
For reasons I’m still struggling to understand, the idea of “nutritional ketosis” (NK, to be distinguished from starvation ketosis, SK or diabetic ketoacidosis, DKA) is often discussed and debated in much the same way as religion or politics. Perhaps this can be said of all nutrition, which is a shame. Nevertheless, in my continued defiance of such sensitive topics, I’d like to add another layer of complexity and nuance to this discussion.
The “rule of thumb” for NK is that caloric intake is determined as follows (this excludes a subset of ketogenic diets known as calorie-restricted KD which, as the name suggests, is specifically restricted in calories):
- Carbohydrate (total, not “net”): less than 50 gm/day, but ideally closer to 30 gm/day
- Protein: up to 1 to 1.5 gm/kg, but ideally below about 120 gm/day
- Fat: to satiety
Let me illustrate what this looks like for Joe (left), Jane (middle), and Jeff (right — an example of a calorie restricted KD), three hypothetical people in NK — but each with different caloric requirements.
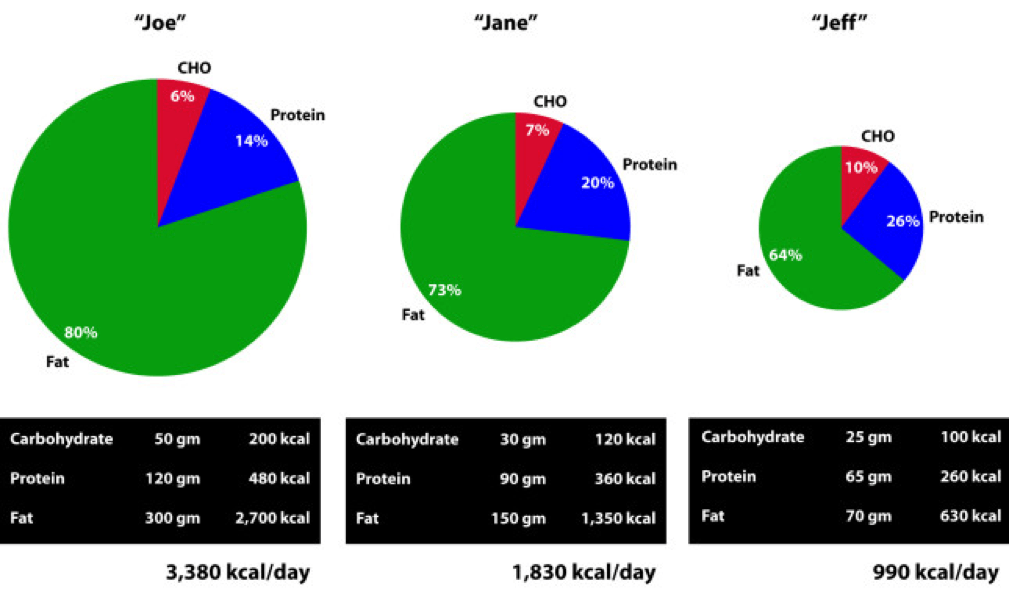
As a general rule, as caloric requirement increases the proportion of calories derived from carbohydrate and protein decreases (and the contribution of dietary fat increases), even while absolute intake of carbohydrate and protein increases.
Anyone who has bought a blood ketone meter knows how tough it can be to get “into” ketosis by carbohydrate restriction (since everyone asks, I use the Abbott Precision Xtra meter which uses two different strips: one for glucose and one for beta-hydroxybutyrate, or BHB). Most practitioners consider the minimum threshold of NK to be a fasting serum level of BHB above 0.5 mM. I’m a bit more stringent in my practice and like to see fasting BHB levels above 1 mM. To give you a sense of one person’s numbers (mine), over a 6-month stretch in 2013, when I was in NK, my mean (i.e., arithmetic average) morning fasting level was 1.7 mM with a median value of 1.4 mM. The highest morning level during that period was 5.2 mM. (The highest morning level I have ever measured in myself is 5.7 mM.)
But, it took me a long time to get it right, especially since at the outset of my foray into NK I was consuming between 4,000 and 4,400 kcal per day. (My average daily caloric intake for weight stability was about 3,800 kcal per day, which was validated by doubly-labeled water.) I could still easily “fall out” of NK. For example, on my daughter’s 5th birthday she insisted I have some of her tikka masala (contains lots of sugar), naan bread, and mango ice cream. How could I say no to a birthday girl who insisted on going to the nicest Indian restaurant in San Diego? As to be expected, the next day my BHB was 0.2 mM, and it took me 2 days to get back above 1 mM.
Here’s a little secret I’m about to let everyone in on… I like carbohydrates. I love sushi (though I now mostly eat sashimi). I love Indian and Thai food, though I prefer to make curry myself to keep sugar out. I make (and eat) the best hummus this side of the Nile River. I’ve figured out how and when I can eat them to meet the following conditions:
- Stay in NK (except on a few occasions like my daughter’s birthday);
- Increase my anaerobic performance;
- Preserve most (but not all*) of the benefits I enjoyed when I was much more strict about my ketogenic diet.
How, you ask? By learning to calculate my glycogen deficit.
(*) For me, the leanest body composition I achieved as an adult was in strict NK with no attempts to do what I’m about to describe below. Since I’m not a model and nobody cares if my body fat is 7% or 10%, I’m happy to be a little less lean if it gives me the flexibility to increase performance and live a slightly more sane life. At least for now.
PLEASE NOTE: I have never suggested, and can’t imagine I ever will suggest, that a KD is “best” or “right” for everyone. What I describe below may seem extreme, both in the amount of work required and the actual application. I fully acknowledge that (1) this is a highly analytical approach to eating, and (2) that I’m a “freak” (my wife’s words, not mine). I certainly don’t do this often, unless a lot is on the line (e.g., a big ride), but I like having this technique in my armamentarium.
If you’ve watched my presentation from 2013 at the IHMC, then you’re familiar with RQ. Through years of metabolic testing I have a pretty good sense of my RQ at any moment in time – when I’m sleeping, when I’m sitting around (most of the time), when I’m riding my bike at 200 watts, when I’m riding my bike at 400 watts, when I’m lifting weights, etc. This allows me to calculate what proportion of my energy I derive from glycogen and what proportion I derive from fatty acid. Consider the following example:
If I ride my bike at an average of 185 watts (you’ll need a power meter to infer this) for, say, 2 hours, I know my average RQ is between 0.76 and 0.80.
The approximate formula is %CHO = 3.333*RQ – 2.333, which can easily be derived from the observation that %CHO utilized increases linearly from 0% at RQ 0.7 to 100% at RQ 1.0.
Furthermore, I know my VO2 at 185 watts is 2.9 liters per min, which means (using the Weir formula which I presented previously) my energy requirement was about 14 kcal per minute, or 1,680 kcal over 2 hours. Hence, of these 1,680 kcal needed to pedal 185 watts for 120 minutes, 336 to 554 kcal came from glycogen. In other words, I utilized between 84 and 138 gm of glycogen.
(By comparison, several years prior to being in NK, this effort in me would have taken place at a slightly higher VO2 – closer to 3.2 liters per min – and at a much higher RQ – between 0.90 and 0.95 – meaning the exact same work output would have required somewhere between 300 and 400 gm of glycogen! That’s a real state of metabolic inflexibility. Basically, I was entirely dependent on carbohydrates for energy.)
Since the first metabolic priority for ingested carbohydrate is glycogen replenishment, I can, in this setting, consume probably somewhere between 60 and 120 gm of carbohydrate following this ride and stay in ketosis. Why? Because those carbohydrates are prioritized to replenish my glycogen stores AND I am highly insulin sensitive. Note the *AND* in this last sentence. (The especially astute reader will realize some of this glycogen debt will be replenished by protein and glycerol, the latter of which is liberated by lipolysis – see post on fat flux for a primer).
Clearly I didn’t consume this amount of carbohydrate on my daughter’s birthday, so why was I out of ketosis the next day? Because my glycogen debt was not high. Of course, I knew this and didn’t really care. But, if I know my wife wants to go out for sushi one night, and I know she’s going to make me eat a California roll, I can “rig it” such that I show up to dinner with a glycogen debt appropriate enough to enjoy them without significantly interfering with my liver’s BHB production.
Extreme example
At one point, I did two tough bike rides on consecutive days. Each day we rode 110 miles under challenging conditions. Over 6,000 feet of climbing each day and very strong winds, which were either headwinds or cross-winds. On top of this, we rode pretty fast. For the purpose of illustration I recorded everything I did and ate on the second day, which I rode a bit easier than the first day.
The second ride took 6 hours and 5 minutes. My average normalized power output was 225 watts, and arithmetic average power output was 184 watts. Based on mechanical work output, this required about 5,000 kcal. Factoring in the other 18 hours of that day, my total energy expenditure was about 6,800 kcal for the day, obviously not an average day. (A detailed explanation of where the extra 1,800 kcal were expended is beyond what I want to get into now, but it’s basically the energy required to keep me alive – transport ions, contract voluntary and involuntary muscles, etc. — plus move me around, and digest food).
So what did I eat that day?
- Breakfast (pre-ride): 5 scrambled eggs, 2 sausage links, 3 pieces of bacon, coffee with cream.
- In ride nutrition (I spread this out over 6 hours): 14 oz (not a typo) of salted cashews, 2 Quest bars, 1 peach, 1 apple, 6 bottles of Biosteel High Performance Sports Drink, water. (Since I know someone will ask, I did not consume super starch this day since I was craving cashews as my carbohydrate source and was craving more sodium, given the 90+ degree temperature.)
- Late lunch/early dinner (post-ride): 2 oz ham, 3 oz pulled pork, large salad with oil and vinegar dressing, 2 slices of cheddar cheese, 6 mini hamburger patties, 2 tomatoes.
What did this amount to?
- Fat – 351 gm, or 3,160 kcal of fat
- Protein – 245 gm, or 980 kcal of protein
- Carbohydrate – 321 gm, or 1,284 kcal of carbohydrate
(I used package information and Nutritionist Pro software to calculate this.)
Hence, on this day I consumed about 5,400 kcal in total at the following ratio:
- Fat – 58%
- Protein – 18%
- Carbohydrate – 24%
By all conventional wisdom I should not have been in ketosis the next morning, right?
The following morning, my BHB level was 2.2 mM and blood glucose was 5.1 mM.
Teaching point I can’t resist: Following 2 days of significant caloric deficit, about 3,000 kcal in total, I should have in theory lost about a pound (mostly fat, possibly some muscle) which would have been noticed on a scale. Instead, I gained 8 pounds over those 2 days! Sure it was mostly water retention, both from the glycogen (small) and the fluid accumulating in the interstitial space (“thirds space” fluid losses, large) due to a systemic inflammatory response. This happens under extreme conditions of exercise. In fact, the harder I exercise, the more weight I gain, transiently. I am at my absolute lightest following 2 days of travel (i.e., rest). So before freaking out at the sight of the scale, keep in mind that most day-to-day weight movement in our bodies is indeed water movement into and out of the plasma and interstitial space, respectively.
What’s my point?
Context matters! If I ate even one-quarter of that amount of carbohydrate and two-thirds of that protein on a normal day – say, 2.5 hours of riding or 1.5 hour of riding followed by 1 hour of swimming, or a day of travel with no exercise – I would have been out of ketosis for two days or more. (Of course, my appetite on those days would not have allowed me to eat 5,400 kcal without feeling sick, but I won’t get into that until a later post.) But on this day, with these glycogen demands, I was able to maintain the perks of ketosis AND glycolysis simultaneously.
There are days, though, when I overshot my glycogen need and end up with a low BHB and high fasting glucose the following morning. Conversely, there are days I underestimate my glycogen depletion and wake up with very high BHB levels and very low glucose levels (i.e., BHB levels higher than glucose levels, when both measured in mM).
Final thoughts
I felt a bit like I was in unchartered territory because the literature on nutritional ketosis hadn’t really (to my reading) explored this level of extreme activity. In future posts, I may write about other experiences and self-experiments, including my experience with exogenous (i.e., synthetic) ketones (which I did not use on this ride, but have experimented with on other rides – no, this is not “raspberry ketones” or other such gimmicks).
2017: You can read about one of my earliest experiences with exogenous ketones in this post.
Are carbohydrates necessary to produce 225 watts or more for hours on end? Yes. But, the key is knowing how much you need and when to take them. A lower RQ at a given level of intensity means less demand on glycogen. In my experience, working with athletes and non-athletes, most tend to make two errors (for lack of a better word):
- They over-estimate their carbohydrate requirement, and/or
- They forget that no factor influences RQ – and therefore substrate requirement – more than dietary composition during lead up to event (or “life”, which is sort of the ultimate event).
Know your engine, first. Then fuel it appropriately.



