Erin Michos is an internationally-known leader in preventive cardiology and women’s cardiovascular health. In this episode, Erin discusses current trends in cardiovascular disease (CVD) through the lens of female biology and the observation that major adverse cardiac events in both sexes are on the rise. She walks through risk factors including LDL-cholesterol, apoB, and Lp(a) and makes the case for the importance of early preventative measures. She explains various interventions for reducing risk including a discussion of statins, GLP-1 agonists, PCSK9-inhibitors, and drugs that lower Lp(a). She goes in-depth on female-specific factors that contribute to CVD risk such as pregnancy, grand multiparity (having five or more children), oral contraceptives, menopause, and polycystic ovary syndrome (PCOS). Additionally, she explains her approach with patients as it relates to the use of hormone replacement therapy and provides advice for people wanting to lower risk both through lifestyle changes and medications.
Subscribe on: APPLE PODCASTS | RSS | GOOGLE | OVERCAST | STITCHER

We discuss:
- Erin’s background in preventive cardiology and women’s health [2:30];
- Recent trends in cardiovascular disease in women, mortality data, and how it compares to cancer [5:15];
- Why early preventative measures are critical for cardiovascular disease risk [13:15];
- ApoB as a causal agent of CVD, and why high apoB levels are not being aggressively treated in most cases [19:45];
- The rising trend of metabolic syndrome and other factors contributing to the regression in progress of reducing cardiac events [27:00];
- GLP-1 agonists—Promising drugs for treating diabetes and obesity [33:30];
- Female-specific risk factors for ASCVD (pre- and post-menopause) [37:15];
- Polycystic ovary syndrome (PCOS): prevalence, etiology, and impact on metabolic health, lipids and fertility [47:00];
- The effect of grand multiparity (having 5+ children) on cardiovascular disease risk for women [52:30];
- The impact of oral contraceptives on cardiovascular disease risk [55:00];
- The effect of pregnancy on lipids and other metabolic parameters [58:45];
- The undertreatment of women with familial hypercholesterolemia (FH) and how it increases lifetime risk of ASCVD [1:02:00];
- How concerns around statins have contributed to undertreatment, and whether women should stop statins during pregnancy [1:09:45];
- How Erin approaches the prescription of statins to patients [1:16:00];
- PCSK9 inhibitors and other non-statin drugs [1:21:15];
- Advice for the low- and high-risk individual [1:28:30];
- The impact of nutrition, stress, and lifestyle on lipids and CVD risk [1:31:00];
- Lp(a) as a risk enhancer for cardiovascular disease [1:41:15];
- The effect of menopause on cardiovascular disease risk [1:50:30];
- How Erin approaches decisions regarding hormone replacement therapy (HRT) for her patients [1:55:30];
- The urgent need for more data on women’s health [2:03:30];
- Erin’s goal of running a marathon in every state [2:09:45]; and
- More.
Get Peter’s expertise in your inbox 100% free.
Sign up to receive An Introductory Guide to Longevity by Peter Attia, weekly longevity-focused articles, and new podcast announcements.Erin’s background in preventive cardiology and women’s health [2:30]
- Erin has been at Hopkins for 22 years
- She did her residency from 2000-2003 and stayed on for a cardiology fellowship
- Then she joined the faculty
- She’s been faculty for over 15 years
- Peter did his residency in general surgery there too, from 2001-2006
- This made him realize they probably passed each other somewhere in the emergency room during residency
When Erin went into medicine, did she know she wanted to do cardiology?
- When she went into medicine, yes
- In college, she didn’t know she was going into medicine
- There are no doctors in her family; she’s the first one
- She started her undergraduate studies at Northwestern as a molecular biology major
- She interacted with so many pre-med students who were her classmates
- Their enthusiasm about entering the field was contagious
- She was doing a lot of bench science, which is a really good experience
- Erin adds, “I think anybody entering science and medicine should have some bench lab work experience”
- She began to long for more direct clinical research with direct patient exposure
- In her last year of undergrad, she switched to being pre-med
- She applied to both PhD and medical programs
- When she started medical school, she fell in love with cardiology
- As medical student, even before residency
- She has a real interest in diet and nutrition, and exercise and lifestyle
“We think that over 90% of cardiovascular disease is due to preventable modifiable risk factors”‒ Erin Michos
- There’s so much we can do for prevention and this is why Erin really loves being a preventive cardiologist
- When she entered residency, she already had her eye on a cardiology fellowship
- She did 3 years of a medical residency (which is standard) and 4 years of cardiology
- The cardiology program was longer because it emphasized research
- She did 2 years of research on a T32 program in cardiovascular epidemiology, and that’s where she got her master’s in health science
Recent trends in cardiovascular disease in women, mortality data, and how it compares to cancer [5:15]
Why doesn’t prevention get more attention?
- Data from the INTERHEART study show that 90% of myocardial infarction risk was due to preventable risk factors
- Peter tells his patients that ASCVD (atherosclerotic cardiovascular disease) is the leading cause of death
- He was surprised last year to realize how much bigger the gap is between ASCVD and cancer globally than in the US
- ASCVD is #1 in both the world and US
- But outside the US, ASCVD causes 18-19 million deaths where as cancer causes 10-11 million deaths (per year)
- ASCVD causes almost 2x more deaths than cancer
- Peter asks, “When you take into account what you just said, that between smoking, hypertension and controlling apoB, you could basically turn that into a disease that would barely rank on the top 10. Does it surprise you that this doesn’t get more attention?”
- It surprises Erin, and she’s concerned that we’re reversing these trends
Recent trends in cardiovascular disease
- The first statin, lovastatin, was approved in 1987
- That along with efforts in smoking cessation and blood pressure treatment, there was a significant decline in cardiovascular disease mortality in men
- During this time, unfortunately, CVD mortality was rising in women till around the year 2000 when this came to attention
- And after that time there was dramatic decline in cardiovascular disease mortality in women and continued decline in men
- But unfortunately, in recent years we are no longer making these strides in progress anymore
- In fact, we’re no longer even stagnated
- There has been a frank uptick in cardiovascular disease mortality in both men and women due to the epidemics of obesity and diabetes and cardiometabolic diseases
- Cardiovascular disease mortality is on the rise in younger women
- And when you look at rates of change, the fastest growing heart disease death rate is in middle-aged women aged 45 to 64
- So we really need to double down on our preventive efforts, and it’s really disheartening to see that we’re no longer making the progress that we used to
- If these trends are not overturned, heart disease is set to overtake cancer as the leading cause of death in younger women as well
- Peter comments on mortality data
- In middle age, cancer is the biggest killer
- In old age, cardiovascular disease and neurodegenerative disease dominate
- He finds this very concerning that cardiovascular disease may eclipse cancer in middle age
Erin’s focus on women’s health
- Erin is focused on women’s health, and cardiovascular disease is the leading cause of death in women
- Women more often fear breast cancer, but far more women are likely to die of cardiovascular disease than cancer
- However, in younger individuals (under the age of 65), cancer is still the leading cause of death in women
- One of her studies tracked death rates in younger women under the age of 65 in the US looking at CDC WONDER data over a 20-year period from 1999 to 2018 (see the figure below)
- They showed during this time that cancer mortality has been declining in younger women
- But since 2010, heart disease mortality in younger women is no longer declining, and it’s actually rising at 0.5% per year
- It’s narrowing the gap between cancer deaths and heart disease deaths in women under 65
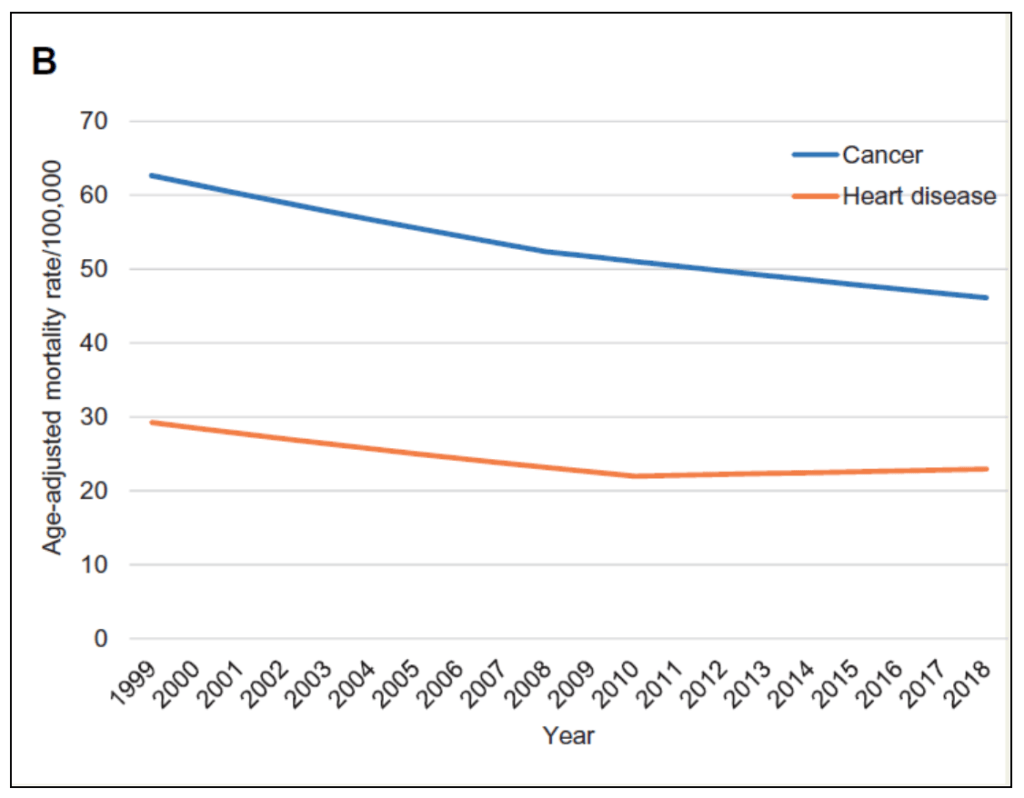
Figure 1. Mortality fates of women under 65 due to heart disease and cancer, 1999-2018. Image credit: EHJ:QCCO 2022
- Erin is discouraged, “If these trends are not overturned, heart disease is set to overtake cancer as the leading cause of death and younger women, which is really discouraging considering that we have so many more tools now for prevention”
{end of show notes preview}
Would you like access to extensive show notes and references for this podcast (and more)?
Check out this post to see an example of what the substantial show notes look like. Become a member today to get access.

Erin Michos, M.D.
Dr. Erin Michos is an Associate Professor of Medicine within the Division of Cardiology at Johns Hopkins School of Medicine. She has a joint appointment in the Department of Epidemiology at the Johns Hopkins Bloomberg School of Public Health. She is the Associate Director of Preventive Cardiology with the Ciccarone Center for the Prevention of Cardiovascular Disease at Johns Hopkins. She is a Fellow of the American College of Cardiology (FACC) and a Fellow of the American Heart Association (FAHA).
Dr. Michos completed medical school at Northwestern University in Chicago, IL, and then completed both her Internal Medicine residency and Cardiology fellowship at the Johns Hopkins Hospital in Baltimore, MD. She also completed her Masters of Health Science degree in Cardiovascular Epidemiology at the Johns Hopkins Bloomberg School of Public Health.
Her research interests are in the areas of Preventive Cardiology and Cardiovascular Epidemiology, with particular focus on (1) physical activity and nutrition; (2) risk prediction for cardiovascular disease including the use of coronary artery calcium scores and biomarkers, (3) lipids and statin therapy, (4) cardiovascular disease among women, and (4) vitamin D.
As part of the Johns Hopkins cardiology faculty, her clinical duties entail seeing patients in the Preventive Cardiology outpatient clinic and the Echocardiography lab. She also teaches students at the Johns Hopkins University Medical School and the Bloomberg School of Public Health. She is the Chair of the Women’s Task Force for the Cardiology Division at Johns Hopkins. She is part of the Editorial Board for the journal Circulation.
Dr. Michos is a co-investigator on the NIH-funded Multi-Ethnic Study of Atherosclerosis (MESA) and Atherosclerosis Risk in Communities (ARIC) studies. She is an investigator in an on-going NIH-funded clinical trial (STURDY trial) studying vitamin D and fall prevention. She is the Training Director for the AHA fellowship program for the AHA’s Go Red for Women Strategic Focus Research Network at Johns Hopkins for research in women’s cardiovascular health.
Dr. Michos has authored or co-authored over 200 manuscripts in peer reviewed journals. She also contributes a monthly article for the US News and World Report Health Section for the public audience. She is also a frequent contributing writer to Johns Hopkins Medicine’s Healthy Heart and Healthy Woman websites. [Johns Hopkins]
Twitter: @ErinMichos



