
I embarked on a self-experiment last weekend to see if I could better understand the interplay between the different types of exercise I do and ketone production (beta-hydroxybutyrate, or B-OHB, to be specific). To be clear, nothing I do with a sample size of one “proves” anything, but sometimes self-experiments can help you formulate hypotheses and, if nothing else, understand how your body works. Consider the parable of the black sheep. If you see even a single black sheep in the field, depending on your field of training, you can draw conclusions:
Three scientists were on a train and had just crossed the border into Scotland. A black sheep was grazing on a hillside. The biologist peered out of the window and said, “Look! Scottish sheep are black!” The chemist said, “No, no. Some Scottish sheep are black.” The physicist, with an irritated tone in his voice, said, “My friends, there is at least one field, containing at least one sheep, of which at least one side is black some of the time.”
My point is, even a self-experiment of one can be good for something.
To test the relationship between exercise and ketosis I decided to examine my blood levels of glucose, B-OHB, and lactate immediately before and after three different types of workouts on three successive days. This interplay is complex and no one knows “everything” about it, including the world’s experts (which I am not pretending to be). I’m going to try to balance a fine line in this post – I want to be rigorous enough to explore the ideas with substance but not too detailed to put you to sleep. I hope I am able to balance these forces adequately.
If any of you are not familiar with the work of Jeff Volek and Steve Phinney, but you are interested in the biochemistry of nutritional ketosis, I recommend getting familiar with their work. The list of people who know more about nutritional ketosis is short.
Let’s take a look at the three parameters I measured in a bit more detail. To give you a sense of what is “normal” here are some guidelines:
Glucose
A normal fasting glucose is generally considered to be between 75 and 100 mg/dL. My mean over the past year has been about 90, but I need to mention two very important caveats:
- On the four occasions I have calibrated my hand-held device with an actual laboratory test, my device seems to run high by about 11 mg/dL, so a measurement of 95 mg/dL on my device is probably closer to 84 mg/dL in reality.
- I carry a genetic trait for a disease called beta-thalassemia. The clinical manifestation of this is that I have much smaller red blood cells than normal (about 65% of normal size). There is some evidence in the literature that this condition prevents some accurate testing of any assay that can interfere with hemoglobin. For example, a test measuring glycosylated hemoglobin suggests I have much more glucose in my blood than is actually measured. In fact, the Glycomark test for mean post-meal glucose level suggested I have an average post-meal glucose level of 190 mg/dL which is obviously not true. In other words, something about my beta-thalassemia seems to interfere with, at the very least, measuring glucose linked to hemoglobin, and possibly measuring glucose in general.
I mention these 2 features to say my glucose levels (unlike B-OHB and lactate which I’ve documented to be very accurate) may be artificially elevated. Here’s the important part, though: the discrepancy seems to be constant, so the increases or decreases seem to be good measurements.
Beta-Hydroxybutyrate (B-OHB)
A normal fasting B-OHB level for a “normal” (i.e., non-ketotic) person is zero. Within a day of fasting, you might expect this number to reach 0.2 to 0.4 mM, and about 1.0 mM within 48 to 72 hours of complete fasting, though this is highly variable among subjects.
If you’ll recall from my discussion of keto-adaptation, the threshold for nutritional ketosis is about 0.5 mM. My normal morning fasting level of B-OHB is usually between 1.0 and 2.0 mM with an arithmetic mean of about 1.4 mM.
Both insulin and glucose (probably by causing the secretion of insulin) suppress ketones. This is why, for example, consuming more than about 50 gm of carbohydrates per day and/or more than about 120-150 gm of protein per day makes it difficult to be in nutritional ketosis – too much insulin secretion.
Lactate
Lactate (or lactic acid) is a byproduct of anaerobic exercise. A normal level is considered to be below 2.2 mM. Basically (I’m oversimplifying a bit), when you exercise in a predominately aerobic capacity, while you do generate lactate your liver is able to match muscle production with clearance via a process called the Cori Cycle (a process in which the liver turns lactate back into glucose).
If you’ve ever done a very intense exercise – like run an all-out mile – and felt like your body is completely seizing up and you are unable to move, you’ve experienced a high lactate. Technically, the lactate is not causing this. Lactate gets a pretty bad rap, and it’s actually a good thing as it allows us to generate energy even when we demand it in an environment where sufficient cellular oxygen is absent. The real “bad guy” is the hydrogen ion that accompanies lactate and interferes with the ability of our muscles to contract and relax properly. However, we use lactate as a proxy for the hydrogen that is actually causing the pain and difficulty in muscle contraction.
For me (personally, though this is probably true for most people) the highest lactate I generate tends to be in all-out activities lasting about 2 minutes which use all muscles in my body (the more muscles you use, the more lactate you generate). Hence, the 200 individual medley (IM) race generates the most lactate in my body: It’s 2-plus minutes of maximum exertion sending pain into every muscle in my body (this event requires a swim, in order, of 50 yards each of all-out butterfly, then backstroke, then breaststroke, then freestyle). A runner would probably concur that the 800 meter (half-mile) run is one of the most painful races in that sport.
The highest lactate I have ever measured in myself, following a 200 IM race, was about 16 mM. I have measured higher levels in several Olympic swimmers, including 20.2 mM in one (as he was vomiting all over the pool deck – for reasons I’ll try to remember to explain in a subsequent post). On my bike, where I’m mostly using my legs, obviously, I think my highest recorded lactate measurement was about 12 or 13 mM following a set of ten 2-minute all-out hill repeats.
I measure my lactate levels using a different hand-held device from the one that measures glucose and B-OHB.
[Another parable, this time about marriage: 2 years ago my father asked me what my wife and I wanted for Christmas. I said “we” wanted a lactate meter with about 200 test strips (I think it was about $900 for everything). He looked at me funny, but figured I knew what I was talking about. When Christmas rolled around and “we” got “our” lactate meter I had to spend a few minutes explaining to my wife why this was a perfect gift for “us” as it allowed “us” to spend lots of time together while she pricked my finger for blood during my workouts. She didn’t really agree with me. I clearly don’t understand women very well – I really thought she would find this device “cool.” Which is why this is a blog about health, not marriage.]
Results from my experiment
Day 1: Saturday (hard swim workout, race pace)
This was a one hour, 45 minute swim with warm-up and cool down. The “main set” was mostly freestyle and butterfly at all-out race pace for distances of 25, 50, 75, and 100 yard intervals with long rest (1:2 – 2 times more rest than swim time) for the all-out 100 yard swims, and modest rest (2:1 – half the rest time of each swim). The single most demanding aspect of this workout took place with about 25 minutes remaining and, though I didn’t measure peak lactate, I suspect it was around 12-14 mM, based on the discomfort I experienced. I was surprised that my lactate level was still as high as it was (see below) 25 minutes later, though I suspect I didn’t cool down as gingerly as I should have, to optimize for maximum lactate clearance.
During this workout I consumed nothing and prior to the workout I consumed my usual 40 mL of medium chain triglyceride (MCT) oil.
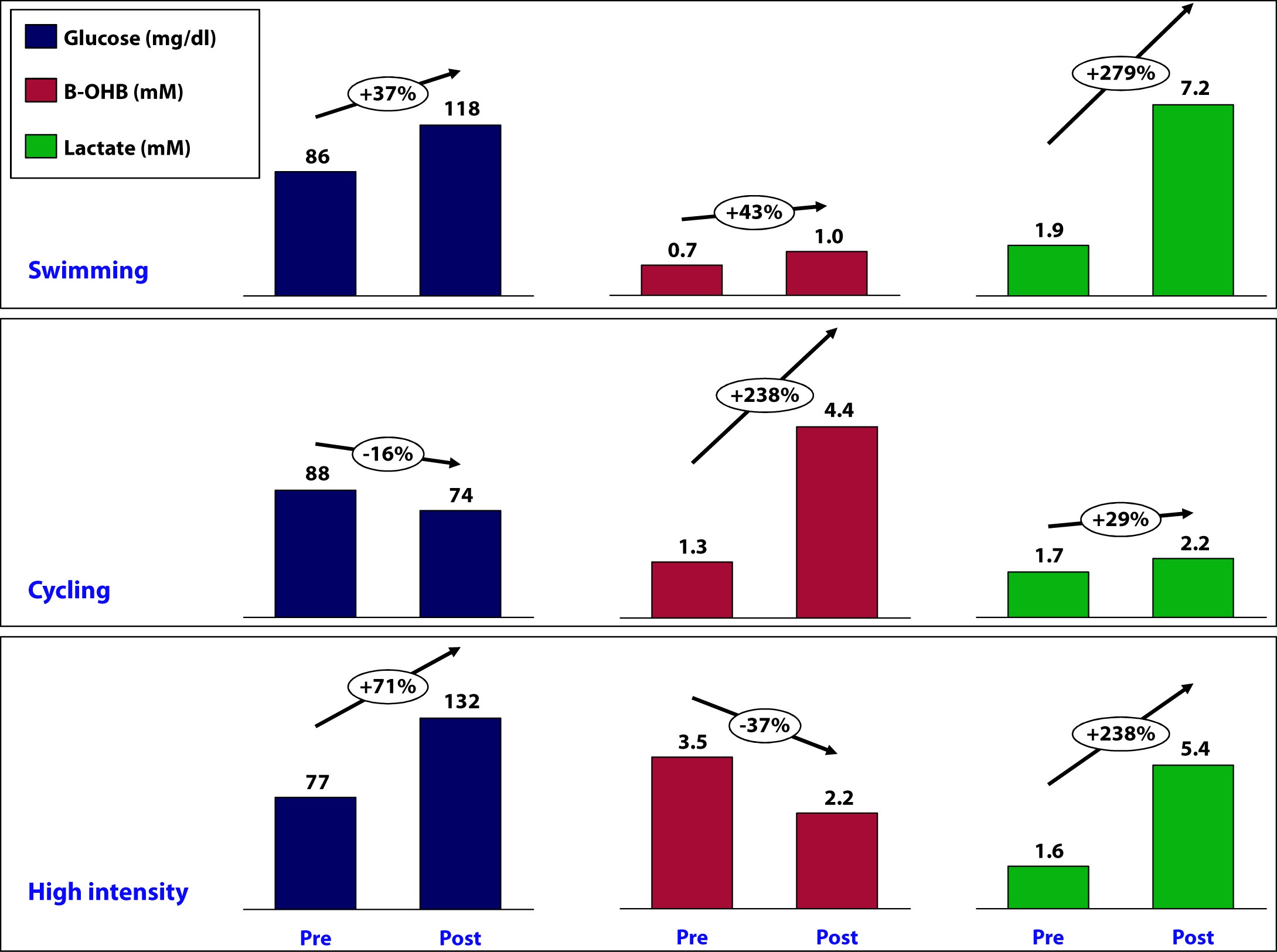
At 7:29 am, just before beginning the workout, my glucose was 86 mg/dL, B-OHB was 0.7 mM (which is low for my fasting level), and lactate was 1.9 mM.
Immediately post-workout, at 9:14 am, my glucose was 118 mg/dL, B-OHB was 1.0 mM, and lactate was 7.2 mM.
Day 2: Sunday (long ride, 80% of race pace)
This was a tempo ride covering 104 miles (167 km) with 5,600 feet of climbing. Average pace was 17 mph (about 28 km/hr) with lots of headwind. My average HR over this 6 hour ride was 141 and average power output was between 190 and 200 watts. There were many sections of the ride, particularly on the climbs, where my HR was sustained in the 160’s for 30 minute stretches and power output was above 275 watts (which, for me, means my muscles generate lactate faster than my liver can clear it).
During this workout I consumed the following:
- Two single-serving packets (1 oz) of cream cheese (14 gm fat; 2 gm carb; 2 gm protein)
- 50 gm of super starch, by Generation UCAN mixed in my water bottles (50 gm super starch which, technically, is a carb but does not behave like one with respect to insulin secretion and ketone suppression – I will write a dedicated post on super starch in the future, but if you must try it now, use this code to get a discount: “UCANPA”)
- 2.5 oz of mixed nuts (25% of each almonds, cashews, walnuts, peanuts – 36 gm fat; 14 gm protein; 15 gm carb)
Total intake during 6 hour ride, therefore, was: 50 gm fat; 16 gm protein; 67 gm carb (of which 50 gm was super-starch), for a total of about 750 calories.
About 90 minutes prior to the ride I consumed 4 eggs fluffed with heavy cream, cream cheese, coffee with heavy cream, and my usual 40 mL of MCT oil.
At 7:56 am, my glucose was 88 mg/dL, B-OHB was 1.3 mM, and lactate was 1.7 mM.
Immediately post-ride, at 2:39 pm, my glucose was 74 mg/dL, B-OHB was 4.4 mM, and lactate was 2.2 mM.
Day 3: Monday (dry-land, high intensity training)
On this particular day, it was raining (one of 3 days a year this happens in San Diego), so I did not do the outdoor stuff (including tire flips).
Prior to the workout I consumed nothing other than my usual 40 mL of MCT oil and during the workout I consumed about 4 gm of branched chain amino acids (BCAA) and 10 gm of super starch mixed in my water bottle – so essentially just water.
Immediately prior to the workout, at 6:43 am, my glucose was 77 mg/dL, B-OHB was 3.5 mM*, and lactate was 1.6 mM.
At 7:52 am glucose was 132 mg/dL, B-OHB was 2.2 mM, and lactate was 5.4 mM.
*If you’re wondering why my fasting B-OHB level was so high (recall, I’m usually between 1.0 and 2.0), I suspect it’s at least a partial result of 2 things:
- Residual fat breakdown from the previous day’s long ride and caloric deficit, and
- On Sunday night I ate (no exaggeration) about half a gallon of my wife’s famous zero sugar, high fat coffee ice cream, which must be the closest thing I’ve ever experienced to heroin in terms of addiction potential.
Summary
The figure below summarizes the data from the mini-self-experiment I just described.
What can we learn about the interaction between glucose, B-OHB, and lactate?
How does super starch impact my ketosis?
Is ketosis helping me or hurting me?
Stay tuned for next week, when I will try to interpret these results…



