As we get older, the age-related decline in muscle mass and strength – known as sarcopenia – is one of the major impediments to performing the tasks of daily living, such as getting in and out of bed, shopping, walking, and preparing meals. Depending on your age, sarcopenia may seem like a concern for the distant future, but the declines in muscle quality begin earlier than many realize, with metrics such as muscle strength and power (strength multiplied by the speed of movement) starting to decline around age 40. Movements requiring strength and power recruit type II muscle fibers, which are known to atrophy with age more rapidly than type I (endurance-type) muscle fibers. In fact, the atrophy (shrinking) of these most powerful type II muscle fibers may be one of the most critical hallmarks of aging.
Yet despite the trends of muscle aging at the population level, this process may not be as inevitable for any given individual as it might seem. A recent study tested whether heavy resistance training could reverse some of the age-related cellular-level changes in skeletal muscle that are generally considered irreversible.
Cellular level changes in aging muscle
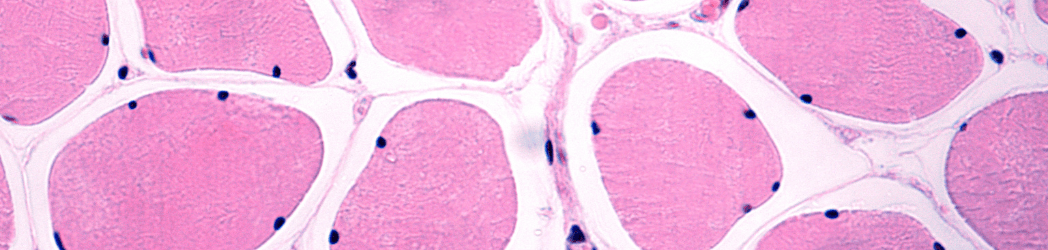
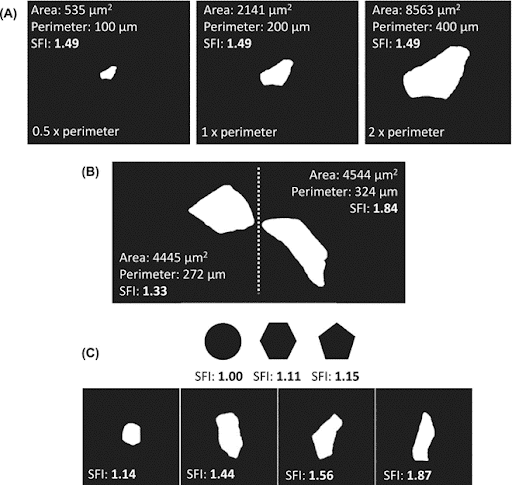
In cross-section, healthy skeletal muscle fibers are tightly packed and form a tessellation, with each fiber taking the approximate shape of a pentagon or hexagon. However, as a muscle fiber atrophies, it tends to take on a more complex and often elongated shape in cross-section. One of the ways to quantify the irregularities in shape is with a “shape factor index” (SFI), which calculates the ratio of the fiber’s perimeter to the fiber’s cross-sectional area. The SFI of a perfect circle is one, whereas an oval with the same area as the circle will have an SFI greater than one. This metric quantifies the deformity of the shape of muscle fibers in cross-section (with higher numbers corresponding to greater deformity) but does not account for the overall size of the fiber (see panel A in the Figure below). Instead, the SFI distinguishes two fibers of similar cross-sectional areas with different levels of deformity (see panels B and C).
Muscle fiber deformity correlates with age
This study used quadriceps muscle biopsies from 197 individuals, who were largely physically inactive, to quantify the deformities in the muscle fiber shape of both type I and type II fibers and assess age-related trends in performance and cellular morphology. For analysis, participants were separated into three groups by age – young (20-36 years), old (60-79), and oldest old (81-97).
In the evaluation of the muscle biopsies, mean SFI exhibited a significant increase across increasing age groups for both type I and type II muscle fibers, demonstrating that the measurement of myofiber shape distortion increases with advancing age, regardless of muscle fiber type. However, the age-related increase in SFI was greater in type II fibers than in type I fibers, and the mean SFI was higher in type II fibers than in type I fibers across all age groups, implying that the type II variety are even more susceptible to atrophy and deformity across an individual’s lifespan than type I fibers. Indeed, compared to the young group, the old and oldest-old groups respectively had a 6.2% and 13.6% higher SFI in type II muscle fibers. Additionally, type II fiber SFI was an independent predictor of overall muscle size (as measured by the cross-sectional area of the quadriceps) and muscle strength (as measured by isometric and isokinetic maximal voluntary contractions).
The effect of resistance training
A subset (n=59) of this cohort then participated in heavy resistance training, which consisted of supervised training three times per week. Since the study aimed to evaluate changes in the quadriceps muscle, only leg exercises were required as resistance training. Training included a 5-min warm-up of low- to moderate-intensity cycling, followed by 3-5 sets of 8-15 repetitions of leg press, leg extension, and leg curl, as well as two optional upper body exercises. These exercises were performed using the maximal weight possible while still completing the 8-15 repetitions. When a participant achieved a target number of repetitions at a given load, the load for that exercise was continuously increased. After 3-4 months of this training protocol, a second muscle biopsy was taken from these individuals.
Compared to baseline, both the young and old groups had a 3-4% decrease in average SFI of type II fibers post-training – a significant change and a partial reversal of the age-related trend. Though no participants in the “oldest old” group were part of the resistance training intervention, the finding that young and old groups experienced similar reductions in type II fiber SFI from suggests that age may not compromise the ability to improve muscle quality through resistance training as much as previously thought – which in turn would imply that “age-related” decline in muscle quality is not as unavoidable as previously thought and more likely reflects a decline in muscle use. (This would also explain why type I fibers see a more modest age-associated increases in deformity, given that these fibers are more important for movements in daily life activities and thus are less likely to be subject to steep declines in use). Furthermore, though 3-4 months of training did not bring the old group quite to the level of the young group’s baseline values, it’s possible with a longer training history, they might experience even more adaptation and further diminish the difference in SFI of type II myofibers between these two groups.
Adding further support for the “use it or lose it” concept of muscle decline, the investigators also tested a subset of muscle biopsies for the presence of a biomarker of myofiber denervation. Denervated myofibers had high SFI values, and the presence of denervated myofibers increased with age, which supports the hypothesis that the deformities in myofiber shape may occur after the loss of motor neuron innervation.
The importance of resistance training at any age
It is well known that, on a population level, type II muscle fibers atrophy with aging and inactivity. However, it is not clear to what degree these age-related changes might be avoidable. I find myself, personally, unconvinced that the magnitude of decline we see at the population level is biologically inevitable. Rather, I believe it is driven more by a vicious cycle of inactivity and deconditioning.
This study provides additional context about how a lack of use, particularly of type II fibers, translates into motor neuron denervation, leading to atrophy and deformity in the muscle fibers. Yet mechanical loading through resistance training stimulates muscle fiber recruitment, which at least partially reverses some of the age-related trends. Similar findings were demonstrated in another recent study of master sprinters (ages 40-85) who, over the 10-year follow-up, showed no change in quadriceps fiber composition or fiber cross-sectional area (meaning no fiber atrophy) as long as they continued their sprint training. Sprinting, like resistance training, also heavily recruits type II muscle fibers, suggesting that consistent training of these fibers is the key to reducing their atrophy as we age.
Remarkably, the reduction in SFI in type II fibers after resistance training was seen across all age groups, as was the higher level of deformity in type II fibers compared to type I fibers. Although older adults had higher SFI and accompanying denervation, these observations imply that this slow decline starts from disuse earlier in life. Training (and maintaining training) throughout life may be a way to minimize what is popularly misconceived to be unavoidable. And while the resistance training intervention in this study was limited to people younger than 80 years of age, there is no reason to think that resistance training wouldn’t be able to stimulate similar changes in people of even older ages, since resistance training is known to increase strength and hypertrophy at any age.
The bottom line
Exercise, and in particular resistance training, is one of the most effective ways to combat sarcopenia, and the so-called “age-related” declines in muscle composition are not as unavoidable as many might assume. The results of this study demonstrate that heavy resistance training creates gross adaptations to skeletal muscle in the form of strength and hypertrophy and suggest that the irregular shape of atrophied muscle fibers is a hallmark of insufficient stimuli more than chronological age alone. Older muscle still responds to resistance training, proving again that it’s never too early or too late to start reaping the benefits of this crucial strategy for preventing muscle losses with age. Show me a 90-year-old who says, “Gee, I wish I had less muscle mass” and I’ll show you a leprechaun at the end of a double rainbow riding a unicorn kissing a mermaid.
For a list of all previous weekly emails, click here.


