
In April I was part of a panel at the Milken Global Conference, the title of which was something like, “Keys to a healthier and more prosperous society.” The panel was moderated by Michael Milken, and it was great to meet him and his rock-star staff (especially Shawn Simmons, Paul Irving, and Nancy Ozeas). The other panel members were seasoned vets of the obesity discussion: Troy Brennan (Executive VP and Chief Medical Officer of CVS Caremark), Tom Frieden (Director of the CDC), Lynn Goldman (Dean of the School of Public Health at the Milken School of Public Health, at George Washington University), and Dean Ornish (president and founder of the Preventive Medicine Research Institute). I was the pauper in the group—no big credentials and zip-zero “panel” experience.
A few weeks before panel, we all jumped on a conference call and Michael set the stage for the discussion he wanted to moderate. He pulled no punches. “If you include the indirect cost—lost productivity, for example—the total cost of obesity and its related diseases is $1 trillion per year to our economy. This is unacceptable.”
Who could disagree? Hell, I usually only reference the direct cost of obesity and its related diseases—about $400 billion annually. But whether we talk about the direct or indirect cost of these diseases, I’ve always found the human cost even greater—every day 4,000 Americans die from four diseases exacerbated by obesity and type 2 diabetes: heart disease, stroke, cancer, and Alzheimer’s disease. Now that is really un-effing-acceptable.
So, back to the panel. The idea of being on a panel kind of freaked me out, even more than the sheer terror and vulnerability of TEDMed. No control. The possible need to be defensive. Sound bites over substance.
I don’t enjoy debates. Nothing comes of them. Just greater and greater polarization. The “winner” isn’t even necessarily the one with the best “facts.” Gary Taubes shared this quote with me recently, which I find really insightful. Dallas Willard, a well-known ecumenical pastor and theologian, was often invited to debate the existence of God and other matters. These invitations included Richard Dawkins himself. His response: “I don’t debate, but I am glad to enter into a joint inquiry. We will seek the truth together.” That’s the attitude I like.
In the end, I decided to just tell a few (in some cases provocative) stories. Why? Because it’s easy to present reams of data, yet so few people remember the point. (If you want to read an amazing paper on the importance of storytelling, check out this one by one of my former surgical mentors, Curt Tribble. You don’t need to care one iota about training cardiac surgeons to realize the gems in this piece.)
I realized going into this that I would be the contrarian in the group. I don’t claim to know all (or even many) of the answers, but I’m willing to bend over backwards in search of them. I realize folks (from readers of blogs to members of the audience at the Milken Global Conference) want facts, answers, prescriptions. I think we need to know more, first.
Below are the notes I made for myself in the days leading up to the panel. Basically, I wanted to tell a few stories, plus summarize it all (if given the chance). I didn’t actually “practice” this or even take notes up on stage (which I regretted when I realized everyone else was smart enough to bring notes), so if you decide to watch the actual video of the panel, you’ll note that I only vaguely followed what’s written below.
But in my mind, here’s how I thought about it. (I haven’t watched the video and I’ve pretty much forgotten anything I said, but I’m sure what’s written below is better than anything I said. I did send the video to two of the best speakers I know to get their feedback. Their feedback: could have been much better, but not the worst job ever. Lots of work to do for next time. Duly noted.)
How did I find myself interested in this problem?
My arrival at this place is really a coming together of two revelations. First, during my surgical residency at Johns Hopkins, not surprisingly, I was often dealing with the complications from diabetes and obesity in my patients. It slowly became obvious that all I was doing was slapping on the surgical equivalent of Band-Aids without ever addressing the underlying problem. I was treating symptoms and not the actual disease. When I would amputate the leg of a diabetic patient, which I had to do, regrettably, all too often, I knew that my patient was more than likely to be dead within five years anyway.
The second revelation was five years ago—September 8, 2009—to be exact. I remember it so clearly. My sport of choice was marathon swimming, and I followed what I believed to be the iconic healthy athlete’s diet. I had just completed an especially difficult swim into the current from Los Angeles to Catalina Island, becoming one of a dozen people to do that swim in both directions. After more than 14 hours in the water, I got on the boat to begin the long ride back to Long Beach Harbor, and my wife looked at me, in my speedo, 40 pounds heavier than I am today, and said, “Honey, you’re a wonderful swimmer. But you need to work on being a bit less not thin.”
And not only was I, well, fat, despite all this maniacal exercise, but it turns out I was also pre-diabetic.
Her comment launched me into a series of nutritional self-experiments. I was already working out three to four hours a day, so the problem couldn’t be sedentary behavior. It had to be what I ate. Over the next year I manipulated my diet until I found what worked for me, which paradoxically didn’t involve eating less, just eating very different from the food pyramid. Along the way I became obsessed with reading the nutrition literature. What I learned was that the evidence supporting our dietary guidelines was ambiguous, at best, and occasionally contradictory. There was a real dearth of evidence to support what seemed like the obvious questions.
I realized then, that if the guidelines didn’t work for me and if I can’t figure this out, with my background as a doctor and someone who studies healthcare, maybe they don’t work for a lot of people. Maybe there are systemic problems here. Maybe these problems were at the root of the ongoing epidemics of obesity and diabetes. Lots of maybes…and not a whole lot of clear, solid, unequivocal answers.
Since then, I’ve made a personal and professional commitment to finding the answers. And if the studies don’t exist to give us unambiguous evidence, then raising the funds and enlisting the researchers necessary to do those studies.
What does success in public health look like?
When trying to understand complex problems, I like to start with success stories, identify patterns and work backwards—reverse engineering success. Consider the following graph.
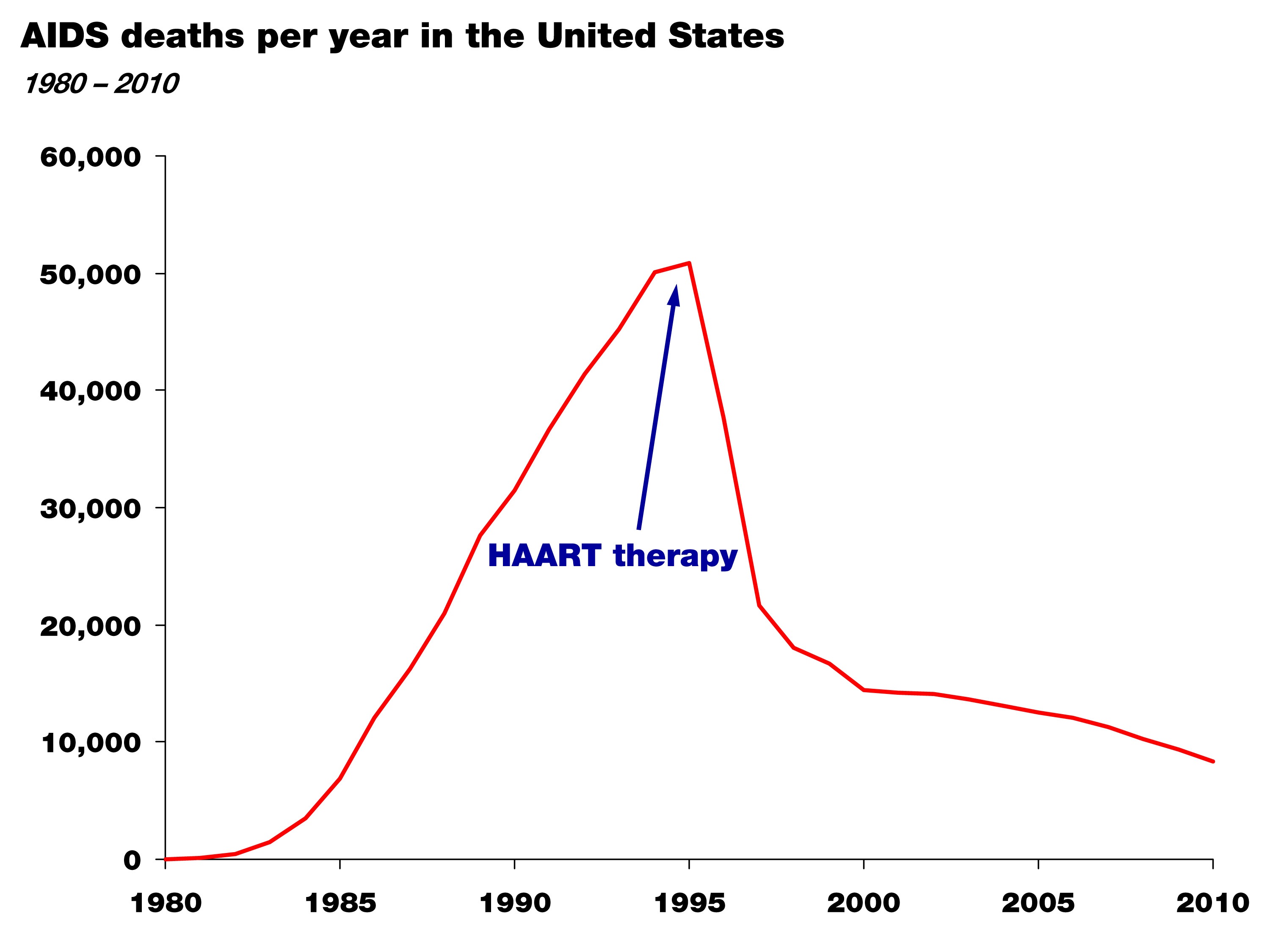
It shows the death rate from AIDS in the United States between 1981 and 2010. The point of this graph isn’t subtle. Death from AIDS rose steadily and monotonically through the mid-90s and since then has declined steadily. Though people still die from AIDS, this still represents a success story in health policy and science. For those experiencing the personal tragedy of AIDS, this is salvation.
So why did it happen? Well, first, the cause of the disease was correctly identified—the HIV virus—in the mid-80s; and second, by the mid-90s highly active anti-retroviral therapy, or HAART therapy, was able to effectively treat the virus and prevent progression to AIDS.
Again, two things happened: the cause of the disease was correctly identified, and an effective treatment was developed by an enlightened healthcare profession.
This is what success looks like. Now, let’s compare this story to that of obesity and diabetes.
Do we have this situation under control? The case study of “failure”
Let’s take a look at this figure. It shows the prevalence of diabetes in the United States over the last hundred-plus years. (Thanks to Gary Taubes who dug up these stats while researching his upcoming book.)
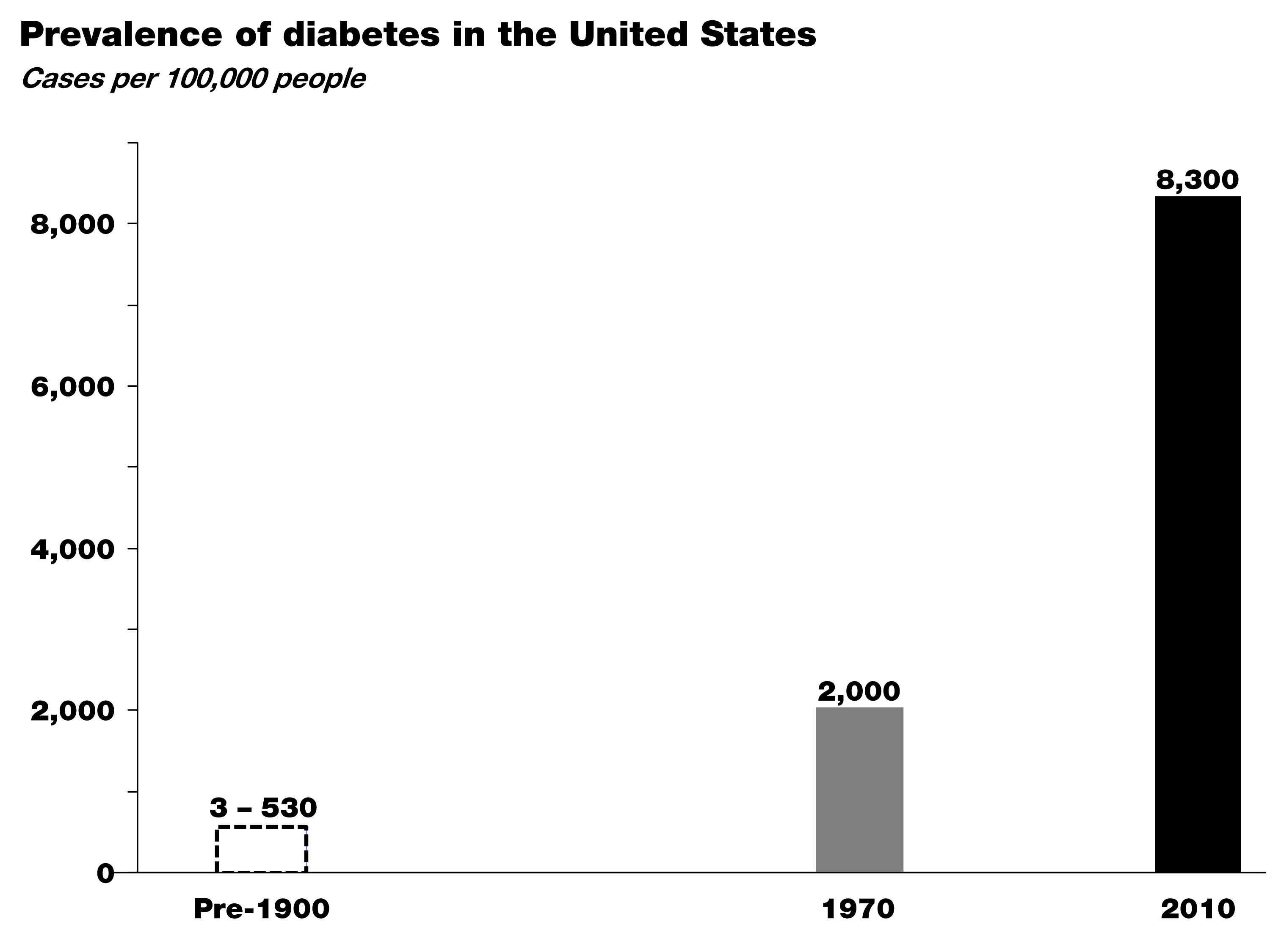
In the early 1900s the leading figures in medicine, Sir William Osler at Johns Hopkins and Elliot Joslin at Mass General, did exhaustive analyses of the number of patients with diabetes based on hospital records and census data. As you can see, diabetes was exceedingly rare in the 19th century—somewhere between about 3 and 500 cases per 100,000, depending on the analysis.
By 1970, around the time I was born, that number was up to 2,000 cases per 100,000, and between 1970 and today—at a growth rate of nearly 4% per year—that number has risen to more than 8,000 cases of diabetes per 100,000.
Worse yet, type 2 diabetes is now spreading into demographics previously naïve to the disease, particularly children. I don’t think any of us in this room today would argue that we have this situation under control. So where are we failing? Many of you understand the world of business. If this were a business, we’d be asking a lot of questions at this point, or we would be out of business. Like any business, we have two possibilities. We either look at our business plan (the basic premise for how we’re going to succeed) or the implementation of that plan (the way we operate on a day-to-day basis). When confronted with a runaway epidemic like this, we have to address the same two basic issues:
Either we understand the underlying cause of this disease and we have a good plan in place, but few individuals have the willpower or wherewithal to avoid the disease—whatever it is…In other words we’re not executing the plan.
Or, we don’t understand the disease in the first place and we’re giving the wrong advice. In other words, we don’t have the right business plan.
In this latter scenario, the failure is not one of personal responsibility, but of our assumptions about the cause of this disease. And these two scenarios have very different implications.
I am not certain which of these is more likely correct, but I do know the risk of ignoring the latter in favor of the former is not a choice we can make any more as a society.
So, maybe the question we should be asking is whether we are right about the environmental triggers of this disease—the underlying cause. Is it as simple as gluttony and sloth and a food industry that overwhelms us with highly-palatable, energy-dense foods, or is there something specific about the quality of the food we’re consuming that triggers these disorders? If we don’t answer this question about what is it in our environment that’s causing this disease correctly, just like we were able to answer it in the mid-80s with HIV’s role in AIDS, we can’t effectively treat the disease. Instead we’re stuck putting on Band-Aids.
Here’s another way to think about it: imagine this panel was on a new crisis in aviation. Planes are constantly crashing—falling out of the sky—and killing 4,000 people a day (just like obesity-related diseases are killing 4,000 Americans a day.) And you’re a pilot and you tell me that surely we understand the principles of flight. Right. Sure, we might suspect user error to be part of the problem. (Maybe the pilots aren’t flapping the wings hard enough!) But, maybe a better idea would be to go back to the drawing board to make sure we really understood this whole aerodynamics thing and we didn’t miss something important?
That’s how we think we have to look at this problem: 4,000 people in this country are effectively falling out of the sky every single day—dying—and we’re saying we’ve got it all figured out, and people just need to adhere better to our advice. I’m not confident that that’s the solution. Nor should you be.
Is there a policy-based solution to this problem?
Surely policy changes will play a necessary role in restoring our health. But it may be less about ‘how?’ and more about ‘when?’ I’d like to refer to this slide showing per capita cigarette consumption in the U.S. from 1900 until today—the number of cigarettes consumed is shown in grey with death rate from lung cancer superimposed in red.
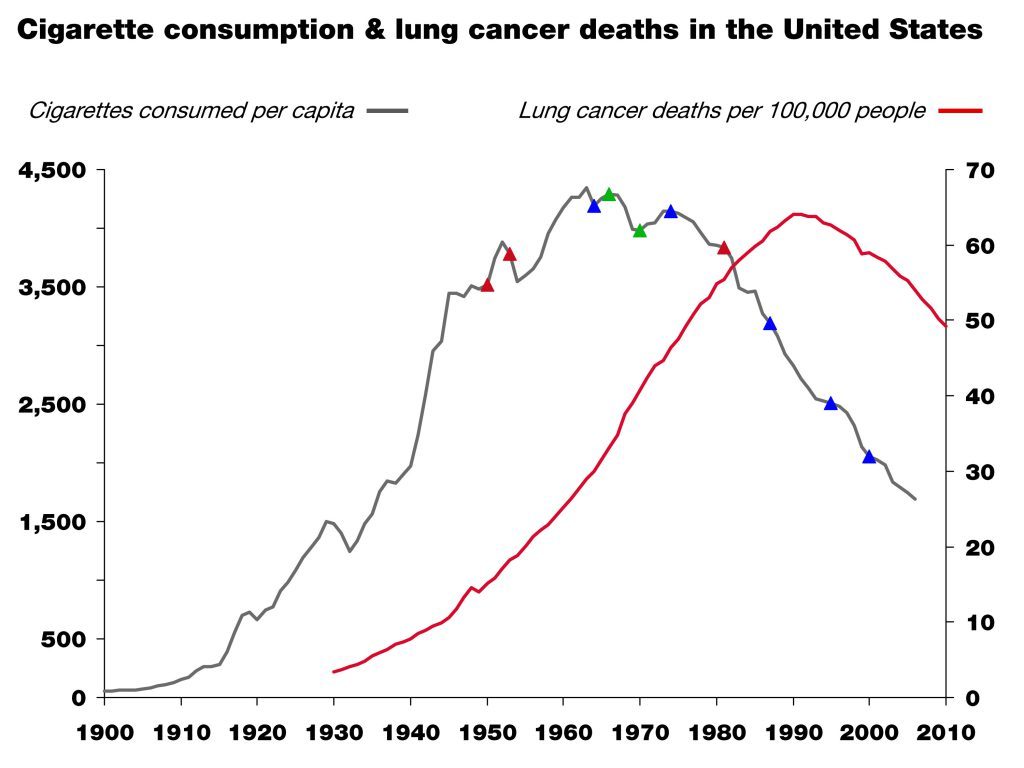
This is another success story. People in this room contributed to that success. The little colored triangles on the grey line are major milestones in science (red), market forces (green), and policy (blue). This is a great example of what one might call the “critical confluence”—scientific elucidation, policy action, market response, and behavioral shift—all coming together to save lives.
But, as in all things in life, algebra included, the order of events matters!
Which came first then? In the case of smoking and lung cancer, it was unambiguous scientific clarity, which in this case happened in the 1940s and 50s and resulted in the 1964 Surgeon General’s report. This information was absolutely necessary to drive the policy action, the market response, and the behavioral shift that followed. Without the knowledge that lung cancer is caused by smoking, no amount of policy or market response would have led to the necessary behavioral shift and so a meaningful reduction in lung cancer incidence.
When we consider the current situation with obesity and diabetes, we may still be missing the equivalent of the scientific clarity linking unambiguously the environmental trigger (smoking) that provided the obvious method of prevention (smoking cessation). And, again, if we think we do have that information, we have to ask why we’ve thus far failed to meaningfully prevent and successfully impact these disorders.
If the death rate from AIDS was still skyrocketing, I think we’d all agree we would either call into question our faith in HAART, or even the premise that HIV causes AIDS, if not both. Yet, in the face of skyrocketing obesity and diabetes, we play the who’s-on-first game all day long pointing fingers at people and industry.
Until we clearly identify the dietary triggers of obesity and diabetes, policies to shift behavior may be misguided and premature, despite their best intentions. Despite our best intentions.
I’m arguing that the policies so far may have been just that. Premature. And based on incomplete or faulty information. In other words, we may have the wrong business plan, but we blame our execution of the plan on our failure.
Parting shot
Today, we’re talking about a problem that touches, directly or indirectly, every single person in this room. It’s a topic that can be confusing and at times polarizing. We can’t lose sight of the big picture, which is easy to do when we just look at this problem through the lens of personal responsibility or will power. Remember, I used to think that “If people just learned to eat ‘right,’ (whatever that is), exercise and control themselves and their diet, everyone would be fine.” Today I reject that logic and the hubris that fostered it.
In the business world we know that the wrong strategy, no matter how well implemented, gives us little chance of success. Similarly, the right strategy, if poorly executed, often fails. What we need is the right strategy first and then the right execution second. At the moment, it’s hard to argue that we’re not failing with at least one of these two tasks. The question is which one.
Much of the discussion around this topic focuses on the execution; little attention is paid to the strategy or underlying insights that form the basis of the intervention.
Just 40 years ago the prevalence of obesity in this country was about one-third of what it is today, and that of diabetes about one-fifth. Is this all because Americans have become too gluttonous and slothful and the food industry figured out how to make food cheap and addictive enough? That they simply are too lazy and stubborn to do what we’ve been telling them to do—eat a little less, exercise a little more—for fifty years. Maybe. And I trust many good minds are already working on solutions to address that hypothesis.
However, what if the problem isn’t about non-compliance but about the nature of the advice we’re passing along. Maybe it’s our failure in that we have a simple idea about what causes these diseases, and like many simple ideas—paraphrasing Mencken here—it just happens to be wrong. It’s hard to fathom that two out of three Americans are simply too lazy to be active and too stubborn to eat healthy, despite losing their lives and their loved ones to the negative sequelae of these diseases. I find that hard to believe.
So, what if the problem is that our dietary advice is wrong in the first place? And incorrect dietary advice has resulted in an eating environment where the default for most people is a diet that causes obesity and diabetes?
If HIV or lung cancer were still spiraling out of control—as they were thirty and fifty years ago before the causes were unambiguously identified—the great minds in this country and the world would be leading investigative teams of scientists to figure out what we may have missed in our understanding of the cause of these diseases. We would not be complacent, perhaps because it would be harder to blame these diseases on the victims and their lack of will power. When we fail completely to prevent two devastating disorders for half a century, isn’t it time to investigate what we might have missed—what is it about these disease states that we do not understand? If nothing else, shouldn’t we hedge against the possibility—however slim you think the odds are—that we’re not as smart as we think we are. Those of us who are here today because of our business acumen know the importance of hedges in business. Isn’t it time we did that with obesity and diabetes?

Photo by PICSELI on Unsplash



Great post Peter. Indeed, the advice to, “Eat right and exercise” plus the one that really gets me, “Everything in moderation” is clearly not working. I admit to viewing the overweight / obese in our society as lazy over-eaters, having the deadly sins of gluttony and sloth, plus a dash of stupidity to have gotten in to that situation in the first place. Now I find myself much more compassionate. Not to say there’s no personal responsibility in the matter, but I certainly accept the notion that people are being misled, remain confused and feel lost as to how to solve the problems they are facing with their failing health.
Peter, I also watched the whole panel discussion. I thought that you were quite clear when delivering your message (great job!), but that the other panel members just didn’t want to hear or understand it. You clearly explained the scientific process; the other panel members just vamped on “we know ever so much.” A strong dose of Karl Popper would benefit some of these folks!
You felt my pain, Mark…
I’m thinking more Kuhn and Planck.
“…a new scientific truth does not triumph by convincing its opponents and making them see the light, but rather because its opponents eventually die, and a new generation grows up that is familiar with it.”
Haven’t seen the discussion yet. Sort of thinking about it, am not even sure if it is worth it. From the comments so far it appears there is a wealth of cognitive dissonance and some eminence based information. Not to say that your time was wasted. It never is when you spend time defending what should be so obvious by now.
I fully agree with you that we have to get at the science behind it. I am getting a bit tired of yet another observational, an other large cohort, controlled for all sorts confounders, or not, because half the time we don’t even know what the confounders are . It is one of the reasons I always enjoy Art Ayers’ posts. And now with the recent research coming out of Sweden about the possible negative impact of antioxidants, because we don’t even know to what extent we are upsetting the delicate balance in the production of ROS where our system is probably more than adequately equipped to intervene when and where needed.
I think I mentioned it before, I came to this not completely unlike so many here, except in my case it was a couple of angina attacks and subsequent verdict , arteries clogged, need double by-pass and statins for life. I did none but started my own research because obviously something was wrong with what we had been doing, eating even though we had both followed the nutritional advice from the experts. Actually my wife is a graduate in Health and Nutrition from Wageningen University. And thus we discovered the ‘alternate universe’. Malcolm Kendrick, Gary Taubes, and of course “there are no safe starches” Ron Rosedale, etc. etc. Which basically set us on a more primal path.
Never went back to my cardiologist, never used a statin in my life and BP went down from 150-160 / 100 to 135/87. I am 72, stand 6 tall (small) and weigh 65kg. No matter how much fat, or how many eggs I eat, I seem not to be able to gain any weight.
Thanks for the clear and for everybody understandable information. Always enjoy the e-mail notification come
Keep it up Peter, NuSi is desperately needed.
Dr. Attia,
I look forward to new content here as it’s a wealth of information, but I do fear the answer is that it depends; it’s the chicken or egg argument. Is this a cause or side effect or both? What are lacking are large unbiased double blind studies. We need studies that are performed without an agenda, The USDA provides us nutritional guide lines, they are interested in protecting/promoting agriculture, not that they are being malicious, but it isn’t helping the population. To paraphrase you, the idea that the business plan is wrong or the implementation of said plan is wrong is a fair assessment, we have the numbers and what we are doing isn’t working, the problem is increasing.
I just feel that without a ground up look at this we have far too many policy makers or experts stuck in a mode of stagnation, They are misinterpreting data or ignorant to new data or ideas that contradict their beliefs.
Now the “why” the statement a calorie is a calorie is true, but not all calories are processed in the same way. The human body processes a calorie or carbohydrate, protein and fat all differently, why don’t we start from there. The identification and solution from this point is going to be rough, there a decades of bad info and poor responses to address the bad info.
Dr. Attia, this is an excellent site. Thank you for maintaining it.
I really enjoyed this post. I find that in my late middle age I don’t want or need a “magic” solution, but want to see good science (not funded by those with an agenda or bottom line) so people have good information. As one who tried to live by the AHA and USDA guidelines, only to get heavier every year, I know what people lack is reliable information they dan trust. I am so glad I stumbled on to Atkins, Taubes, and you, which finally allowed me to get control and avoid diabetes which I was clearly headed for. I have nothing but sympathy for people who are obese, for they in the main don’t understand what’s taken control of their bodies. If I hadn’t found out about the power of carbs I would be there myself.
Hi Peter,
I am Tom Bilyeu’s assistant and he wanted me to find your Reversing the Smoking Trend Graph so that I can get the important moments from it, however I cannot find it online. He let me know that you showed it to him personally. Is there any way that you can send me an email with the graph?
Best,
S. White
As usual great post Peter! I don’t think there can be any better way of highlighting the problem as you did by using business model and the airplane analogy. I would quote the great poet Dr Iqbal here: “Although my group has idols up their sleeves, my job is to keep calling towards truth.”
High blood pressure was quoted as leading cause of death, I wish they knew how effective low carb is for high blood pressure. Good to hear from Ornish in his concluding remarks, …”a diet low in refined carbs…” I was expecting him to say low in fat.
Peter, I thought it was interesting in the panel discussion how Ms. Goldman failed to grasp the point you made with regard to the lack of emphasis being placed on determining the true causes of obesity in the face of the obesity-related death toll in comparison to what resources would be spent if that same death toll were the result of airplane crashes.
I made the following observation over at Art DeVany’s blog years ago: Saying that expending more calories than you ingest is the key to controlling obesity is sort of like saying that gravity causes airplane crashes — true, but it doesn’t tell you much.
Tom, glad you noticed this. I was worried I did too lousy a job explaining the analogy (which I may have). I like your gravity one, also.
I have nothing of substance to add, just want to say I’m new to your site and feel like I’ve just discovered a veritable gold mine in terms of what the future of nutrition is going to look like.
All too rare these days to find someone who practices the scientific method with absolute purity, if I had a complaint it is that you don’t write often enough.
Mark in Canada
Thanks, Mark. Not sure I can do much on the writing frequency problem, though.
How you must have suffered. Was it billed as a debate? The rest of the Milken panelists, made up of industry, academic, governmental and medical establishment types, were there to pontificate the current paradigm: eat-less and burn-more. As you rightly pointed out in your slide, the reason the anti-tobacco public policy reduced incidences of cancer is because tobacco causes cancer. The SAD pyramid diet promoted by the establishment in last 40 years got us an epidemic of obesity. Their fix is to hand them more of our tax dollars money and let them pile on more governmental regulations ( all buildings designed w/ Goldman staircase) and social coercions, ala the cigarette model.
Bad ideas beget awful results. People died. Instead of seeing the flaw and resulting damage their policies have wrought, perhaps due to cognitive dissonance, they double down w/ more of the same policies.
I sensed your reticence to declare the fallacy of the SAD paradigm, because you didn’t want to offend the esteemed (credentialized w/ gazillion degrees) panelists. You can’t afford to burn potential funders at confabs. Sensibly, you held back, sounded agnostic and played nice as the pompous Ornish’s kept bloviating about his clinical trials, arterial slides and snarking at Dr. Atkin’s hypothesis.
You are one calm hombre!
P, you’re kind in your praise. It wan’t billed as a debate, but as you can see, these things are sometimes set up as such.
Well done, but your argument lost strength with me when you used the analogy of 4000 people falling from the sky daily to create the sense of urgency in recognizing 4000 obesity-related daily deaths in the US. I instantly thought, “How many people are alive today in US and how many people fly daily? Those can’t be the same numbers. The answers: 318,253,000 alive in US today (rounded off) and, using a 2010 figure, 6,575,343 persons fly per day. If 4000 people die in US per day, that means .00126% of our population dies each day from obesity-related causes; .00126% of 6,575,343 (the number of people flying daily) equals 83.
Eighty-three people falling from the sky daily is a more accurate proportion in creating your intended comparison. Still absolutely alarming.
As for my personal experience of weight and health, I lucked into the Specific Carbohydrate Diet eight years ago (Paleo-like, but with the addition on non-liquid dairy and homemade yogurt; based on monosacharrides vs di- and poly-) due to deteriorating health after ten years of ulcerative colitis. More and more meds, yet getting sicker and sicker. It definitely takes will power to resist all the ‘yummy’ food around me, but luckily I feel the literal pain of poor choices within a couple of days if not hours, so it’s easy to re-set my course and be, for the most part, incredibly healthy. I think choices are most often based on motivation and I lucked into a condition that grabs me and throws me on the toilet in a ball of pain in short order if I don’t make the right choices. My weight is great, I exercise and am strong as a horse, and all my numbers are stellar. I am extremely active. But making the right choices has taken me years (I didn’t want to believe that my diet had to be that ‘restrictive’) and I still stumble despite my motivation and exposure to a wide range of information. I don’t even know where to start when speaking to my 85-year-old mother about nutrition. It’s as though she hasn’t read anything about nutrition since 1993, still believing that fat makes people fat and that rice cakes count as breakfast. So, yes, people are confused as to what to eat, but I also know that it’s pretty clear that cake and ice cream is not what you should eat if you want to lose weight and yet my friends do exactly that. To me it seems more like we are all battling addictions more than anything else.
I was going for a simpler message, but I actually like your analysis more. May I modify it and use it next time I make this case?
Peter – But, of course. Nice of you to ask.
Peter-
I listened to your panel discussion you posted.
I am just so stinking proud of you! The female who disagreed with you was off base
But oh well- you handled yourself well! I am always
Encouraged by you! Incidentally, we had a ‘biggest loser’
Competition at wrk- I ate mostly ketogenic and won the competition.
Always inspired by you! Thank you.
Yup, she sort of missed the point…
Nina Teicholz apparently does a good job of telling a story. It was so good I read it twice. Things were bad, but I did not realize how bad. Basically, the business plan has been very questionable, but investments have been made, careers made, and reputations established based on a particular dogma.
The food industry responded, and people basically eat what is offered in the local supermarket. Most of what is sold is low fat, no fat, high carb. If you have to ask the dairy guy to go search in the back for a plain, full fat yogurt that has not been injected with jam, you don’t need to do a study to find out what most people are eating. It is in plain sight, and you have to make a real effort to do something else. In fact, you probably have to violate what your doctor is telling you to do.
Unfortunately, most people who can’t tolerate what is presented as healthy in their local supermarket, and blame themselves for not jogging enough everyday, or suffer severe calorie restriction are just going to get worse. The situation is so bad in the research community I don’t expect things to change until they just die off.
Ditto on the difficulty at times of finding plain full fat yogurt!
I am in the process of reading Nina’s book Big Fat Surprise. It’s a must read which I’m sure as probably been mentioned elsewhere here. I’m at the part about Crisco and how it came to the forefront. It got me to thinking that I became a Crisco/margarine kid with lean steak and skim milk and so forth. Makes me wonder if my weight use has been compounded by these items I ate as a kid.
What a panel to have been on. You actually had one of the better credentials, Peter You actually worked on yourself. You had health issues and you tackled them. One of the panel I don’t think has ever had weight issues and he tells us to eat plant based and do this or that. It makes me wonder if he actually has thought as critically about these issues as you have. .
Good Morning Peter, et al…
I’ve had the PLEASURE to peruse your site extensively over the past week and came across MANY a post that screamed for me to respond, but I’m just a ‘layman’ and needed time to put my words to paper without seeming like a total moron!
Firstly… I totally understand your passion. It seems though, that the harder you try to explain it, the more you are faced with resistance. As is with me. The harder I advocate this solution, the more I’m faced with ‘but what about this… and what about that.’
My story (if anyone cares)
I jumped on the LC bandwagon 6 or so years ago after seeing a doctor about being “sick and tired of feeling … SICK and TIRED” After a general blood work up, it was concluded that (not only was I overweight/obese… but borderline Anemic as well” Otherwise healthy and strong (and stubborn). Don’t visit him but maybe once a year but in this case I just KNEW something wasn’t right! Of course his advice… lose weight, eat more frequently. Yaaa…ok!! I’m a ‘starve’ all day except for “IV” of coffee,cream and sugar that I tote around…. then come home and graze until bedtime. OK.. I get it… eat more frequently to ‘fuel’ your body all day long. Start with oatmeal.. “it sticks with you all day” … Gave it a try… and over a period of 7 months and lost 62 lbs! (From 248 to 186) Yay me!! Eating ‘lower carbs’ definitely was PART of the solution….
Well… (trying to Cliff Note my post) managed to keep it off for 2 yrs and then, like many, LIFE just throws you a curve ball… and all went to hell. So.. in summation (is that even a word?) here I am today… back up at 220.6 as of last Tuesday (when my “$hit or get off the Pot” journey started once again) Down to 214 today! 🙂
SO… eating low carb.. nothing new to me! It works AND I know it!
Please don’t be offended when people ask you what you eat. We just want to make sure we are choosing the right ‘gasoline’ for the ‘tank’ (insert winky smiley face here) <—- More of a good vs bad foods education lesson. When I read it I took it as.. Oooohhh cheese…. ooohhhh butter… oooohhh… whipping cream. We know quantities and preference differ … we just are grasping at … well…. whatever roadmap that will inevitable guide us to our final destination. (cheesy, I know)
There is a question coming, I promise…
Ultimately… the bottom line (for me) is getting to the point of Ketosis. You mention that it could take up to 3 weeks to get there…. however I read another article yesterday that put it at '3-5' days? Is this possible?
The reason why I ask (and why I frantically dissected many an article re: Ketosis last night) is that I experienced many of the symptoms/side effects yesterday morning) Extreme cramping/sweating/nausea in the morning and an 'out of body' feeling for the rest of the day. A 'foggy haze' so to speak. Alert and absolutely able to work but just a feeling that I was looking at my world from the 'outside' Was this in fact a possible result of Ketosis? A 6.6 lb loss in 1 week totally exceeded my expectation… 'stoked' none the less… and realistically not expecting those numbers every week… I just really want to get to the point of being in Ketosis but I'm unclear if I'm already there or not.
I know you are followed by many informed and educated folks and know you are busy and 'have a life' (whaaaat?) so I'm happy to heed the advise or comments from any one of these fine folks. Have a SUPER day. And 'thank you' …. just 'thank you'
Hi Dr.:
Firstly, my extreme appreciation for your work, your passion, and your writing. Now, to piggy-back on Erika’s story/question, I am wondering what your current stance on a ketogenic diet is at the moment – that is to say, Richard Nikoley at Free the Animal has taken a turn away from low carb and away from ketosis as a result of his work with Tator Tot Tim and the mighty Resistant Starch/gut biome research. Thoughts? Thanks!
Hi Peter,
my first comment over here… Been around here for a while now and thought it was time to share my thoughts and tell you how much i learned through reading your well-thought-out posts here.
Your point of view seems so logical to me that it is hard to believe how our society is not able to implement the clear steps this implicates.
It seems like we´re blind to the difference between root causes and symptoms.
As a side note, your content always is enabling folks to form their own believes and hypotheses. I really like that.
Have a nice day!
Justin
Thanks very much, Justin.
All the Milken panelists, after prefacing that they remained open to new ideas on causes of obesity, rest of the time they focused on public policies for prevention and touted anti-tobacco as the perfect model to rid of obesity. As far they are concerned, root cause has long been settled. Simply hand over more power to these credentialized experts, the government(CDC director) , business(Caremark exec), academia (Dean Goldman), do-gooder (Milken) and medical(Ornish), to regulate and coerce the mass to eat-less, burn-more and de-stress ala Ornish. Like Galileo’s Inquisition for doubting geocentrism, your lone voice of skepticism never had a chance. Love your blog. Keep fighting!
Is there a chance?
IMHO, the scariest part of the panel discussion is not that most of the panel favors a plant-based, low-fat, calories-in,calories-out approach — it’s that they all seem to favor using public policy ( i.e. Government) to mandate and/or force their ideas onto everyone else, as if this matter has already been settled….
This has been done for forty years with disastrous results. It is not so much that there is a government nutrition policy, it is that the food manufacturers reverse engineer their foods based on the required labeling/policy. Additionally, product promotion, and even media careers have been made supporting that policy. The majority of what is presented to you in your local supermarket, or public media for that matter, has been a result of government food policy.
The really obscene aspect of all of this is that if you faithfully followed the policy and it made you sick, then you are treated as a slothful, glutton who failed to adhere to the party line. A common variation of this is the knee jerk reaction of ” you don’t get enough exercise and you play too many video games.”
I am probably not persuaded by the exercise argument simply because I am 67 years old, and anybody jogging in my inner city Detroit neighborhood would have probably been suspected of mental illness in 1955. When I tell people this the come back is that everybody worked out on the assembly line every day. Well, all those office workers didn’t
work out, and “beer” bellies were far more prevalent among the assembly line workers.
Up until the government nutritional/medical complex became afflicted with some kind of nutrition psychosis, and I am not using that term lightly, most people thought they got fat by eating too many sweets, or drinking too much beer. In fact, people thought meat was nutritious.
(First off, Gary has a new book on the way? That’s one big rock I must have been living under of late…)
Really thought-provoking insights here. The comparison to AIDS treatment is keen, as it illustrates the stakes and severity of the implications of the obesity and diabetes epidemics. As you pointed out, both strategy and implementation must be on point for any treatment to be effective. While Americans’ overall implementation of government-promoted nutritional standards has been fairly abysmal, I think it’s also safe to say that said standards and the current obesity treatment (“eat less fat and overall calories, exercise more!”) are equally abysmal. Whether those standards are causative of the implementation is up for debate, but seems likely. Either way, the situation warrants further study (by both the scientific community and individuals taking responsibility for their health) and stringent application of those treatments that have shown to be effective.
I’ve recently started moving forward with pursuing my dreams of working in medicine, and sites like yours make me all the more excited about what lies ahead – particularly the opportunities to use lifestyle interventions to improve quality of life and promote healing. So, as always, thanks for sharing.
Happy to provide even a small amount of excitement about what lies ahead.
Just happened to be reading about ghrelin, and came across researchers being hampered by buying into this exact mindset:
In 2009 “GOAT links dietary lipids with the endocrine control of energy balance” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2789701/ “we also find that activation of the GOAT- ghrelin system is triggered by a specific lipid-rich environment rather than by caloric deprivation. These observations suggest that the ghrelin/GOAT system informs the CNS [central nervous system] about availability, rather than absence, of calories”
Then picked up in a 2013 review “Peptides and Food Intake” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4005944/ “this mechanism [enzyme ghrelin O-acyl transferase] may act as a nutrient sensor by using absorbable fatty acids to signal to the brain that high caloric food is available”
This because they see that ghrelin remains high in presence of lipids, so must be eating lipids that causes high ghrelin. So maybe do the experiment and see if ghrelin remains high under all conditions instead of just saying it is so? Well someone did, and in ketosis ghrelin drops: 2013 “Ketosis and appetite-mediating nutrients and hormones after weight loss” https://www.ncbi.nlm.nih.gov/pubmed/23632752
Oops. Somehow that didn’t make it to the review. Vicious cycle of ignoring failure in real life application to creating failure in research which perpetuates the failure in real life application.