have learned a lot about you through a podcast with Tim Ferris and other videos.
I am originally from Syria and I am planning a Fundraiser cycling ride, and I have a couple questions about endurance training and how to hack my body to perform better during this ride.
please email me at [email protected]
your help is much appreciated.
Regards,
Feras
Dr. Attia, this post reminded me of my own M1 path lecture on atherosclerosis found in young soldiers who had died in Vietnam. Seems like we’ve known about this for a while, but I unfortunately recall the takeaway being that we can’t do much aside from not smoke and avoid dietary “bad” cholesterol. On a side note, while teaching-hospital based residencies are great to appreciate acute pathophysiology after shit hits the fan, do you think physicians are being adequately trained on chronic disease prevention and management with respect to understanding causative factors?
I really don’t think so, Palak.
Dr. Attia. What strategy do you take for APOE4 patients with elevated cholesterol, in particular, LDL-P elevations? Some arguments have been made that APOE4 patients need more cholesterol to overcome the transport defects in the brain associated with the APOE4 allel. Others say lower ldl-p at all costs. Some say statins should be used especially if desmosterol is high while others say that high desmosterol is a good thing. Even as a physician I find this all so confusing! I’m feeling especially clueless when my patients are now coming to me with their 23andMe results in hand. Any tidbits you could share would be helpful.
Too complicated for a trite response, unfortunately.
Peter,
I have to say I’m a fan of your blog and so well written posts.
As a brazilian engineer and mother of two little girls I was gratefully surprised to know you are Senna’s fan!
Can’t wait for the book.
If only there were more doctors like you out there…
Congratulations on your approach on health!
Thank you, Priscilla. Senna forever.
Dr. Attia,
I really appreciate the time and knowledge you give everyone on your blog. Just curios, but I’ve read that calculating non-HDL (Total Cholesterol – HDL cholesterol=Non-HDL Cholesterol) is simple way to determine highly atherogenic lipoproteins. Is this formula too simplistic to have any validity?
With best regards,
Jerry
Too simplistic.
Hi Peter
Hope you’re well. I’ve learnt a lot from your previous blog posts, though I think this one is a bit technical for lay persons. I know you won’t be likely blogging for a year, but I just wanted to put a couple of things out there in terms of weight loss/your clinical practice as a GP, which might be interesting topics for you to blog on eventually. Not just in terms of the ‘state of the art’, but what relevance you see to them in terms of your day to day work.
I’ve struggled with weight loss, being obese since 7 myself, going down to a ‘normal weight’ in my twenties but developing an eating disorder to do so (exercise bulimia) and gone up and down in weight many times. I would think there would be a lot of overweight/obese people in your practice who fit that pattern.
However one of the good things/hopeful things that is occurring more recently is that (i think) scientists and doctors (endocrinologists in particular) seem to be becoming more accurate at working out the physiological factors relating to weight loss. These include some things other than strict low carb/high fat (though the advances seem to be in line with LCHF mechanisms for explaining obesity).
The things I was hoping you might address (in terms of day to day practice) are:
– What effect you consider vitamin d deficiency to have on insulin sensitivity/weight loss.
– Whether you counsel patients to have larger breakfasts (with a significant amount of protein) and to not eat at night.
– Whether, further to the above question, you see intermittent fasting as helpful for weight loss/control (I think I’ve read previously that you consider hunger might be generally counterproductive).
– Whether you counsel the use of low volume HIT exercise that can be done without ‘formal exercising’ e.g. sprinting up the stairs every day while going to work etc.
– The importance of the micro biome in weight loss e.g. in avoiding artificial sweeteners which tend to induce insulin resistance through their effects on the micro biome.
– The use of DNA testing to try to ascertain the particular metabolic strengths and vulnerabilities of individual patients.
I guess I am interested to see what an MD very interested and well read in weight loss thinks about the above. These seem to be some of the latest and greatest attempts by other doctors/scientists to help with weight loss.
Take Care
Mad Max