Keith Flaherty is the director of clinical research at the Massachusetts General Hospital Cancer Center and a previous guest on The Drive. In this episode, Keith first delves into the statistics on cancer’s prevalence as we age, underscoring the significance of finding effective treatments and early detection methodologies. He touches on the history of cancer therapeutics and illuminates the notable enhancements in cancer therapy within the last decade that are setting the stage for a promising future. He goes into detail on the potential of immunotherapy and therapies that can combat cancer’s evasive tactics while explaining some of the existing challenges around specificity, cost, and scalability. Additionally, Keith highlights the significant leap in early detection methodologies, namely liquid biopsies, which have the potential not only to determine if a cancer is present in an early stage, but also identify the possible tissue of origin.
Subscribe on: APPLE PODCASTS | RSS | GOOGLE | OVERCAST | STITCHER

We discuss:
- Keith’s interest and expertise in cancer [3:15];
- Cancer deaths by decade of life, and how cancer compares to other top causes of death [7:00];
- The relationship between hormones and cancer [12:00];
- The link between obesity and cancer [18:45];
- Current state of treatments for metastatic cancer and reasons for the lack of progress over the decades [22:30];
- The interplay between the immune system and cancer cells [32:00];
- Different ways cancer can suppress the immune response, and how immunotherapy can combat cancer’s evasive tactics [39:30];
- Elimination of a substantial portion of cancers through immune cell engineering faces challenges of specificity, cost, and scalability [52:15];
- Why TIL therapy isn’t always effective, and the necessity for multimodality therapy to address various aspects of the cancer microenvironment [1:01:00];
- The potential developments in cancer therapy over the next five years: T-cell activation, metabolic interventions, targeting tumor microenvironments, and more [1:06:30];
- The challenge of treating metastatic cancer underscores the importance of early detection to improve survivability [1:19:15];
- Liquid biopsies for early detection of cancer and determining the possible tissue of origin [1:24:45];
- Commercially available cancer screening tests [1:33:45];
- How to address the disparity in cancer care, and the exciting pace of progress for cancer detection and treatment [1:40:15]; and
- More.
Get Peter’s expertise in your inbox 100% free.
Sign up to receive An Introductory Guide to Longevity by Peter Attia, weekly longevity-focused articles, and new podcast announcements.Keith’s interest and expertise in cancer [3:15]
A lot has happened in the past four years
- In therapeutic development, maybe you could have said four years ago that some of the things that have played out would have played out
- But on the diagnostic side, Keith didn’t quite have the crystal ball vision as to how things would develop there
- Those two areas are tightly related in oncology
Give folks a short background, a little bit about what you’re doing and why you are in a great position to talk about the field of cancer [4:15]
- Keith is a medical oncologist whose been in the field for 23 years
- The first translation of molecular insights (specifically genetic insights into cancer biology) really became therapy 23 years ago
- That’s when Imatinib (or Gleevec) was first used in patients and was a revolutionary moment
- Keith’s career started right then and there as a medical oncologist
- His focus has been trying to translate science to medicine in very much that way, taking insights in terms of the genetic makeup (like the mutational architecture of cancers) and trying to translate that understanding into therapy
- Like anybody in the academic medical world and oncology, he focused on specific cancer types ‒ melanoma and kidney cancer
- He chose both of those because of the molecular insights that existed at the time felt like they were beginning to be ripe for translation
- Keith did that work for about a decade at University of Pennsylvania
- Then he moved to Mass General to build a clinical program focused on therapeutic development much more broadly across cancer
- Part of the Harvard Medical School umbrella
- He built a translational research group surrounding therapeutic development on this interplay between therapeutics and molecular understanding and diagnostics
- It’s what he refers to as, “bedside-to-bench translational research”
- The goal is to understand mechanisms of action and mechanisms of resistance
- In other words, when drugs work, why?
- And if they don’t work, why not?
- Then use those insights to try to accelerate or drive the whole process forward
- Over the past 10 years, he’s co-founded a handful of biotech companies
- Loxo Oncology being the first 10 years ago, and that was acquired four years ago
- Scorpion Therapeutics being the most recent, where he sits in the offices of Scorpion Therapeutics
- Through those channels, it’s his job to keep a steady eye on new therapeutic concepts that could be ready for primetime and then trying to translate his understanding into tools that we can actually use for real patients (such as diagnostics)
Cancer deaths by decade of life, and how cancer compares to other top causes of death [7:00]
- Peter points out, “There’s something about cancer that’s particularly damning, which is when you look at the other two chronic diseases that are huge killers, which are cardiovascular disease and neurodegenerative disease, they increase in their severity exponentially as you age. They don’t really become a dominant source of mortality until people are in the seventh and eighth decade of life, and that’s not true for cancer.”
- Our analysts put together the table below of the % people that die from cancer in 10-year increments
- What’s interesting is that number peaks in the middle
- At age 25-34, its 6%
- At age 35-44, it’s 13% and that’s a staggering number for people so young
- At age 45-54, it’s 23%
- At age 55-64, it’s 30%
- At age 65-74, it’s 31%
- Then, paradoxically, it begins to come down because those other diseases are taking off
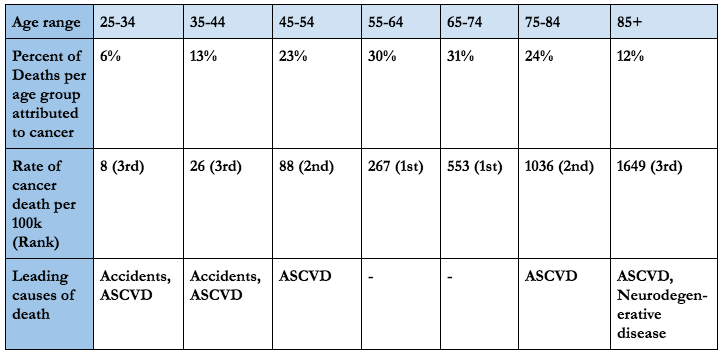
Figure 1. Percentage of people that die from cancer in 10-year increments.
- Another way to look at this is, where does cancer rank in cause of death for all causes by decade?
{end of show notes preview}
Would you like access to extensive show notes and references for this podcast (and more)?
Check out this post to see an example of what the substantial show notes look like. Become a member today to get access.

Keith Flaherty, M.D.
Keith Flaherty earned his Bachelor of Science from Yale University. He earned his medical degree from Johns Hopkins University, completed his residency in internal medicine at Brigham and Women’s Hospital, and completed a medical oncology fellowship at the University of Pennsylvania. Dr. Flaherty began his career as a Professor of Medicine at the University of Pennsylvania. Currently he is a Professor of Medicine at Harvard Medical School where he is the Richard Saltonstall Endowed Chair in Oncology. He also serves as the Director of Henri and Belinda Termeer Center for Targeted Therapy, Cancer Center, Massachusetts General Hospital, and Director of Clinical Research, Cancer Center, Massachusetts General Hospital. At Dana-Farber/ Harvard Cancer Center he serves as the co-leader of the developmental therapeutics program, and he is a member of the melanoma research program.
Dr. Flaherty has expertise in melanoma. His research focuses on understanding novel, molecularly targeted cancer therapies and predictive biomarkers. Dr. Flaherty and colleagues have established the efficacy of inhibiting BRAF and/or MEK for treating metastatic melanoma. He has also been a leader in characterizing mechanisms of resistance to BRAF inhibitor therapy. Dr. Flaherty has served as Principal Investigator for numerous clinical trials of novel cancer therapies.
Dr. Flaherty joined the NCI Board of Scientific Advisors in 2018 and AACR Board of Directors in 2019. He serves as editor-in-chief of Clinical Cancer Research. Dr Flaherty has co-founded and served as an advisor for several biotech companies. In 2013 Dr. Flaherty co-founded Loxo Oncology, served on the Board of Directors, and chaired the Scientific Advisory board until its acquisition by Eli Lilly for $8 billion. He is co-founder of Strata Oncology, X4 Pharmaceuticals, Apricity, and Scorpion Therapeutics. He serves on the board of directors of Loxo Oncology, Inc. and Chair of Clinical Advisory Board for Monopteros Therapeutics. [Monopteros]