
A couple of weeks ago Tim Ferriss and I were having dinner and the topic of cancer came up. As some of you may know my background is in oncology, specifically in exploring immune-based therapies for cancer by exploiting the properties of regulator T-cells. But that was a long time ago. Like many of you, I expect, I’ve also been personally impacted by cancer having lost a friend to glioblastoma multiforme (GBM). I often describe GBM to people as one of the cancers that gives cancer a bad name. When I went to medical school I planned on becoming a pediatric oncologist, and though I ultimately chose to pursue surgical oncology, my interest in helping people with cancer never wavered.
Over dinner that night, Tim asked me if I could write – in about 1,000 words! – a post on cancer that would be interesting and digestible to a broad audience. “1,000 words?!,” I asked. “How about 30,000 words?,” I responded only half kidding. After explaining why I couldn’t possibly write such an abridged version, Tim talked me into it. And so, I plan to accept the challenge and hope to provide readers with such a post (it will be on Tim’s blog when I do so), hopefully in the next month or two.
For an introduction, however, I’d like take a step back and place this topic in a broader context. I don’t need to say much about cancer that you don’t already know. You probably know that about one in three Americans will develop cancer in their lifetime, and you probably know that about half of them will succumb to the disease. What you may not know, however, is that we have made virtually no progress in extending survival for patients with metastatic solid organ tumors since the “War on Cancer” was declared over 40 years ago. In other words, when a solid organ tumor (e.g., breast, colon, pancreatic) spreads to distant sites, the likelihood of surviving today is about what it was 40 years ago with rare exceptions. We may extend survival by a few months, but not long-term (i.e., overall) survival.
We screen better today for sure, but subtracting lead-time bias, it’s not clear this extends overall survival. We’ve had success in treating and even curing hematologic cancers (e.g., some forms of leukemia and lymphoma). Certainly testicular cancer patients (especially seminomatous) are better off today and those with GI stromal tumors (GIST), too. Surgical control of cancer is much better today and some local treatments (e.g., specific radiation), too. But for the most part, when a patient has metastatic cancer today, the likelihood of living 10 more years is virtually unchanged from 40 years ago.
About a year ago, I was asked to give a talk about metabolic disease to a group of physicians. But before I spoke, a very astute and soft-spoken oncologist, Dr. Gary Abrass, gave the following introduction as a way to frame the context of my talk. After all, I’m sure many in the audience were wondering what could a discussion of insulin resistance have to do with cancer. I have thought often of his words that night in the many months since he so eloquently and informally introduced me.
I asked Dr. Abrass if I could have a copy of his talk and share it with you, to which he kindly agreed. Below is, nearly verbatim, the talk he delivered that night. (Dr. Abrass did give me the liberty of tweaking the text a bit, for emphasis and clarity.)
How have we fared in the War on Cancer?
On December 23, 1971, President Nixon declared war on cancer by signing the National Cancer Act. I was going to title this, “40 years in 4 minutes,” but I think this will take me a bit longer. At the time I was a third year medical student. Two years before, Neil Armstrong had inflated our national pride by setting foot on the moon, and there seemed no scientific goal unachievable. Activist Mary Lasker published a full-page advertisement in The New York Times: “Mr. Nixon: You Can Cure Cancer.” And she went on to quote Dr. Sidney Farber, Past President of the American Cancer Society and whose name now sits atop the Harvard Cancer Center, “We are so close to a cure for cancer. We lack only the will and the kind of money and comprehensive planning that went into putting a man on the moon.” Since then, the federal government has spent well over $105 billion on the effort.
Forty years later, Dr. Farber’s prophecy remains unfulfilled. In 2012 cancer killed an estimated 577,190 people in the United States. The death rate, adjusted for the size and age of the population, has decreased by only 5 percent since 1950. And most of this decline is due to mammography screening in breast cancer and cessation of smoking, resulting in less lung cancer in men.
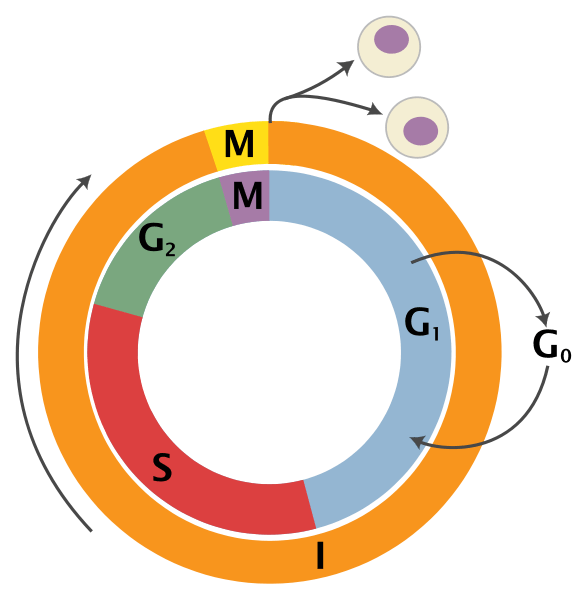
We have however developed a greater understanding of the biological and molecular basis of cancer. When I was a medical student, this graphic summarized what we knew about the growth cycle of the cancer cell.
The next graphic demonstrates what we have learned, a truly overwhelming accomplishment, a dizzying array of interconnecting signaling “pathways,” and spawned a whole new field, “translational medicine.”
![]()
With the completion of the Human Genome Project, new sequencing technologies have also opened up the prospect of personal genome sequencing as an important diagnostic tool. A major step toward that goal was the completion of the sequencing of the full genome, first on James D. Watson, one of the co-discoverers of the structure of DNA. In fact, Steve Jobs had personal genome sequencing. The price is down to $1,000 and Mayo Clinic Proceedings recently had an article raising the concern of direct to consumer advertising for genomic sequencing. We are now able to sequence gene by gene, pathway by pathway, the genetic code of some cancers. New “smart” drugs have been developed that target various mutations in these pathways. And currently there are over 800 “targeted agents” in clinical development. These drugs have been described by some investigators as “The Holy Grail,” but the clinical results suggest more of a commemorative cup for a “Happy Meal.”
While there is nothing unique about this paper, it is a good example of a typical negative trial targeting the IGF-1 receptor with a monoclonal antibody. The lack of response does not make us question the role of the IGF pathway as a prime driver of malignancy, but rather demonstrates the ability of the cancer to resist therapy. It seems there is so much redundancy in the system that the cancer finds alternate pathways. The cancer cell continues to defend itself, to bob-and-weave like the arcade game “Whack-a-Mole.”
So the investigators combined the IGF-1 monoclonal antibody with various other therapies: standard platinum based chemotherapy regimens, the “small molecule” tyrosine kinase inhibitor gefitinib (Iressa) targeting another common pathway (EGFR), and also the mTOR inhibitor temsirolimus (Torisel) which targets the IGF-1 pathway a bit further along. In any case, the point is, it still didn’t work. But why?
Investigators have mapped the genome of a typical lung cancer patient and found over 50,000 mutations. That’s a lot of targets! Granted they are not all ‘driver’ mutations, some are ‘passenger’ mutations. The patient whose genome was mapped was a 51-year-old man who’d reported smoking 25 cigarettes a day for 15 years. At 50,000 mutations, it works out to one mutation for every 2.7 cigarettes.
Last year the New England Journal of Medicine published a study by Gerlinger and colleagues. These investigators looked at intra-tumor heterogeneity. They performed a molecular dissection. They found diversity within the tumor itself. Each cancer is not cancer but, indeed, it is CANCERS. In other words “all cancers are rare cancers.” Let me repeat this point. Each tumor is a collection of heterogeneous – not homogenous – mutated cells. This article has engendered some discussion and some controversy. Many say that the results of the study bring the idea of personalized medicine to a halt, or at least dramatically slow it down. Are there exceptions? Yes, but they are rare. One example of an exception to this revelation is chronic myelogenous leukemia (CML), a cancer with a known single driver mutation.
In September 2011, biologist Dr. Alasdair MacKenzie of the University of Aberdeen, speaking at the British Science Festival in Bradford, explained that researchers trying to fully understand how our DNA causes disease might not be looking in all the right parts of the genome. The past decade of genetic studies has revealed that our 3.2-billion-long-DNA-letter code is more complex than anyone could have thought. More than 98% of the human genome does not encode protein sequences. It’s been referred to as “Junk DNA” and thought not to have a function, but maybe more correctly is that we do not know the function. He refers to this as the “dark matter” of the genome. And it’s thought that some of these “alternate pathways”, in which our resourceful cancer cell seeks refuge, may reside here. If this was not complicated enough, the new field of Epigenetics has grown exponentially resulting in a widening of the battlefield.
These are factors that can affect the expression of genes without causing mutations, turning switches on and off. In terms of cancer, much of this research has concentrated on what are called “Nononcogenic stress targets.” We can stress an organism in many ways: heat, poison, starvation, suffocation or more scientifically thermal, chemical, metabolic and oxidative stress. Organisms have an ingenious way of responding to such stress. In the 1960s an assistant in FM Ritossa’s lab accidentally boosted the incubation temperature of Drosophila (fruit flies), and when later examining the chromosomes, Ritossa found a “puffing pattern” that indicated the elevated gene transcription of an unknown protein.
This was later described as the “Heat Shock Response” and the proteins were termed the “Heat Shock Proteins.” This same HSP increases survival under a great many pathophysiological conditions. The HSP70s are an important part of the cell’s machinery for protein folding and help to protect cells from stress. While it enhances the organism’s survival and longevity under most circumstances, HSF1 has the opposite effect in supporting the lethal phenomenon of cancer. These proteins enhance the growth of cancer cells and protect tumors from treatments. This remarkable protein affords a protective response to other proteins in the cell, acting as a “chaperone” preventing them from mis-folding or “denaturing,” like when a boiled egg white turns opaque. These heat shock proteins are expressed at high levels in many tumor types: breast, endometrial, lung, prostate, even brain tumors. HSP overexpression signals a poor prognosis in terms of survival and response to therapy. HSP’s are now on the radar as a key target in the ongoing battle. This protein folding stress response is a hot topic in current cancer research. I have been communicating with Dr. Debu Tripathy who is currently studying epigenetic changes and protein folding stress responses associated with obesity. This protein folding stress response affords the cancer cell a survival advantage, and we share this protective mechanism with a fly, such a distant relative in our family tree, that one can only conclude that the cancer cell has hijacked this maneuver, this protective drive for immortality from the legacy of 100’s of millions of years of evolution…such a resourceful and formidable opponent.
In any case, when the Human Genome Project was near completion, President Clinton hosted a White House ceremony and announced that, “it will revolutionize the diagnosis, prevention and treatment of most, if not all, human diseases, and that humankind is on the verge of gaining immense new power to heal.”
The hubris of it all. It’s reminiscent of the quote of Sidney Farber. Hopefully this is not tempting fate. Theologians tell us the only unforgivable sin is pride. The increasing complexity of the science is affording us quite a dose of humility. British Physicist Brian Cox said that “being at the junction of the known and the unknown is a beautiful place to be for a scientist,” but it seems the more we know, the more we don’t know. Not unlike Winston Churchill’s characterization of Russia as “a riddle wrapped in a mystery inside an enigma.” Not unlike modern theoretical physics, one questions whether we are capable of understanding the complexity of the science. Hopefully it’s not like trying to teach my dog quantum theory. We are so smart, but it seems that the cancer cell is smarter. It bobs and weaves, slips our punches, and when we back it into a corner, it defends itself in remarkable ways borne of millions of years of evolutionary acumen much of it hidden in the dark matter of our genome.
Maybe we should call a truce in the War on Cancer and concentrate on prevention. Besides smoking, the most preventable cause of cancer seems to be obesity. It is generally thought that obesity may account for about a third of many cancer types, particularly breast, colon, uterus, kidney and esophagus. Obesity is a risk factor for type II diabetes and these patients are not only more likely to get cancer, but to have poor outcomes. Other speakers will explore the relationship of obesity and cancer, the epidemiology and the science, and see if this lends support to any practical prevention measures.
Gary Abrass, M.D.
April 19, 2012
Afterword
Just as the best way to get in shape is not to ever get out of shape, the best treatment for cancer is almost assuredly not to get cancer. And that’s clearly the theme of the introduction Dr. Abrass gave me. But I’m sure many of you are asking a more important question — what happens if I or someone I care about has cancer? If you can be patient with me, I do plan to address this, to the best of my understanding, in the coming months.

{kind=link}
{kind=link}
Fasting Glucose – Question
Background – Started LCHF in response to high CACS score >900 and other related metabolic syndrome symptoms.
My fasting glucose has slowly risen from ~ 4.5 and now remains stubbornly high (5.5-6.5) in spite of being LCHF for the past 3 yrs and a relatively active lifestyle (avg 1.5 hrs/day).
Fasting ketones have remained steady between 1.2-2.5.
Current BMI 26.5, target <25.
Would like to find a way to reset my avg blood glucose in the 4.5 range
Would like to lose the last stubborn 5kg around my midriff.
Any suggestions would be greatly appreciated. Thank you for your blog.
Any suggestions on how to break through this plateau and reset blood glucose levels would be appreciated.
Todd,
There is a fair amount of discussion on the blog Hyperlipid (https://high-fat-nutrition.blogspot.ca/ on the subject of fasting BG. There is reason to believe that the liver is generating some glucose to supply minimal requirements early morning. Glucogenisis amount varies with individual. It is not something to be concerned about, but please check it out. The discussion took place in 2008 somewhere so you will have to do some searching.
Peter
I had an operation for prostar cancer 1,5 yrs ago and am free from problems now. My Testosteron levels are still low. I am 72 more fit Than my age group. Hos does low carb or ketosis influence Testosteron ? Do you know or can you guess ?
I don’t know from a clinical trial standpoint, but in me I’ve experienced a 50% increase in free T and total T. I’ve also reduced my training volume, which be a greater driver.
Some random thoughts:
1. A couple of items in the Jul/Aug 2013 DISCOVER:
“Evolution in Overdrive” (p. 20) notes that in the past 10,000 years, world population has gone from about 5 million to more than 7 billion persons. This very fast, very recent population expansion has resulted in “millions of rare gene variants . . . gene variants that might make us more prone to illness, or simply less likely to survive.”
Maybe the introduction of agriculture didn’t encourage cancer by, as is often suggested, introducing “Neolithic” foods to which we aren’t adapted, but by providing abundant food that helped support a population explosion, an explosion that got us a bunch of new DNA mutations?
But according to “Cancer: The Long Shadow” (pp. 62ff), cancer was with us long before the introduction of agriculture. “. . . the fossil record reveals a disease that may have been with us since prehistoric times.” The author’s closing remarks: “Yet running beneath the surface there has been a core rate of cancer, the legacy of being multicellular creatures in an imperfect world. There is no compelling evidence that this baseline is much different now than it was in ancient times.”
2. According to Dr. Abrass, “. . . the most preventable cause of cancer seems to be obesity.” Has this been proven? I did an internet search for “does obesity cause cancer?” and saw the words “linked to” and “associate with.” Granted, I didn’t check all the results of the search, but “linked to” and “associated with” are not the came as “causes.” My hunch is that actually proving that obesity, in and of itself, causes cancer might be next to impossible.
3. Has mammography really saved that many lives? I can see where cessation of smoking can save lives, but from what I’ve read, mammography is perhaps not the life-saver it is promoted to be. The reality seems to be that a whole lot of women have to be scanned repeatedly for a whole lot of years to save one life. Meanwhile, all that screening can result in false positives, unnecessary full-out treatment of something that would never have been a problem, possible generation of new cancers from the extra radiation, and so on.
Marilyn, I agree with you hunches. Specifically, I doubt that obesity, per se, causes anything, let alone cancer, except in rare cases. And this includes T2D. But there is a strong association and underlying causative issues to both obesity and metabolic disease. Cancer is no exception. Additionally, I agree there is great controversy around the big 3 screening tools: mammo, PSA, and colonoscopy. At worst, there is no improvement in stage-adjusted survival, given lead time bias. At best, there may be a modest improvement. I suspect this is due to the same problem that plagues the statin trials — poor stratification of subjects and failure to identify a priori who is really at risk to warrant intervention.
Cancer screening is, to me depressingly parallel to low fat/low calorie ideology: an overwhelming push by medicine and government in the absence of any real data to support it. And virtually no honesty about this in the propaganda or the individual advice provided within the health care system. Same with flu shots and so much else.
With cancer screening, it’s not clear to me what such data could even be, e.g., what “data” can tell you how to weigh, say ten women losing their breasts, or a hundred women suffering lymphedema or suffering the effects of radiation or chemo, against, say, one woman possibly having her life extended? Unless screening tests become virtually 100% specific (unimaginable at present) or, as Peter suggests, the small number of truly high risk people can be identified some other way, with screening strictly limited to them, it will always be a personal judgment and different choices will be reasonable for different people.
With protocol-driven, guideline-based medicine strongly in ascendency, and doctors incentivized to follow them, there seems to be little prospect for such free, individual choices for some time to come. My own doctor has acknowledged to me that he is graded on how well people like me follow the guidelines and submit to colonoscopies, etc. Fortunately he’s a very good guy and supports my personal decision to opt out, happily trading off a tiny chance of benefit against a much greater chance of getting unnecessarily sucked into the medical mill and quite possibly being harmed in the process. Others might reasonably make different choices, though I think far fewer would if they knew how little evidence there is to suggest that the benefits outweigh the risks.
This response isn’t to Marilyn, but to Peter…can’t seem to find a link to leave a reply to his comment.
Just wanted to say THANK YOU, Peter, for this: “I doubt that obesity, per se, causes anything, let alone cancer, except in rare cases.” I’m so tired of obesity constantly being cited as the *cause* of all our society’s medical woes. It’s like you said in your TED talk, and like so many others in the low-carb/Paleo worlds have suggested: obesity is rarely, if ever the *cause* of chronic disease, but rather, it’s simply one more *effect* of fuel partitioning and overall metabolism gone awry due to our physiologically incongruent diets and lifestyles. I understand that adipose tissue can be considered an endocrine organ, so it’s obviously not completely benign, but for us, as a population, to keep laying the blame for everything from heart disease to rainy days on obesity just perpetuates the moral judgment of the obese as lazy, gluttonous, greedy people who sit on the couch all day with one hand in a bag of chips and the other on a bottle of Mountain Dew. It’s the easy way out, and, of course, dead wrong in most cases.
I couldn’t have said it better, Amy. Thank you.
Thank you for everything that you do! People like yourself, Gary Taubes and Robert Lustig are heros of mine who I believe have added 20 – 30 years to my expected lifespan! The book Good Calories, Bad Calories changed my life and your blog is constant reminder to help keep me on my new eating path!
I was at the mall today and a group of people were selling things like candy apples and cotton candy to raise money for breast cancer. I wanted to go up to them and explain that what they are selling is one of the main causes of the cancer that they are trying to cure. Its disheartening to think of all the money directed at the wrong research, but I think it is so wonderful that NUSI has been founded. Again THANK YOU for all the time you spend sharing this message with people like myself, who would be slowly killing ourselves day by day without having a clue! My life was changed several years ago and this is my first time ever writing a comment. If you or your colleagues ever feel discouraged that the message is not being accepted fast enough, remember there are tons of us out here who you have changed our lives and we have just been silently thankful! The government and associations will be the last to change their tune, but the individuals are starting to learn and understand! THANK YOU!
Thank you, Amanda, for your kind words. The tide will change not because of the Gary’s, or Rob’s, or Peter’s, but because of you and everyone else.
…………………
……………………..
……………………..
Carb Load Experiment
After eating 10 cups grapes – my glucose measured 225 – I thought about this a little bit and decided it was better to have a high – temporary – glucose reading than to secrete excess insulin to keep it lower – which I suppose my pancreas could easily have done if it wanted to
I suppose it knows what it is doing ?
It’s interesting to see that the ADA is starting to hedge it dietary bets a bit. Down here at the bottom of the world, our equivalent, Diabetes New Zealand still seems a bit confused. They say this: “•Carbohydrate: has the most direct impact on blood glucose levels and comes form both sugars and starches. Where possible sugar has been replaced or reduced.All dried fruit, juice, flour and other starchy foods (including potato, rice, flour and so forth) will have an effect on blood glucose levels so serving size counts” but then in their recipe section get quite carried away with recipes for muffins, hamburger buns and pasta etc. The best is their “special fruit cake” with ingredients as follows:
•1 kg mixed dried fruit
•1/2 cup boiling water
•1/2 cup orange juice
•1 cup nuts
•2 cups wholemeal flour
•2 tablespoons gluten flour or extra flour
•3 teaspoons baking powder
•3 eggs
•1/4 cup slivered almonds
•2 tablespoons sherry
Sorry, but it makes me feel ill! NZ is not far behind the USA in the T2D/IR/obesity stakes and sadly the unfortunate people who have to live with these conditions have little hope of getting the advice they need unless they strike out on their own. Thank God (seriously) for Gary Taubes, yourself Peter, AND Tim Ferris.
Oh, ad I’ll write to Tom Hanks if you won’t – do you know his address?
Dr. Attia – I just finished “Grain Brain” by David Perlmutter. What are are your thoughts about gluten vs, just the excess carbs (that is, living non-keto) as causative agent in the various degenerative diseases.
Thanks,
Scott
Not enough expertise to comment.
“Tim Ferris and I were having dinner” – Can I tell you how excited I was at the thought of you two collaborating? I’m not terribly familiar with Ferris’ work, but from what I have seen he seems to have incredibly effective (if unorthodox) methods, and I have a lot of respect for him.
On another note, this post was great and I look forward to reading more on your thoughts regarding cancer. I only just got my Bachelor’s in English, and nutrition is more of a hobby for me, so these posts always challenge me to learn more and do even more of my own research (and it makes me even more excited about the possibility of getting my graduate degree in a health-related field!).
Again, thank you…your site is a wonderful resource!
Thanks for you informative posts. Wonder if you can comment on Seyfried’s idea that the very models of 1) accumulated mutations causal in cancer and 2) metastasis, are questionable – supported, I believe, both by the heterogeneity of tumors and application of Occam’s razor (i.e. too complicated both with regard to random multiple mutations as well as multiple de-differentiation/re-differentiation of cancer cells required to posit that cancer cells seed other organs). Instead he interprets murine data to suggest that in fact there is a tipping point when the physiologic and metabolic loads over time cause energy systems (specifically mitochondrial respiration) to “go awry” globally and hence multiple cancers can arise, with numerous associated but not causal anomalies? I ask this in part out of theoretical interest, because of your background in immunologic, molecular research, and in part to wonder whether, if one entertained this hypothesis, it would be possible to avoid lymphadenectomies and extensive surgeries in favor of more conservative interventions (although as I type I’m already discounting the question as I recall that he does suggest modified macrophages travel and form distant niduses, perhaps giving some credence to the desireability of pruning the lymphatic system – yet seems dangerous to me nonetheless!).
Beyond that speculation, can you recommend any nutritionists with experience managing the restricted calorie ketogenic diet clinically for cancer, am needing some assistance with this and with diet cycling, as recommended by Seyfried – despite being low carb for almost 20 years since my first introduction to the concept by Barry Sears, I find myself with a diagnosis and am wanting to hit it hard with diet and needing some support. Thanks in advance and looking forward to more.
Teresa, these are great questions and I’m not sure I know the answers. But I’m all eyes/ears, for both personal and professional reasons. A dear friend’s wife is battling breast cancer and this very question (the nature of mets) is germane to her treatment choice. It’s a huge struggle for them, and I wish I could offer more insight. If you haven’t read it already (you probably have), you will appreciate “Emperor of all Maladies: The Biography of Cancer,” especially the chapter on Halsted and the radical mastectomy. You may be right re: the utility of aggressive lymphadenectomy.
Hi Teresa,
I know David Jocker https://www.drjockers.com/category/health-news/cancer/ believes in the treatment of cancer with a ketogenic diet. I’m not exactly sure how he runs his practice but its worth checking out.
All the best!
Teresa, My son is fighting a form of brain cancer and we’ve recently decided to put him on a ketogenic diet. We work with Carrie Loughran of Ketocare (www.ketocare.com). She is an RD and has decades of expertise in the diet for epilepsy and is now starting to work with a few cancer patients. You might also be interested in Miriam Kalamian. She’s not an RD but has an MS in nutrition science and worked with Seyfried on taking her son on a KD several years ago. So she has a lot of personal experience and now is a KD coach for cancer patients. She’s here: https://www.dietarytherapies.com and an interview with her just a couple days ago is here: https://www.thelivinlowcarbshow.com/shownotes/8826/738-miriam-kalamian-offers-hope-to-cancer-patients-with-the-ketogenic-diet/
I lost my first son at two years of age to GBM. After quickly coming to the same conclusion that you outline here (successful treatment means extending life by a few months), we chose to eschew aggressive treatments and worked instead on making our boy’s remaining days as enjoyable as possible. At first, that meant a trip Disney World and lots of trips to the petting zoo. At the end, that meant morphine at home in his own bed surrounded by those who loved him. For what its worth, those physicians who promised the least but could discuss the reality of the situation with unblinking candor remain in my highest esteem.
I look forward to reading your next post on this issue.
Mark, I don’t even possess the vocabulary to describe how sorry I am and how upsetting this is. I was, for reasons I don’t fully understand, drawn to pediatric oncology, even while in engineering school, and this eventually led to my decision to go to medical school, rather that engineering grad school. However, until I had a child of my own I don’t think I could even half understand what a parent like you goes through. I obviously still can’t.
Sometimes the people around me — wife, colleagues, friends — ask why I’m such a relentless freak in my work life. Why can’t we slow down, just a bit, they ask? I think one of the reasons to keep the pedal down all the way is the knowledge that every day we don’t have something to offer cancer patients based on an improved understanding of the disease is another day of this kind of sadness. And the same is true for all metabolic diseases.
Thank you for sharing your story. I hope one provider of healthcare is reading this and gleaning from it your wisdom.
Response to Peter. The stuff you are doing with Gary, Dr Lustig, the low carb community, etc., is really important. Even if the alternative hypotheses all turn out to be wrong, it’s clear that you (collectively) are adding critical thinking to the mix, i.e., you are improving the robustness of scientific debate (which it sorely needs). Keep at it. These efforts really do affect the well being of so many people.
Thanks very much, Paul.
dear Peter,
hope You might be interested in my resume of a popular explanation about some of my cancer research,
trying to use ordinary expressions,
those strange sicknesses sadly became an unnecessary violent public health issue,
¿ how can we understand the creation of cancerous cells ?,
out of several trillion body cells, every singular one is collaborating with a mutual benefit, for one and the same body,
(90% of those cell types are found all over the earths biomass),
our proper body cells, can achieve to ‘copy’ themselves as much as 80 times !,
just take your passport and make a copy, and a copy of this copy, and so on, eighty times, and if there wasn’t enough ink, (‘ genetic material ‘), you won’t be able to read the illegible name, nor the numbers,
and the related cells become confused about which body they are working for,
begin to struggle and to serve themselves,
and are therefore recognized as cancerous cells,
the ‘ink’, the material necessary to complete the copies, in real life, are the so called aminoacids, mostly supplied by natural vitamins, etcetera,
(and without putting any oil (ink) into an engine, normal performance, will become critical, very soon),
¿ by what means do our bodies get their essential building blocks ?,
(aminoacids and minerals, (oil for the engine, ink for the printer)),
to guarantee our organs can function correctly, assure our body can preform its normal tasks, maintain the ability to carry on, assembling genetic structures, proteins, digestive enzymes, hormones, (some natural vitamins), etcetera,
endless vital micro- and nano-processes must just happen fine, with a typical and sane outcome,
the majority of those aminoacids, are taken in by the means of natural vitamins, etcetera,
the existing 22 aminoacid molecules, (almost living structures), composed mainly by few hydrogens, nitrogen, oxygen and carbon atoms, which attract and repel themselves, in a steady dance, (awash in cosmic radiations),
several are essentially unstable to temperatures higher than 42° degrees celsius, (various of those needed by or bodies),
their balanced interatomic shake, is where life originates,
with vibrations comparable to the sound of a musician,
and a protein, for example, assembled with thousands of those molecules, creates the impression of an orchestre,
some, which due to their temperature responsiveness, start to stutter, with as little as 42° degrees celsius,
(while pasteurizing is 80° and cooking 100°),
often the reason, why those active fundamental building blocks can loose their vitality, and go numb,
with an awful problem emerging to many biological processes !,
¿ to what degree are our bodies building blocks, those vigorous aminoacids, animated ?,
¿ do they have ‘ gods divine breath of life ‘ ?,
which is so easily destroyed, unachievable to be restored, and even more hopeless, to be originated,
¿ are those molecules just melted down to passive, increasingly lifeless structures, due to excessive temperatures ?,
¿ are we ‘ homo ignis incendium ‘, the only mammal species using fire to ‘prepare’ food ?,
what so ever, we are taking about mayor implications, in case those vital, force giving, aminoacid molecules fall short,
cells can easily turn cancerous,
(with alzheimer, diabetes, etcetera, just on a brink),
but after thousand million years of trials and errors, biology creates the impression to have regulated this setback with 3 000 000 000 dendritic lymphocytes, (or probing cells, who search for those ‘disoriented’ cells), fundamental parte of our bodies immune systems, which break, those cells turned cancerous, to pieces and recycle their proteins,
with the only inconvenient, that those dendritic ‘fighter cells’, as well, need aminoacids, delivered by natural vitamins,
in resume, it simply may be of greatest importance to consume natural vitamins by means of minimum 20 to maximum 50% raw food, (fruits, salad, nuts, honey, etcetera, that never suffered temperature),
just to allow biological methods to assimilate enough essential building blocks,
that’s no news at all !,
on the other hand, ¿ how come that year after year we consume far less than twenty per cent, (in an average global scenario), using artificial, lifeless drugs and vitamins, on a regular base, instead ?,
clearly i’m oversimplifying biological phenomenons,
true to life, ‘miracles’, are everlasting more entangled and increasingly complex,
to give just one example,
amino acid containing substances, are not barely supplied by vitamins, but by proteins, (which themselves are built with those building blocks), etcétera,
misunderstandings are difficult to be avoided,
too many biological functions are partially unknown, or not radically comprehended, still,
but the twenty precursors, our bodies are based on, are fairly well understood,
half of which we have to take up with food, and others can be pieced together by our own mortal organs,
all those are essential upon fundamental mineral absorption, to so many metabolic processes, for some truly special nerve structures, neurotransmitters, even the entire non standard defense and immune system is shaped by them,
whatever you may imagine,
all backed by indispensable DNA molecules, planing those proteins and vitamins,
and as well made from those bioactive compositions, delivering marvels,
the obvious dissimilarity between natural bioactive and inert artificial vitamins and proteins,
could be pictured as a key that enters a door lock, turns the lock, opening the door,
while an artificial vitamin would exclusively be able to slide into the lock, but not to turn it,
consequently blocking the door in fault of a jammed lock,
rendering impossible normal biological procedures,
often shutting them down permanently,
cheers
milo
John U,
Thank you for your reply, I will spend some time exploring that website.
I have heard of glucogenisis but my impression was that elevated BG regardless of the source will trigger an insulin response. I have been endeavouring to modify my exercise and nutrition regime to minimize BG while maintaining a state of NK in order to eliminate arterial inflammation.
I have reduced protein consumption considerably and replaced the calories with fat. This has had a very positive effect on my blood pressure and seems to be slowly modifying my body composition, notwithstanding my current weight plateau. However, I am concerned about the potential long term effects of an elevated BG level as the principle reason for me embarking on this journey was my elevated CACS score and my strong preference to avoid statins, which was the prescribed course of action of my physician.
Once again, thank you for your response.
Hi Todd. I am no expert and in fact I am just slogging through all the info on nutrition and trying to follow along. I don’t know your history but I think that you are doing the right thing in following a high fat, LC diet . The blog to which I referred, Hyperlipid, is hosted by a man who eats about 80% saturated fat in his diet. Since the CAC score would reflect what has happened to your ateries over many years, I don’t believe that it would predict with any high degree of accuracy your outcome after you have modified you nutritional intake. From the reseach on CAC that I have seen, the evidence that CAC is a good predictor of CVD hinges on the subjects continuing for many years whatever they were doing in the past. What’s done is done, and maybe it cannot be reversed, but maybe some can after a diet change for the better, so I would not assign a high predictive ability to the cac score unless you know something more than I do.
I also would not take the statins. There is already so much written in books and blogs about the poor research that was done in support of their use, and the evidence of seriously harmful side effects. You have made a smart choice.
I’m a recent uterine cancer survivor. The contributing factors to my cancer were these: over 50, post-menopausal, nulliparous, and overweight. All of these factors interact in ways that are complex and likely highly specific to an individual. I hope to not have a recurrence, and am regaining my stamina to increase my activity levels, as exercise is also preventative, according to the data.
I wonder if the two instances in which I experienced sudden & dramatic weight loss — 40+ pounds in a matter of two months, had an impact on my developing cancer.
The context for these weight loss episodes, once due to depression following a sexual assault, and again after a nasty divorce, with subsequent weight gain plus, has meant that I metabolized a lot of fat very quickly. Since abdominal fat is estrogenic in women, did these sudden weight loss episodes dump a lot of estrogen in my system, causing my endometrium to grow beyond a healthy amount? Was the time I had a more gradual weight loss, one that has since reversed, a less metabolically impactful process, or did that fat metabolizing also release extra estrogen into my system?
The incredible levels of hatred directed particularly at women for being fat, or even larger that a size 6, is psychologically quite damaging, and well documented. I never want to diet again, yet I need to lose weight to maintain my cancer free status, after surgery & radiation. At age 58, have I so damaged my metabolic system by this weight roller coaster that I have no ability to lose and keep weight off?
When the AMA declared obesity a disease, a stance that I think will do more harm than good, I asked my Dr. how my HMO was planning to rend to this. I want a biweekly support group for emotional eating, help with stress management, and a PT who can coach me at a gym three times a week, all paid for by my insurance. I have three weight related diseases; osteoarthritis in my knees, sleep apnea, and cancer. Yet all my usual health indicators are good: blood pressure, cholesterol, blood sugar, stress heart test.
I am scared of a cancer recurrence or metastases, and I need medical support to help me correct a lifetime of emotional overeating & lack of exercise. I have not been able to do this myself, and work full time, manage a home, a marriage, raise kids, deal with aging parents, cope with not enough money, etc. It’s all just too damn much.
These are important questions, Rebecca, and I wish I knew the answers. Your last point really resonates and I’m sure others, too, will understand and relate to it. I look forward to the day when a community exists around support and sponsorship for helping us all get through these struggles.
On money & related, check out Mr Money Mustache, or some other financial independence blog. There’s probably a lot of things you’re spending money on that you’d be perfectly happy without.
Great stuff, Peter. The blog is awesome; this is the first time I’ve had a chance to comment. And I have to say that I’m super pumped about the thought of you and Tim Ferriss teaming up.
You guys are both high on my list of “people I’d like to work with someday”. And, yes, I actually have that list. 🙂
-mark
Ha ha, Mark. Last time Tim and I worked out together in SF a few people interrupted Tim to ask if he was Tim. He was very gracious and it was funny. I’m sure he gets it all the time.
Reporting age-adjusted mortality rates over all ages the way Dr. Abrissa does, when he claims that mortality “has decreased by only 5 percent since 1950”, tends to conceal greater relative reductions of mortality at younger ages, as noted by Kort 2009. We cannot know to what extent the younger birth cohorts also will experience lower cancer mortality at old age in the future: the great mortality reductions at very young ages are probably much due to specific treatment success in e.g. acute leukemia and testicular cancer, but this does not seem to explain the declining mortality among people in their 40s and 50s.
Hey Peter, I stumbled upon your talks on youtube in my own quest with a Keto diet and they were awesome. Thank you for yours, Gary’s and any others who are spreading these ideas that maybe we have got it all wrong, that maybe it is carbs that are killing us. I think the science is getting there and you guys are at the forefront of the battlefield in nutrition. That is a great thing to be apart of and much respect. Keep pushing and make sure your voices are heard as much and as loud as possible.
As for cancer, even Sloan Kettering is coming up with carbs are huge factor in cancer.
Watch the president of Sloan Kettering speak on it here. They are roughly the same type of presentation but I figured I would share both.
2010 – https://youtu.be/WUlE1VHGA40
2012 – https://youtu.be/PV3UnNvN3NI
Yes, Jared, many very influential oncologists, such as Craig Thompson (here) and Lew Cantley of Cornell are really beginning to view cancer as a metabolic disease, a view I obviously share.
A blood glucose question: If one has increased BG when on lo carb, higher fat, say 90-100 reading vs 70’s to 80’s when on a much higher carb diet and lower in fat, would this be indicative of someone who is insulin sensitive? Assume Trgs no more than 60 in both cases.
If one has lo Trgs 60 or less regardless of carb intake what does tt mean?
Thanks,
Steve
Addressed in previous post. Also see here: https://high-fat-nutrition.blogspot.com/2007/10/physiological-insulin-resistance.html
Why should anyone reserve judgement on Tim Ferriss? He has a public persona and his business is literally selling himself, his worldview, and his techniques. To suggested anyone should reserve judgement on him because we have not met him is silly. The problem with Tim Ferriss is not that he is a self-help guru or or that his business is self-promotion. The problem is that he does this from the perspective of a sociopath and unapologeticly promotes the schemer mentality. I would have thought someone of your caliber would give little credence to Mr. Farriss.
Peter,
I really enjoy your YouTube talks, you’re very well-spoken and fascinating to listen to.
I wanted to ask you if glycine will spike insulin and push me out of ketosis at doses of 15g with every meal (4 meals/day). I’m using it to treat negative symptoms of schizophrenia because it’s supposed to increase nmda receptor activity. I couldn’t find an answer online to this so I’m asking you since youre the expert on ketosis. Weight loss/health and treating negative symptoms are both high priorities of mine, but I can always switch to sarcosine if glycine does spike insulin.
Probably, since glycine is a gluconeogenic AA (AA are typically gluconeogenic or ketogenic). But give it a shot.
I’m a bit bemused by the fairly vitriolic reactions to Timothy Ferriss. of course I have never met him, but to describe him as a sociopath is bizarre. I have his first two books, and am currently reading his latest, “the 4 hour chef”. The latter is the most enjoyable cookbook I have ever read but it’s a lot more than a cookbook. Based on my reading, he seems to be a truly independent thinker who is happy to share what he’s doing. For me, I would never have found the LCHF diet and ketosis if I hadn’t first read “the 4 hour body” so thank you Tim.
That guy’s comment was simply stunning and not even worthy of rebuke.