
I wrote this post at about the same time Germany won the World Cup in Rio de Janeiro in 2014. There’s been a lot of moving and shaking in the world of exogenous ketones since then, not to mention soccer. Looking back on my post, I still consider it relevant in terms of what exogenous ketones possibly can (and cannot) do for performance. In this case, to see if exogenous ketone esters provide me a “boost” by allowing me to do the same amount of work while expending less energy (and work at a relatively lower VO2) compared to no supplementation.
I’m getting an increasing number of questions about exogenous ketones. Are they good? Do they work for performance? Is there a dose-response curve? If I’m fasting, can I consume them without “breaking” the fast? Am I in ketosis if my liver isn’t producing ketones, but my BOHB is 1.5 mmol/L after ingesting ketones? Can they “ramp-up” ketogenesis? Are they a “smart drug?” What happens if someone has high levels of both glucose and ketones? Are some products better than others? Salts vs esters? BHB vs AcAc? Can taking exogenous ketones reduce endogenous production on a ketogenic diet? What’s the difference between racemic mixtures, D-form, and L-form? What’s your experience with MCTs and C8?
Caveat emptor: the following post doesn’t come close to answering most of these questions. I only document my experience with BHB salts (and a non-commercial version at that), but say little to nothing about my experience with BHB esters or AcAc esters. But it will provide you will some context and understanding about what exogenous ketones are, and what they might do for athletic performance. We’ll likely podcast about the questions and topics above and cover other aspects of exogenous ketones in more detail.
—P.A., June 2018
§
Original publication date: August 14, 2014
Last year I wrote a couple of posts on the nuances and complexities of ketosis, with an emphasis on nutritional ketosis (but some discussion of other states of ketosis—starvation ketosis and diabetic ketoacidosis, or DKA). To understand this post, you’ll want to at least be familiar with the ideas in those posts, which can be found here and here.
In the second of these posts I discuss the Delta G implications of the body using ketones (specifically, beta-hydroxybutyrate, or BHB, and acetoacetate, or AcAc) for ATP generation, instead of glucose and free fatty acid (FFA). At the time I wrote that post I was particularly (read: personally) interested in the Delta G arbitrage. Stated simply, per unit of carbon, utilization of BHB offers more ATP for the same amount of oxygen consumption (as corollary, generation of the same amount of ATP requires less oxygen consumption, when compared to glucose or FFA).
I also concluded that post by discussing the possibility of testing this (theoretical) idea in a real person, with the help of exogenous (i.e., synthetic) ketones. I have seen this effect in (unpublished) data in world class athletes not on a ketogenic diet who have supplemented with exogenous ketones (more on that, below). Case after case showed a small, but significant increase in sub-threshold performance (as an example, efforts longer than about 4 minutes all-out).
So I decided to find out for myself if ketones could, indeed, offer up the same amount of usable energy with less oxygen consumption. Some housekeeping issues before getting into it.
- This is a self-experiment, not real “data”—“N of 1” stuff is suggestive, but it prevents the use of nifty little things likes error bars and p-values. Please don’t over interpret these results. My reason for sharing this is to spark a discussion and hope that a more systematic and rigorous approach can be undertaken.
- All of the data I’ll present below were from an experiment I did with the help of Dominic D’Agostino and Pat Jak (who did the indirect calorimetry) in the summer of 2013. (I wrote this up immediately, but I’ve only got around to blogging about it now.) Dom is, far and away, the most knowledgeable person on the topic of exogenous ketones. Others have been at it longer, but none have the vast experiences with all possible modalities (i.e., esters versus salts, BHB versus AcAc) and the concurrent understanding of how nutritional ketosis works. If people call me keto-man (some do, as silly as it sounds), they should call Dom keto-king.
- I have tried the following preparations of exogenous ketones: BHB monoester, AcAc di-ester, BHB mineral salt (BHB combined with Na+, K+, and Ca2+). I have consumed these at different concentrations and in combination with different mixing agents, including MCT oil, pure caprylic acid (C8), branch-chained amino acids, and lemon juice (to lower the pH). I won’t go into the details of each, though, for the sake of time.
- The ketone esters are, hands-down, the worst tasting compounds I have ever put in my body. The world’s worst scotch tastes like spring water compared to these things. The first time I tried 50 mL of BHB monoester, I failed to mix it with anything (Dom warned me, but I was too eager to try them to actually read his instructions). Strategic error. It tasted as I imagine jet fuel would taste. I thought I was going to go blind. I didn’t stop gagging for 10 minutes. (I did this before an early morning bike ride, and I was gagging so loudly in the kitchen that I woke up my wife, who was still sleeping in our bedroom.) The taste of the AcAc di-ester is at least masked by the fact that Dom was able to put it into capsules. But they are still categorically horrible. The salts are definitely better, but despite experimenting with them for months, I was unable to consistently ingest them without experiencing GI side-effects; often I was fine, but enough times I was not, which left me concluding that I still needed to work out the kinks. From my discussions with others using the BHB salts, it seems I have a particularly sensitive GI system.
The hypothesis we sought out to test
A keto-adapted subject (who may already benefit from some Delta G arbitrage) will, under fixed work load, require less oxygen when ingesting exogenous ketones than when not.
Posed as a question: At a given rate of mechanical work, would the addition of exogenous ketones reduce a subject’s oxygen consumption?
The “experiment”
- A keto-adapted subject (me) completed two 20-minute test rides at approximately 60% of VO2 max on a load generator (CompuTrainer); such a device allows one to “fix” the work requirement by fixing the power demand to pedal the bike
- This fixed load was chosen to be 180 watts which resulted in approximately 3 L/min of VO2—minute ventilation of oxygen (this was an aerobic effort at a power output of approximately 60% of functional threshold power, FTP, which also corresponded to a minute ventilation of approximately 60% of VO2 max)
- Test set #1—done under conditions of mild nutritional ketosis, while still fasted
- Test set #2—60 minutes following ingestion of 15.6 g BHB mineral salt to produce instant “artificial ketosis,” which took place immediately following Test set #1
- Measurements taken included whole blood glucose and BHB (every 5 minutes); VO2 and VCO2 (every 15 seconds); HR (continuous); RQ is calculated as the ratio of VO2 and VCO2. In the video of this post I explain what VO2, VCO2, and RQ tell us about energy expenditure and substrate use—very quickly, RQ typically varies between about 0.7 and 1.0—the closer RQ is to 0.7, the more fat is being oxidized; the reverse is true as RQ approaches 1.0

Results
Test set #1 (control—mild nutritional ketosis)
The table below shows the data collected over the first 20 minute effort. The 20 minute effort was continuous, but for the purpose of presenting the data, I’ve shown the segmental values—end of segment for glucose and BHB; segment average for HR, minute ventilation (in mL per min), and RQ; and segment total for minute ventilation (in liters).
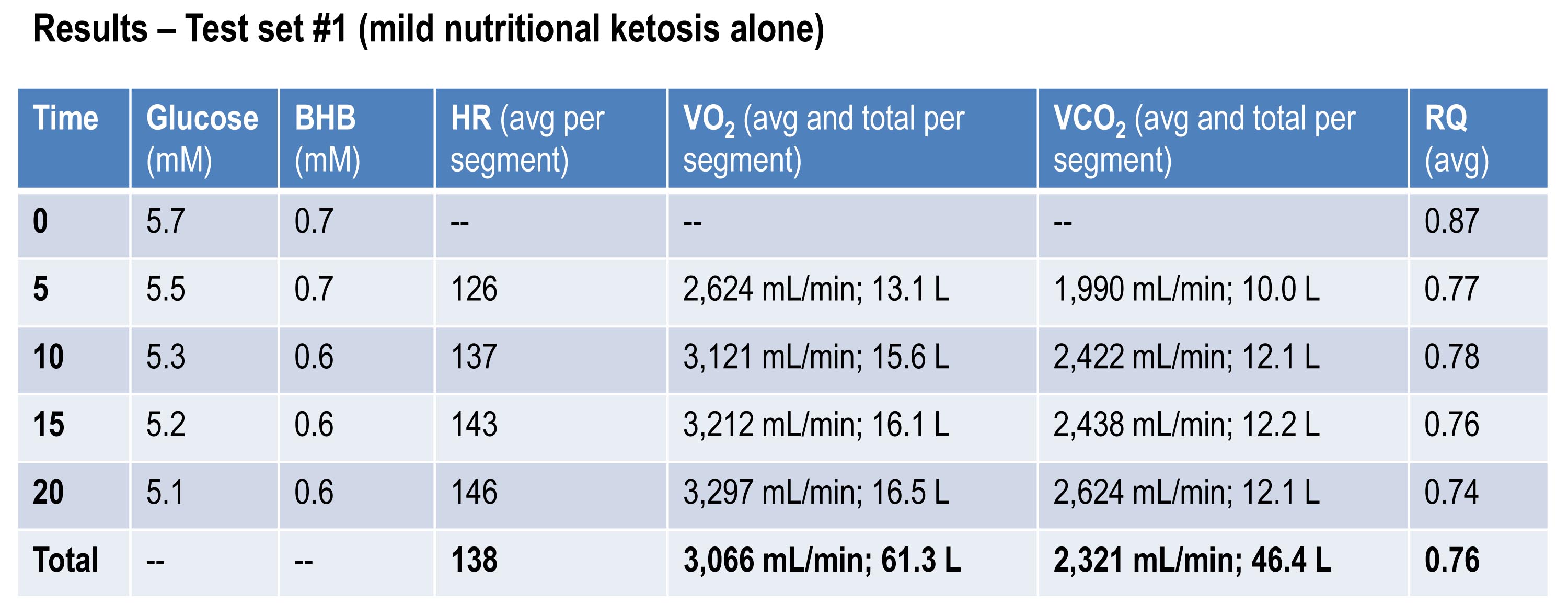
Glucose and BHB went down slightly throughout the effort and RQ fell, implying a high rate of fat oxidation. We can calculate fat oxidation from these data. Energy expenditure (EE), in kcal/min, can be derived from the VO2 and VCO2 data and the Weir equation. For this effort, EE was 14.66 kcal/min; RQ gives us a good representation of how much of the energy used during the exercise bout was derived from FFA vs. glucose—in this case about 87% FFA and 13% glucose. So fat oxidation was approximately 12.7 kcal/min or 1.41 g/min. It’s worth pointing out that “traditional” sports physiology preaches that fat oxidation peaks in a well-trained athlete at about 1 g/min. Clearly this is context limited (i.e., only true, if true at all, in athletes on high carb diets with high RQ). I’ve done several tests on myself to see how high I could push fat oxidation rate. So far my max is about 1.6 g/min. This suggests to me that very elite athletes (which I am not) who are highly fat adapted could approach 2 g/min of fat oxidation. Jeff Volek has done testing on elites and by personal communication he has recorded levels at 1.81 g/min. A very close friend of mine is contemplating a run at the 24 hour world record (cycling). I think it’s likely we’ll be able to get him to 2 g/min of fat oxidation on the correct diet.
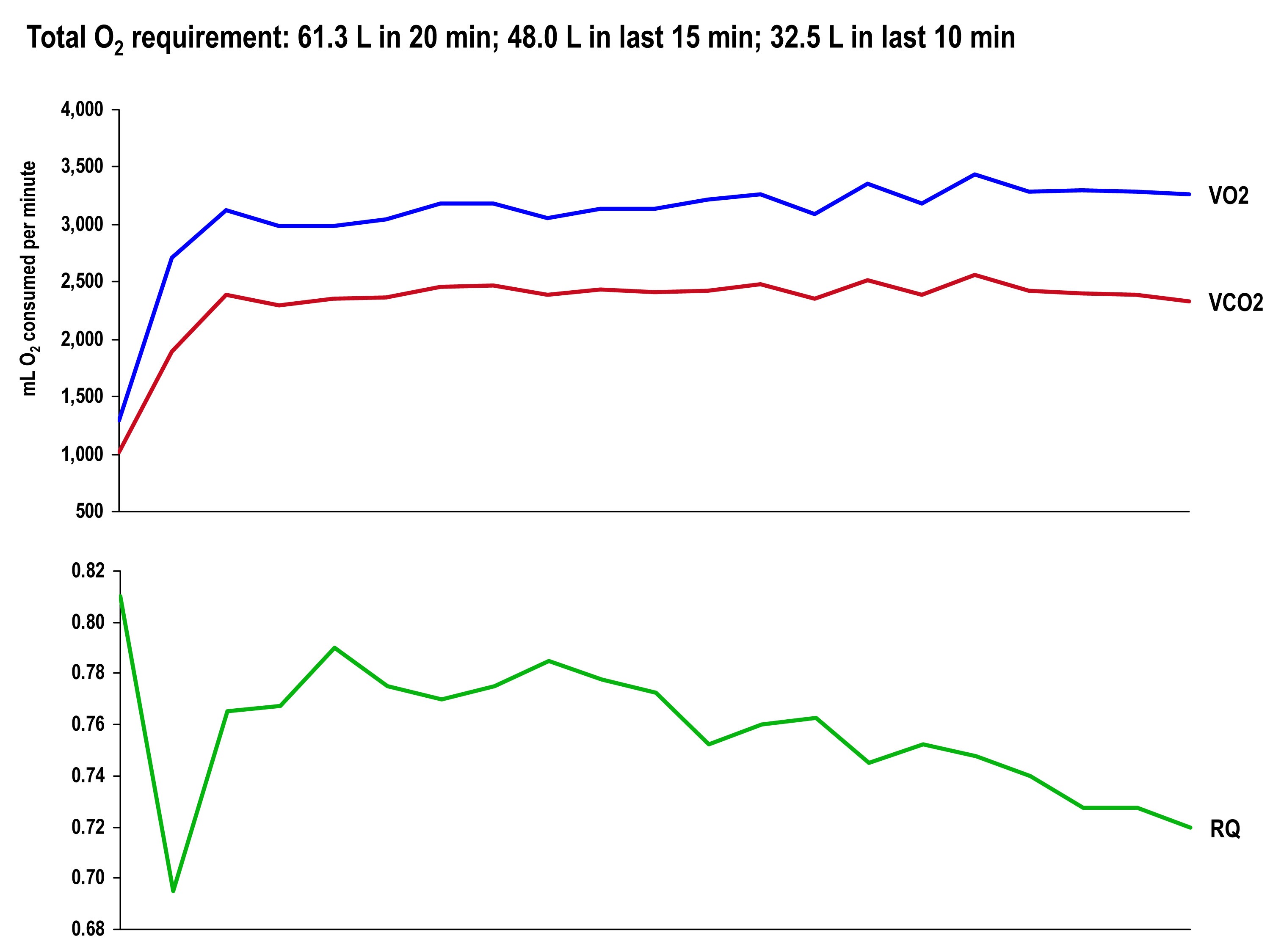
The graph, below, shows the continuous data for VO2, VCO2 (measured), and RQ (calculated).
Test set #2 (ingestion of 15.6 g BHB salt 60 minutes prior)
The table below shows the same measurements and calculations as the above table, but under the test conditions. You’ll note that BHB is higher at the start and falls more rapidly, as does glucose (for reasons I’ll explain below). HR data are almost identical to the control test, but VO2 and VCO2 are both lower. RQ, however, is slightly higher, implying that the reduction in oxygen consumption was greater than the reduction in carbon dioxide production.
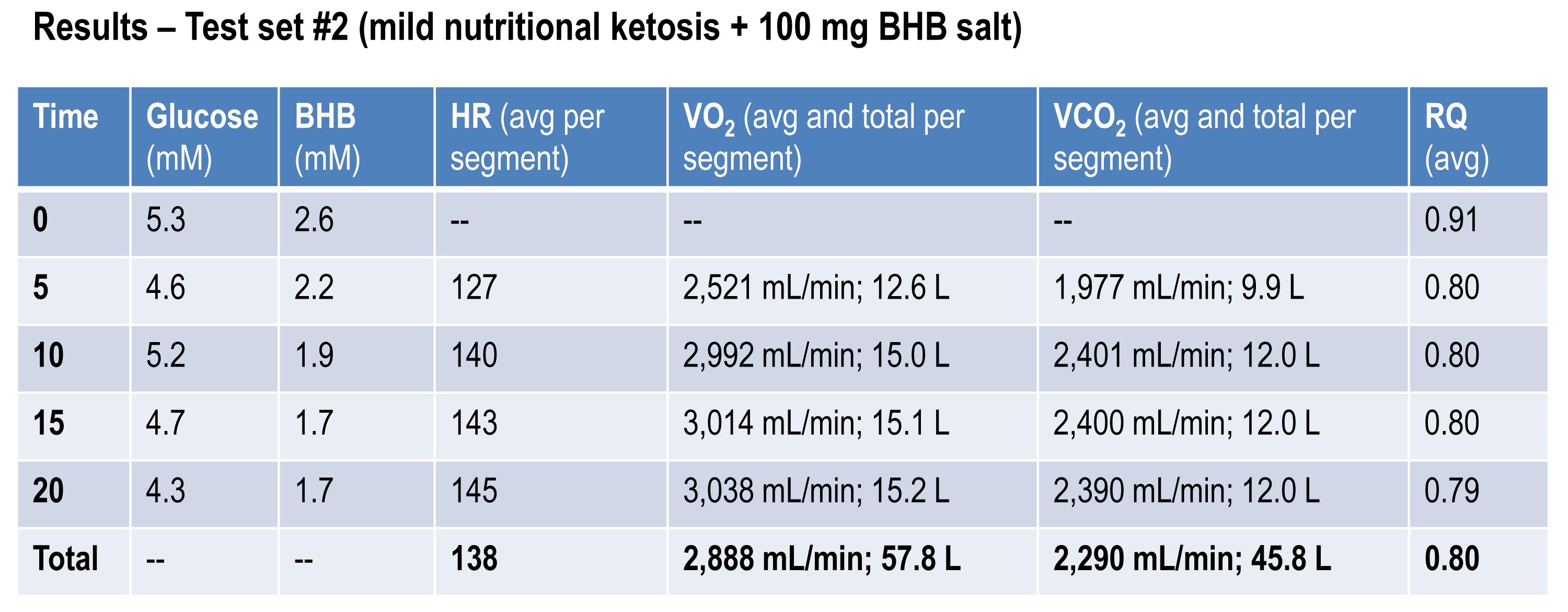
If you do the same calculations as I did above for estimating fat oxidation, you’ll see that EE in this case was approximately 13.92 kcal/min, while fat oxidation was only 67% of this, or 9.28 kcal/min, or 1.03 g/min. So, for this second effort (the test set) my body did about 5% less mechanical work, while oxidizing about 25% less of my own fat. The majority of this difference, I assume, is from the utilization of the exogenous BHB, and not glucose (again, I will address below what I think is happening with glucose levels).
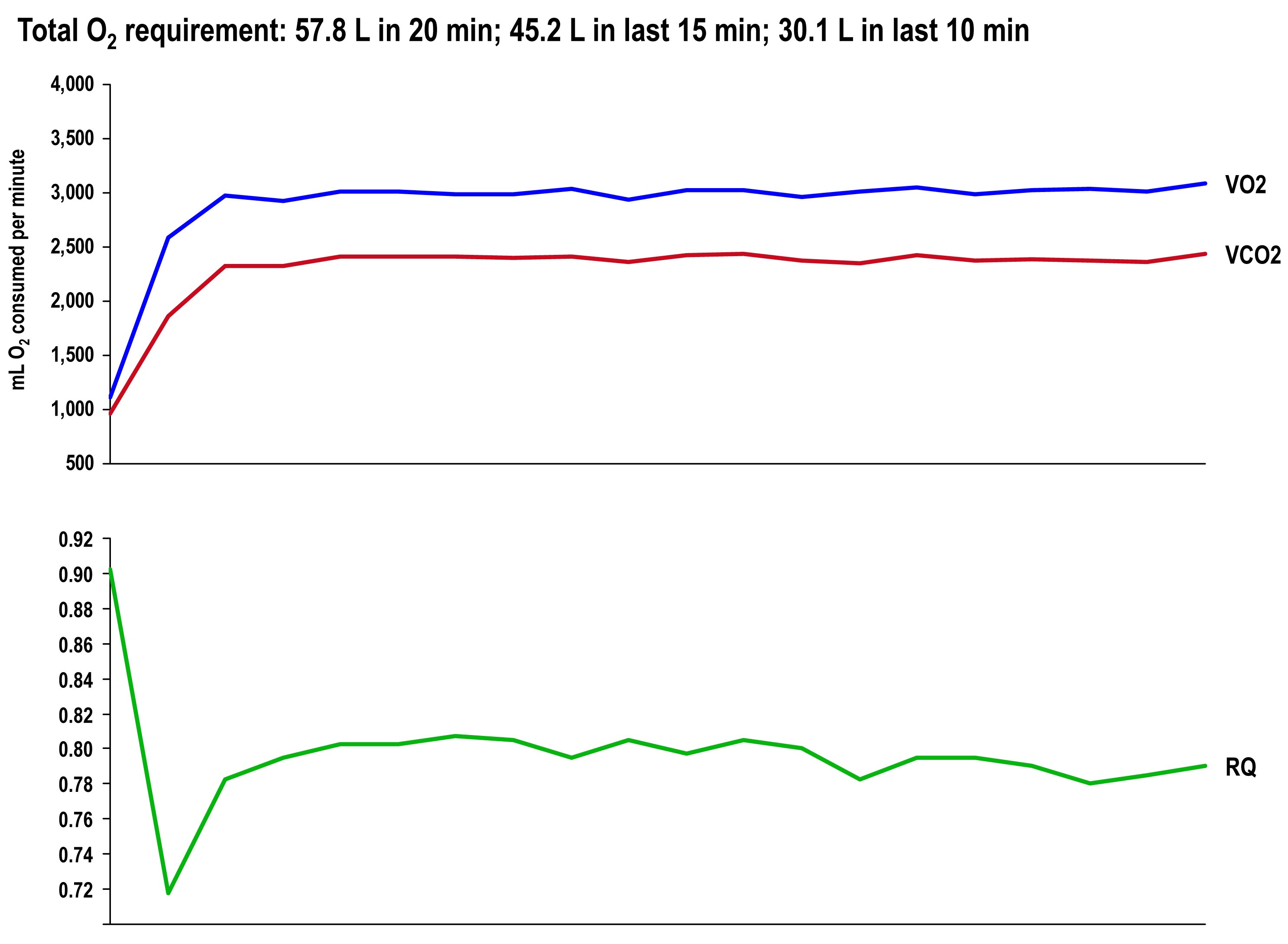
The graph once again shows the continuous data for VO2, VCO2 (measured), and RQ (calculated).
Side-by-side difference
The final graph, below, shows the continuous data for only VO2 side-by-side for the 20 minute period. The upper (blue) line represents oxygen consumption under control conditions, while the lower line (red) represents oxygen consumption following the BHB ingestion. In theory, given that the same load was being overcome, and the same amount of mechanical work was being done, these lines should be identical.
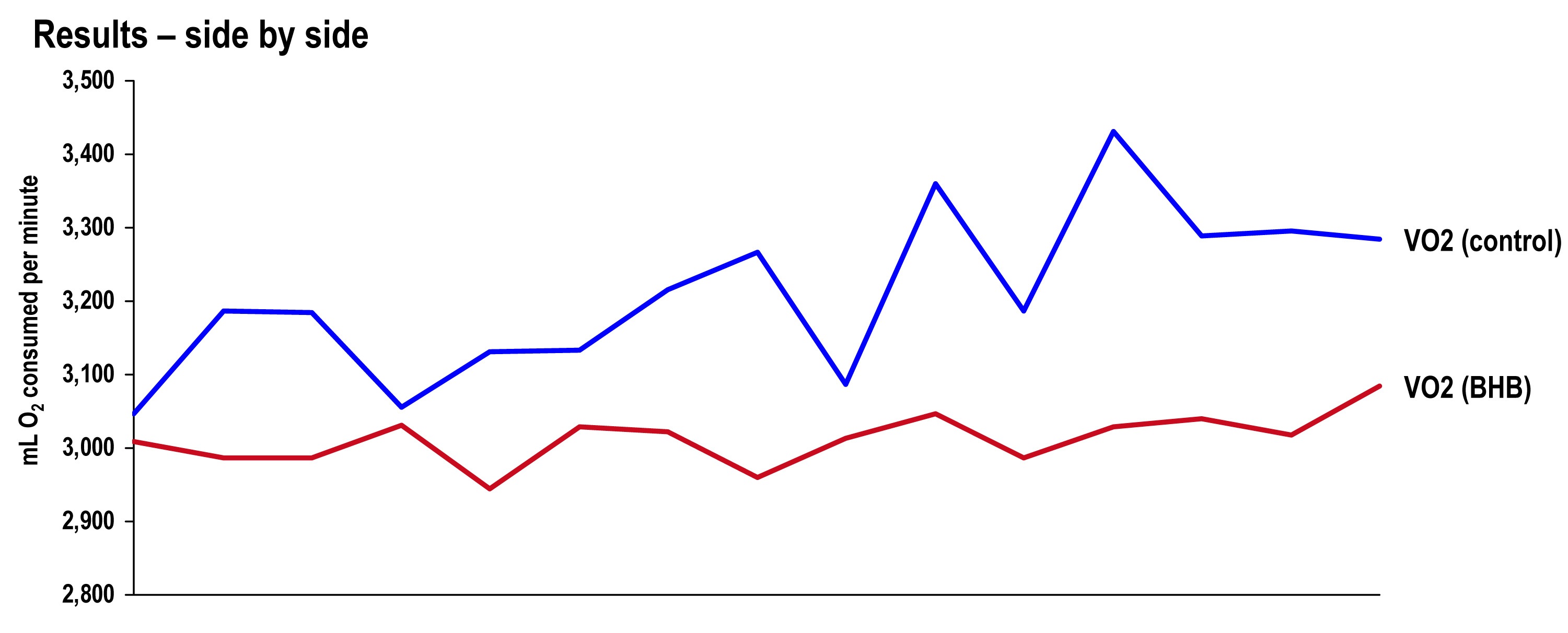
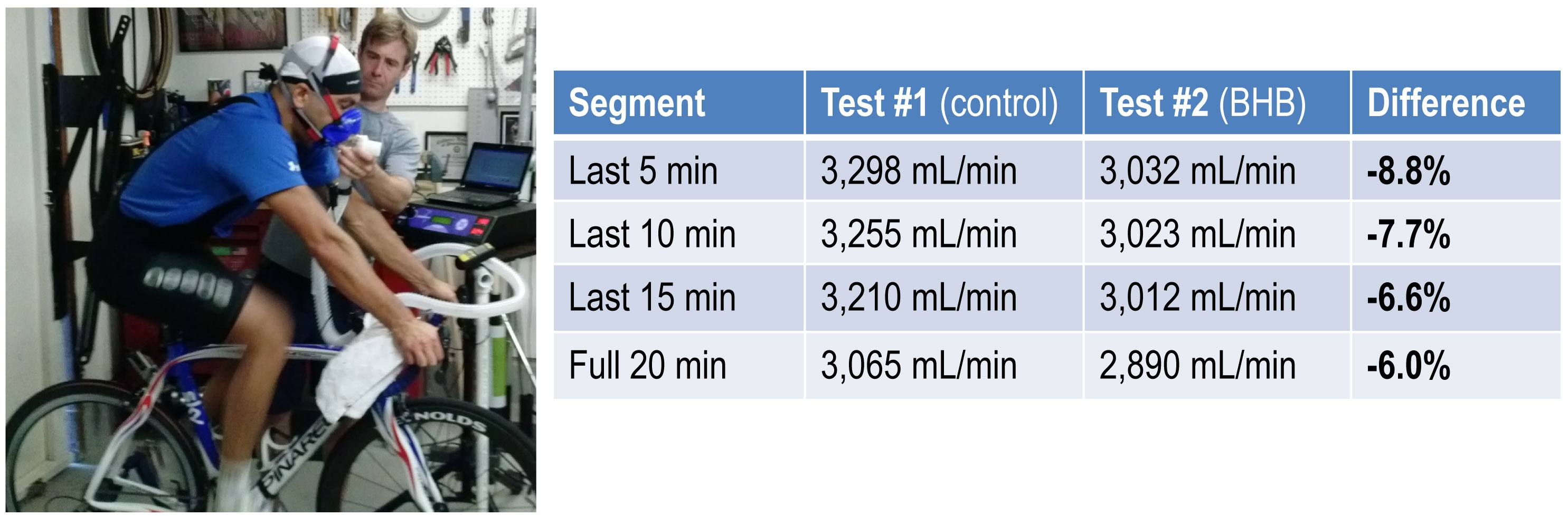
The hypothesis being tested in this “experiment” is that they would not be the same. Beyond visual inspection, the difference between the lines appears to grow as the test goes on, which is captured in the tabular data showing 5 minute segmental data.
Limitations
The most obvious limitation of this endeavor is the fact that it’s not an appropriately controlled experiment. Putting that aside, I want to focus on the nuanced limitations—which don’t impact the primary outcome of oxygen consumption—even if one were appropriately doing a real experiment.
- It’s not clear that the Weir coefficients used to estimate EE are relevant for someone in ketosis, let alone someone ingesting exogenous BHB. (The Weir formula states that EE is approximated by 3.94 * VO2 + 1.11 * VCO2, where VO2 and VCO2 are measured in L/min; 3.94 and 1.11 are the Weir coefficients, and they are derived by tabulating the stoichiometry of lipid synthesis and oxidation of fat and glucose and calculating the amount of oxygen consumed and carbon dioxide generated.) While this doesn’t impact the main observation—less oxygen was consumed with higher ketones—it does impact the estimation of EE and substrate use.
- In addition to the Weir coefficients being potentially off (which impacts EE), the RQ interpretation may be incorrect in the presence of endogenous or exogenous ketones. As a result, the estimation of fat and glucose oxidation may be off (though it’s directionally correct). That said, the current interpretation seems quite plausible—greater fat oxidation when I had to make my ketones; less when I got my ketones for “free.”
Observations from this “experiment” (and my experience, in general)
Animal models (e.g., using rat hearts) and unpublished case reports in elite athletes suggest supplemented BHB produces more ATP per unit carbon and per unit oxygen consumed than glycogen and FFA. This appears to have been the case in my anecdotal exercise.
The energy necessary to perform the mechanical work did not appear to change much between tests, though the amount of oxygen utilization and fat oxidation did go down measurably. The latter finding is not surprising since the body was not sitting on an abundant and available source of BHB—there was less need to make BHB “the old fashioned way.”
As seen in this exercise, glucose tends to fall quite precipitously following exogenous ketone ingestions. Without exception, every time I ingested these compounds (which I’ve probably done a total of 25 to 30 times), my glucose would fall, sometimes as low as 3 mM (just below 60 mg/dL). Despite this, I never felt symptomatic from hypoglycemia. Richard Veech (NIH) one of the pioneers of exogenous ketones, has suggested this phenomenon is the result of the ketones activating pyruvate dehydogenase (PDH), which enhances insulin-mediated glucose uptake. (At some point I will also write a post on Alzheimer’s disease, which almost always involves sluggish PDH activity —in animal models acute bolus of insulin transiently improves symptoms and administration of exogenous ketones does the same, even without glucose.)
In addition, the body regulates ketone production via ketonuria (peeing out excess ketones) and ketone-induced insulin release, which shuts off hepatic ketogenesis (the liver making more ketones when you have enough). The insulin from this process could be increasing glucose disposal which, when coupled with PDH activation, could drive glucose levels quite low.
If that explains the hypoglycemia, it would seem the absence of symptoms can be explained by the work of George Cahill (back in the day; see bottom figure in this post)—when ketone levels are high enough they can dominate brain fuel, even ahead of glucose.
Finally, these compounds seemed to have a profound impact on my appetite (they produced a strong tendency towards appetite suppression). I think there are at least two good explanations for this, which I plan to write about in a dedicated post. This particular topic—appetite regulation—is too interesting to warrant anything less.
Open questions to be tested in real experiments
- Are these results reproducible? If so, how variable are the results across individuals (by baseline metabolic state, diet, fitness)?
- Would the difference in oxygen consumption be larger (or smaller) in an athlete not already keto-adapted (i.e., not producing endogenous ketones)?
- Would the observed effect be greater at higher plasma levels of BHB (e.g., 5 to 7 mM), which is “easily” achievable with exogenous ketones?
- Would the observed effect be the same or different at higher levels of ATP demand (e.g., at FTP or at 85-95% of VO2 max)?
- Would the trend towards improved energy efficiency continue if the exercise bout was longer in duration (say, greater than 2 hours)?
- How will exogenous ketones impact exercise duration and lactate buffering?
- Why do exogenous ketones (both BHB and AcAc it seems) reduce blood glucose levels so much, and can this feature be exploited to treat type 2 diabetes?
- Are there deleterious effects from using exogenous ketones, besides GI side-effects?
- What are the differences between exogenous BHB and AcAc (which in vivo exist in a reversible equilibrium) on this particular phenomenon? (Work by Dom D’Agostino’s group and others have shown other differences in metabolic response and clinical application, including their relative impact on neurons.)
Photo by Alexey Lin on Unsplash

Hi Peter, which product did you use for this experiment?
BHB (sodium) salt.
Hello Peter, I really respect you and admire your approach and thinking to diets and health, which often goes against the mainstream. Anyway could I please get your thoughts about Gout? The conventional wisdom or what most doctors tell folks is to cut out all or most red meats, proteins, and eat a lot of carbohydrates and fruits etc. However my hunch is that lower carb diets are actually better for gout in the long run and do not greatly increase Uric Acid levels and may in fact lower than which is against the mainstream thoughts.
I’ve been reading some articles that suggest that fructose actually greatly increased uric acid levels in the body vs decreasing it – which would go against the general consensus of eating large amounts of fruit etc. What are your thoughts on this?
I used to do low carb fairly consistently 8 – 10 years ago, then got off it for some reason, and stopped working out, gained a bunch of weight etc. Anyway I’ve been wanting to go back to the low carb lifestyle in a big way and get back to working out like I used to with weights, however I recently had an episode of gout, which I never had in my life, should I have any worries about going back to low carb? My though is that in the beginning phases could be at risk, however overall I think eating low carb is actually better and will benefit me.
anyway I would love to get your general thoughts on this as you seem to know your biochemistry very well and may have some theories
thanks
It might be a bit of both and might depend on the individual and other factors. I think there are good explanations for both the “too much protein” and “too much sugar (fructose)” route, though the former is considered the conventional wisdom. To read up on the latter, check out the work of Richard Johnson at the University of Colorado. His book (I think it’s called Fat Switch or something like that) is good.
Hi Peter: What is your view on creatine, arginine and alanine supplements?
Peter,
I’ve been on a Ketogenic diet for several months now, and started checking my blood with a meter for the first time January 01, 2015. I’m in Ketosis every time I take a reading, however my numbers only range between .7 and .9. Once in a while I’ll hit 1.0 to 2.0 at the most. What do I have to do to get above 2.0 more consistently, and does it matter? I can honestly say I feel a certain degree of mental clarity as it is, but can that improve with higher numbers, and can you feel a difference?
Thank you,
You have one other article with VO2Max testing here:
https://eatingacademy.com/how-a-low-carb-diet-affected-my-athletic-performance
and in that you give a very useful linear relationship where the percent of fat used in aerobic metabolism is a function of CO2 over O2. Do you happen to have the actual equation for that relationship or an idea where to find it? The reason to have the actual equation is so we can modify our own VO2Max test data and do calculations at each level of exertion about the approximate amount of fat and glucose being used at those levels.
Yes, to a first order it’s dervived by know that RQ=0.7 is approx 100% fat ox and RQ=1.0 is approx 100% CHO ox. Linear equation.
Good morning all!
I have been follwing a keto lifestyle for a couple months now. It is a personal experiment to see how I can push my performance to the next level. I will be running a Half Marathon on this specific nutritional lifestyle.
In previous races, I had relied greatly on Carbs as energy. My traditional “final prep” is described below:
*The Night Before the Race*
Eat a big meal at least 12 hours before race time. Don’t eat anything that you haven’t had before or something that bothers your stomach. No dessert, no salad. After this meal take a light walk.
*Race Morning*
*4 hours prior to the start*
Ingest 1.5 to 2 grams of carbohydrate per pound of my body weight. Taken through a liquid carb drink and the rest in bagels, bread, bananas, honey… whatever is best. Drink AT LEAST 32 ounces of water with this meal to start the digestive process and the water does this.
*Two hours prior to the start*
Ingest .5 to 1 gram of carbohydrate and AT LEAST 24 ounces of water.
*One hour prior to the start*
Ingest a small carbohydrate snack and 16 ounces of water or Gatorade. Powerbars etc. seem to have a bad effect, fresh stuff like bread and honey, and bananas seemed to work well.
*10 minutes prior to the start*
Drink 10 ounces of sports drink. I like accelerade because it has some carb and protein.
What race day nutrition would be most beneficial for a body in ketosis? As far as supplements, I am equipped with UCAN Superstarch and Vespa energy packets. I am looking for information to consider in regards to what I should look to eat the night before and the final hours leading up to the race. Any information to share is greatly appreciated. Thanks!
I have tried the BodyBio brand Sodium/Potassium Butyrate which contains about 500 mg of butyric acid. It runs straight through me. I find that odd since butyrate is supposed to nourishing to the gut. I would really like to understand the physiology of why some of us cannot tolerate it. I thought it was just me until your report in this article.
Just small correction. In article you say that RQ is calculated as the ratio of VO2 and VCO2. It is the inverse, the ratio of VCO2 over VO2. Technically, that ratio for a whole body measurement is RER. RQ refers to that same measurement in a specific muscle group, which in this case you probably did not have. So you were probably measuring RER = VCO2/O2
I just found this site and really like the discussions. I am a powerlifter and KB lifter and have experienced the exact same result. I am talking glucose and ketone blood readings before and after training sessions. I am starting to suspect it is related to volume. On my high volume days (usually squat/deadlift), my glucose number goes up 50 points and my ketones drop. On these days I also have several sets of high intensity. I have also gotten a large glucose spike on an extreme KB day, but not with a more normal workload. The swing is less with lighter days. I am experimenting with different loads and volume and also with different supplements. Coconut oil before training seems to help on the light/medium days but not on the days with a heavier load. I want to minimize the glucose rise, so any ideas would be appreciated.
Hi Peter,
Have you thought much about how ketogenic states or NK might be applicable to folks with glycogen storage diseases? IE – Phosphoralayse Deficiency/ McArdle’s disease. Many patients with McArdle’s are self-experimenting with ketosis and there is anecdotal/ common-sensical reason to believe someone who can’t access muscle stored glycogen could enter into ketosis more quickly than the average Joe/Jane and alleviate symptoms of exercise intolerance. The problem with most experiments on McArdle’s is that there are so few people to merit good clinical trials, so patients end up self-testing and reporting it back (*with giant disclaimers*) to the group (see the “Ketosis in Mcardle’s” facebook group, or self-published blogs by people w/ McArdle’s). I have McArdle’s (though milder symptoms, for some reason, than most) and would like to work with a nutritionist to monitor NK and improved exercise performance, but have had trouble finding docs/ nutritionists who are educated enough to really feel comfortable recommending ketosis. Any chance you know of a like-minded colleague in the Central Texas (Austin) area?
Yes, I’ve thought about this a lot and have even tried to talk some folks into doing a clinical trial of NK supplemented with UCAN (which has made a big difference in GSD).
I agree with your hypothesis, but I don’t know who you could see in Austin. Sorry.
HELP–SFA and LCHF diet for CKDisease stage 3-5 is untested. Yet diabetics benefit nd improve greatly from this diet. But with a single kidney, and filtration issues (low eGFR) I need to learn how HF in my diet (NOT high protein – the 40-60gr daily of protein serve me well) but how FATS may harm filtration? I am looking for the SWEET SPOT of fat I can consume for health, stave off dialysis, and weight loss. ( ALL other factors, BP, sleep, meds, Trig.LDL,etc are perfect, but weight loss needed, <13 lbs in 45 days on LCHF. Ideal protein for me is dairy-full fat yogurt, cheese, butter, eggs, hemp protein, <50 carbs.)
thanks- here is one study:
https://www.renalandurologynews.com/high-fat-low-carb-diet-beneficial-for-ckd-patients/article/314032/ << last line confirms NO studies on CKD3-5 who MIGHT benefit the most!!!
Can you provide more info or your thoughts? Most nephrologists are old school, no idea on nutritional ketosis, or most dietitians either. they all freak at the word HF, and still relate it to CHD causing…
you said:
Dr. Peter Attia is a very-low-carbohydrate, ketogenic diet proponent who believes that elevated LDL-P values warrant dietary modification, including reduction in saturated fatty acid (SFA) intake. I He goes on to say: "While I believe the population-based guidelines for SFA are not supported by a standard of science I consider acceptable, it does not imply I believe SFA is uniformly safe at all levels for all individuals."
Hey Peter,
Interesting anecdote to report and wondering if you or anybody else can sympathize. Being in ketosis seems to make my vision BETTER. I’ve been keto for about 2 years with obvious junky carb days when willpower is low. Those junky carb days are then followed by a day or two of slightly blurry vision. Better vision comes back with MCT oil coffee and resumption of keto diet.
Interesting. I have not heard that before.
Several people have reported to me improved vision with the ketogenic diet and ketogenic supplementation (MCT and BHB salts). This may be due to lowering of blood glucose and improved blood flow associated with ketone metabolism
Paleo x 5 years with increasing ketogenic dieting x 1.5 years. Today while on a extended fast (48 hours into zero calorie only water fast ) I noticed I can read without glasses for the first time in probably 15 years. I estimate improved vision of about 35-40% over baseline but enough to read without glasses.
I plan to follow this more by standardized vision testing on fasting days comparing to feeding days. I do IF regularly 18-20 hours a day. Absolutely fascinating.
For what it’s worth, at my last eye test the optician reported that my eyesight had in fact somewhat surprisingly improved, so I seem to be more anecdotal evidence in line with the above/below comments. Context: I have astigmatism which affects my far-sight, and at this point when the test was done, I had been on a ketogenic diet and had substantially adapted, having been on it for perhaps 9-12 months which sprang from my interest in endurance running. I am 45 y/o. And as I say, during testing it became obvious my far-sight had apparently improved noticeably. She mentioned that far-sigh sometimes improves as a result of progressing age, but that this usually coincides with weakening near-sight, due to the hardening of the eye lens etc. However whereas my far-sight had measurably improved there were no indication of any weakening of near-sight. Her comment was just “Keep doing whatever you’re doing.” 🙂
I’ve been upping my fat intake (mostly unsaturated) over the last 6 months via tweaked Soylent and am very interested as an endurance athlete about the ability to oxidize more fat at higher heat rates. Is there any way a person on a budget can get a sense during a workout of their fat vs cho oxidation? I can’t even afford (or should I say, justify) a power meter for the bike… Is there any correlation between V02 (or simple breathing rate) and fat vs cho oxidation for the same power output? I suppose if someone does ever make a wrist worn device that could report instantaneous fat vs cho calorie consumption they’ll do well selling to the endurance athletes out there..
I am a female professional cyclist and am very interested in learning more about utilizing a higher ketosis diet. My first question would be, can I sustain this type of diet during the racing season when I will have to go anaerobic at some points during races or should I reserve implementing a higher ketosis diet during off-season when I am doing more aerobic base type training?
I also administer metabolic testing at a facility in Scottsdale, AZ and see numerous athletes everyday who may benefit from utilizing a ketosis diet. Where can I send them for more information on how to go about creating a keto diet that is specific to them and their training objectives?
Thank you for your help. I look forward to hearing back from you. Smiles.
Very fascinated by this topic and any research and observations that have been made. Ready to share the ability to add ketones into the body through a much more pleasant and tasty method than in your research… reaching ketosis in under 59 minutes. http://www.facebook.com/pruvitnow I would enjoy your feedback as a professional in the field.
Anna- I am also a cyclist and have been playing around with Exogenous Ketones. Seeing interesting results from them and so far a big fan. They are available now to the market place and so far anybody on the cycling front I know of are seeing good results from them.
Chris
I am an endurance athlete and suspect I have been training in a state of ketosis for many years.
I have been doing long runs and bike rides without ingesting much and training my body to burn fat for energy. I was interested to read your entry Ketosis part 2 as it relates to aerobic exercise.
Is it possible to starve the liver of glycogen and cause damage to it through exercising in ketosis.
Hi Dr. Attia,
Have you heard of or tried Keto-OS by Pruvit? It is based on BHB salts and coconut. It is revolutionary. The taste is phenomenal and will provide the results you were seeking with this experiment. Please email me for more details 🙂
Lori, MS, RD, CSCS
I have just started taking KETO-OS and have noticed a huge difference in my energy levels as well as mental clarity. On concern I have that no one has brought up yet is, does this in any way have a negative effect on the liver? Also, there is a lot of sodium in this product 40%, is this a concern for blood pressure at all?
I am also interested in your feedback on keto//os and answers to the questions about liver…and not so I can sell it–I really could care less. I really would love your expertise on what we are ingesting. Mytime.justpruvit.com is the link to the keto//os info.
Looking to purchase exogenous ketones, Is there a brand that is recommended?
See what Prototype Nutrition is selling.
I don’t know if you have heard of this, but in India and several other countries, some individuals drink their own urine. It is said to be particularly effective in the morning and when fasting, and to be very beneficial to one’s health. The morning and fasting would also be the times that higher levels of ketones would be in the urine, is that correct? I’m not aware of any scientific studies, but for better or worse here is a wikipedia link: https://en.wikipedia.org/wiki/Urophagia
Peter,
Came across your work thanks to Tim Ferris’ podcast featuring you. I plan to try to absorb as much of the information you are sharing in your blog. Thank you for putting it out.
As a competitive rower training 4-6 hours/day, a father of 5, and a full time IT employee; I find it sometimes difficult to keep my mental focus. I have utilized ketosis in my journey from being a 450lb couch potato to 220lb rower still struggling to lose the last 20 or so pounds to allow me to make my really fly.
What I have absorbed so far has been enlightening but has brought up a bunch questions, which I will wait to ask after I have done the adequate reading.
Again, thank you for your work, and self-experimentation.
Carlos
Interesting. You state that O2 consumption should be the same for the same amount of work – I thought that burning fat needed slightly more O2 per molecule of ATP produced. As to the very different O2 consumptions in your two tests – do you have the biochemical explanation for this? Presumably it relates to how BHB is metabolised and how many ATP molecules are produced per O2 used, but it would be nice to know the details.
I think I wrote about extensively in another series on ketosis. It has to do with delta G.