Ethan Weiss is a preventative cardiologist at UCSF, an entrepreneur-in-residence at Third Rock Ventures, where he is working on a project related to cardiometabolic disease, and a previous guest on The Drive. In this episode, Ethan compares and contrasts the diagnostic imaging tools, CAC (coronary artery calcium score) and CTA (CT angiography), used to image plaque—including the latest in CTA software—and how these tools inform our understanding of ASCVD risk and guide clinical decision-making. Ethan discusses the types of plaque that cause events and the data that make a case for optimal medical therapy over stenting outside of particular cases. He explains why high blood pressure is problematic and walks through the data from clinical trials testing aggressive treatment. He talks about the best way to actually measure blood pressure, why we shouldn’t simply accept that blood pressure rises with age, and how he uses different pharmaceutical agents to treat hypertension. Additionally, Ethan explains our current, but limited, understanding of the role of metabolic health in ASCVD. He discusses the impact of fat storage capacity and the location of fat storage and explains how and why there is still a residual risk, even in people who have seemingly normal lipids, don’t smoke, and have normal blood pressure.
Subscribe on: APPLE PODCASTS | RSS | GOOGLE | OVERCAST | STITCHER
We discuss:
- Ethan’s entrepreneurial work in the cardiometabolic disease space [4:30];
- Calcium scans (CAC scores) and CT angiography (CTA), and how it informs us about ASCVD risk [6:00];
- Peter’s historical CAC scores, CTA results, and how one can be misled [10:45];
- How Peter’s CTA results prompted him to lower his apoB [14:45];
- Calcium scans vs. CT angiogram (CTA) [21:15];
- How Ethan makes clinical decisions based on CTA results and plaque burden, and the importance of starting treatment early to prevent ASCVD [28:15];
- Improved methods of CTA to grade plaque lesions and how it’s shaped medical decisions such as stenting [33:45];
- Why Ethan favors optimal medical therapy over stenting outside of particular situations [41:45];
- The need for FFR CTA, and the potential for medical therapy to eliminate ASCVD [54:00];
- The fat attenuation index (FAI) and other ways to measure inflammation in a plaque [57:30];
- Statins and exercise may increase the risk of calcification, but what does this mean for risk? [59:45];
- The root cause of statin hesitation despite evidence that statins are a profoundly important intervention [1:05:30];
- Importance of keeping blood pressure in check, defining what’s normal, and whether we should just accept higher blood pressure with age [1:10:45];
- Blood pressure variability, how to best measure it, and data suggesting the enormous impact of keeping blood pressure down [1:21:00];
- Drugs for treating high blood pressure recommended by the ALLHAT trial [1:35:15];
- What the SPRINT trial says about the aggressive treatment of hypertension, and the risks of such treatment [1:38:15];
- Confirmatory results in the STEP trial for blood pressure, and how Ethan uses the various pharmacological agents to lower blood pressure in patients [1:43:15];
- The role metabolic health in ASCVD: what we do and don’t know [1:51:00];
- The impact of fat storage capacity and the location of fat storage on metabolic health and coronary artery disease [1:56:15]; and
- More.
Get Peter’s expertise in your inbox 100% free.
Sign up to receive An Introductory Guide to Longevity by Peter Attia, weekly longevity-focused articles, and new podcast announcements.
Ethan’s entrepreneurial work in the cardiometabolic disease space [4:30]
Ethan’s career has evolved over the past couple of years
- Ethan had a bit of a midlife crisis and decided he didn’t want to keep doing the same thing for the next 25 years
- He was given the opportunity to get involved with a local group of investors who create biotech companies
- He closed his lab and has become a volunteer clinical faculty at UCSF
- He sees patients infrequently
- He spends most of his time working to build a new company (he’ll explain more later)
Calcium scans (CAC scores) and CT angiography (CTA), and how it informs us about ASCVD risk [6:00]
A quick recap of what a calcium score (CAC) is and a CT angiogram (CTA)
- They spent a lot of time talking about the distinction between calcium scanning (CAC) and CT angiography (CTA) in Ethan’s previous podcast (at 1:40:15)
- They used the analogy that a calcium scan demonstrates a sight of a prior injury
- What we know is that the more calcium you have in your arteries, the worse you do
- The higher the risk of both cardiovascular and all cause problems
- We suspect that calcium represents a healed plaque, so the amount of calcium you have in your arteries is strongly related to the amount of plaque that you have in your arteries
We know that the amount of plaque you have in your arteries is related to your risk of having heart attacks and dying from heart attacks
- Ethan uses an analogy with his patients‒ a calcium scan is like a satellite image of your heart
- It gives you a sense of any damage that has occurred over your lifetime
- It also gives you a nice adjunct indicator of your overall risk of dying from a heart attack
- One of the nice things about a calcium score is it’s very, very low in radiation
- Even CTAs are low now (we’ll talk about that later)
- The calcium scan is also a very inexpensive tool; some places do these scans for ~$200
- (But you can still find some places still charging $2,000+ for the same scan)
- The calcium scan is a low-risk procedure; it doesn’t require dye
- And it provides great insight, especially the first time it’s done
Ethan did a “full 180” on the utility of calcium scans
- When he first started his cardiology practice in the early 2000s, he thought calcium scans were annoying, and he didn’t know what to do with them
- Obviously there’s epidemiologic value in understanding the risk of different populations
- Now he finds value in many contexts and even in individual patients
- A calcium scan doesn’t have value for everybody; in a 25-year-old, it is probably not worth anything
- Calcium scanning is now a tool that he uses regularly
- Peter explains this to patients as a 2×2 of young versus old and zero versus non-zero calcification (see the figure below)
- There are two areas where the scan provides insight (shown in blue below)
- Older people (70+) who have zero calcification
- Young people (45 or 50) who already have calcification
- And there are two areas where the scan does not provide insight (shown in white below)
- If a 40-year-old has a calcium scan of zero, you haven’t really learned a lot
- Further, if a calcium scan of zero in a 40-year-old is accompanied by other risk factors, Peter would not be dissuaded from aggressively treating those risk factors
- Similarly, when an 80-year-old has a calcium scan of zero, you might be less inclined to push for aggressive measures
- Even though there could be false negatives
- There are two areas where the scan provides insight (shown in blue below)
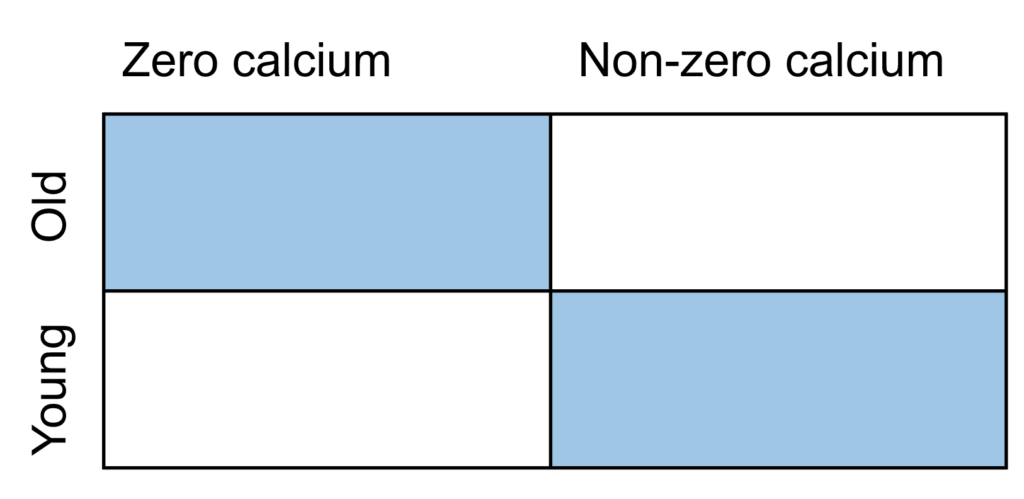
Figure 1. 2×2 for interpreting calcium scan results, with informative results highlighted in blue.
- Peter has spent some time in the literature on this and learned that a calcium scan is a relatively imprecise measure
- The thickness of the slices that are used in that scan are significantly greater than the slices that are used in the CT angiography
Peter’s historical CAC scores, CTA results, and how one can be misled [10:45]
- When Peter was in his mid 30s (2008/2009), he had his first calcium scan
- At the time, his doctor thought he was crazy because he was 35 and exercising at least 24 hours a week
{end of show notes preview}
Would you like access to extensive show notes and references for this podcast (and more)?
Check out this post to see an example of what the substantial show notes look like. Become a member today to get access.
Ethan Weiss, M.D.
Ethan Weiss got his bachelor’s degree from Vassar College. He completed his MD and residency at John Hopkins. He then went to UCSF where he completed a clinical fellowship in cardiology and postdoctoral research training. Dr. Weiss is an Associate Professor in the School of Medicine at UCSF where he practices preventive cardiology and conducts research.
In his research, Dr. Weiss uses genetic models to better understand the mechanism of metabolic disorders such as obesity, fatty liver disease, and diabetes. He also studies the blood clotting system and has interest in identifying novel ways to safely block clots associated with diseases such as heart attack and stroke without causing an increase in bleeding. He has conducted randomized clinical trials to assess the impact of nutritional interventions on weight loss, insulin sensitivity, and metabolism.
Currently, Dr. Weiss has shifted his attention to entrepreneurial work at Third Rock Ventures. He is working on a project related to cardiometabolic disease. He is also the Co-Founder and Medical Advisor for Keyto, a company that created an app and program to make it easier to follow a Mediterranean-style keto lifestyle. [UCSF Profiles]
Twitter: @ethanjweiss



