In this episode, David Sinclair, Ph.D., a Professor in the Department of Genetics at Harvard Medical School and co-Director of the Paul F. Glenn Center for the Biological Mechanisms of Aging, returns to the podcast to discuss the content of his new book, Lifespan: Why We Age – and Why We Don’t Have To. This conversation focuses on the biological mechanisms involved in what David terms the Information Theory of Aging which provides insights into the “clock” that determines our aging and to what degree it can be manipulated. Our discussion on aging of course leads us into interconnected topics of epigenetics, sirtuins, cellular senescence, as well as what compounds David is personally taking for his own longevity. Additionally, we discuss the most up to date information related to NAD and longevity by looking at the potential benefits (if any) of supplemental agents (NAD precursors, NR, NMR, etc.) that pose a promise of increasing NAD.
Subscribe on: APPLE PODCASTS | RSS | GOOGLE | OVERCAST | STITCHER
We discuss:
- SIR genes and cellular identity [8:45];
- Sirtuins regulate gene expression [14:30];
- DNA is methylated at the deepest layer of the epigenome [17:45];
- Methylation pattern and determining cellular age [20:15];
- Cellular reprogramming [33:45];
- Yamanaka factors to push cells “back in time” [41:00];
- Human cellular reprogramming viability [57:00];
- Measuring the rate of aging [1:02:45];
- Cellular reprogramming for longevity [1:14:45];
- Compounds David takes for his own longevity [1:29:15]
- NAD precursors (NR, NMN) and pterostilbene [1:40:00];
- The current field of sirtuin activators [2:03:15];
- David’s artistic work [2:05:15] and;
- More.
Get Peter’s expertise in your inbox 100% free.
Sign up to receive An Introductory Guide to Longevity by Peter Attia, weekly longevity-focused articles, and new podcast announcements.
SIR genes and cellular identity [8:45]
The SIR gene – silent information regulator – is a gene that controls other genes
- One of the roles it is most well-known for, is its implication in longevity: In a study by Matt Kaeberlin Sir2 was shown to control the aging process in yeast
- The gene group’s primary roles are to:
- Silence other genes
- Repair damaged DNA
The SIR enzyme is the master regulator of this cellular survival circuit
- The SIR gene cannot silence other genes and serve a cellular repair function at the same time
- silenced genes are temporarily “turned on” while the damage is repaired by the enzyme protein
- “turned on” genes help with the repair
- the protein then returns to its “silencing post”
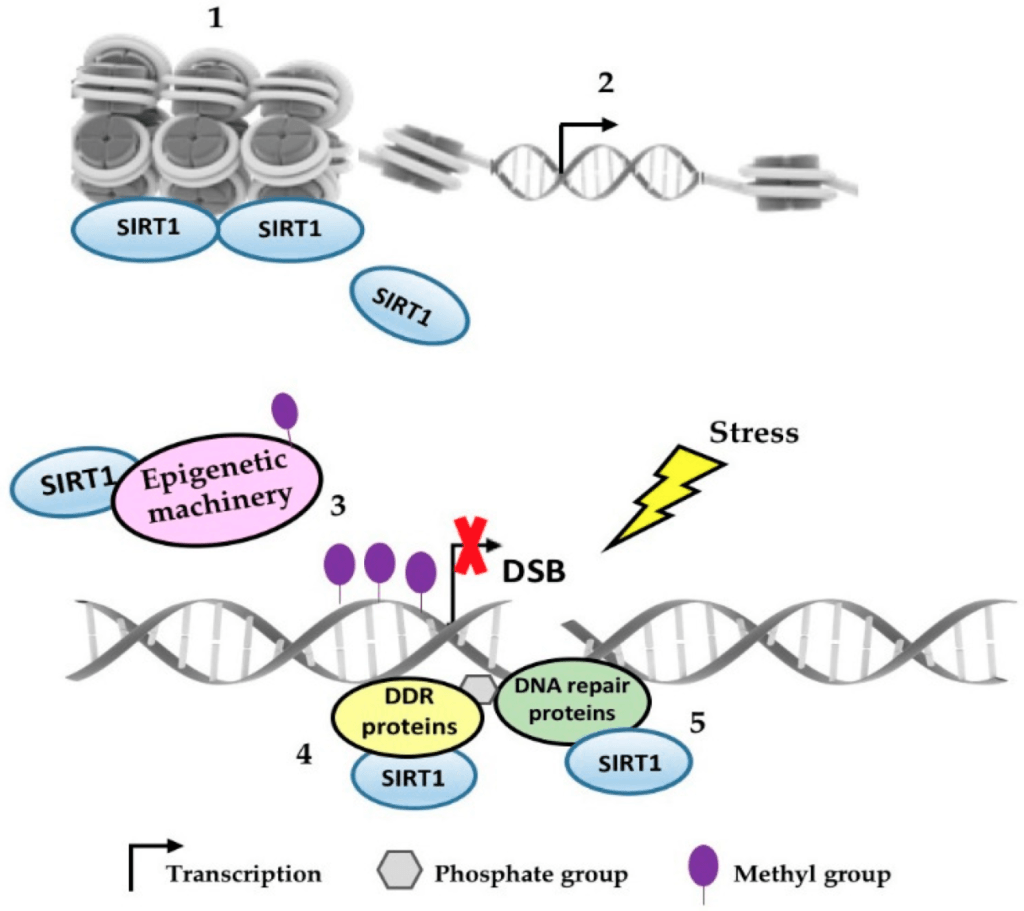
Figure 1. When SIR enzyme proteins detect stress in the cell (e.g. DNA breakage) the protein leaves the silent region to go and repair the DNA. When the problem is fixed, it returns to its original post, silencing genes. Image credit: (Alves-Fernandes and Jasiulionis, 2019)
Overtime, in the back-and-forth of repair… SIR genes lose track of which genes should be silenced or not
- In aging yeast, the loss of cellular identity results in a sterility phenotype
- With age, our cells lose their “program” but early evidence in mice suggests that the original “hard disk program” can be recovered; restored to the original programming
“We have some early evidence from mice that we can actually find that hard disk drive and reinstall the software so that it’s pristine again and we find that we can actually improve the health quite dramatically in parts of a mouse’s body.” — David Sinclair, Ph.D
What does Claude Shannon’s Information Theory of Communication have to do with aging?…
- In his 1940 paper, mathematician Claude Shannon presented his Information Theory of Communication
- He presented how to encode information and make sure that information gets to the receiver
- Shannon figured out how to preserve information: make a repository and reset the system
{end of show notes preview}
Would you like access to extensive show notes and references for this podcast (and more)?
Check out this post to see an example of what the substantial show notes look like. Become a member today to get access.

David Sinclair, Ph.D.
David A. Sinclair, Ph.D. is a Professor in the Department of Genetics at Harvard Medical School and co-Director of the Paul F. Glenn Center for the Biological Mechanisms of Aging.
He is best known for his work on understanding why we age and how to slow its effects. He obtained his Ph.D. in Molecular Genetics at the University of New South Wales, Sydney in 1995. He worked as a postdoctoral researcher at M.I.T. with Dr. Leonard Guarente where he co-discovered a cause of aging for yeast as well as the role of Sir2 in epigenetic changes driven by genome instability. In 1999 he was recruited to Harvard Medical School where his laboratory’s research has focused primarily on understanding the role of sirtuins in disease and aging, with associated interests in chromatin, energy metabolism, mitochondria, learning and memory, neurodegeneration, and cancer. He has also contributed to the understanding of how sirtuins are modulated by endogenous molecules and pharmacological agents such as resveratrol.
Dr. Sinclair is the co-founder of several biotechnology companies (Sirtris, Ovascience, Genocea, Cohbar, MetroBiotech, ArcBio, Liberty Biosecurity) and is on the boards of several others. He is also co-founder and co-chief editor of the journal Aging. His work is featured in five books, two documentary movies, 60 Minutes, Morgan Freeman’s “Through the Wormhole” and other media.
He is an inventor on 35 patents and has received more than 25 awards and honors including the CSL Prize, The Australian Commonwealth Prize, Thompson Prize, Helen Hay Whitney Postdoctoral Award, Charles Hood Fellowship, Leukemia Society Fellowship, Ludwig Scholarship, Harvard-Armenise Fellowship, American Association for Aging Research Fellowship, Nathan Shock Award from the National Institutes of Health, Ellison Medical Foundation Junior and Senior Scholar Awards, Merck Prize, Genzyme Outstanding Achievement in Biomedical Science Award, Bio-Innovator Award, David Murdock-Dole Lectureship, Fisher Honorary Lectureship, Les Lazarus Lectureship, Australian Medical Research Medal, The Frontiers in Aging and Regeneration Award, Top 100 Australian Innovators, and TIME magazine’s list of the “100 most influential people in the world”. [medapps.med.harvard.edu] His new book, Lifespan, explains why we age and why we don’t have to.
David on LinkedIn: David A. Sinclair, Ph.D. A.O.
David on Twitter: @davidasinclair
David on Instagram: davidsinclairphdDavid’s book website: lifespanbook.com



