In this special episode of The Drive, we have pulled together a variety of clips from previous podcasts about cardiovascular disease to help listeners understand this topic more deeply, as well as to identify previous episodes which may be of interest. In this episode, Peter highlights the importance of understanding cardiovascular disease and why early intervention is critical. He also provides a primer on lipoproteins and explains the fallacy of the terms “good cholesterol” and “bad cholesterol.” Allan Sniderman discusses the metrics measured in routine blood work – along with the limitations of those standard panels – before explaining why apoB is a superior metric for determining risk. Additionally, Tom Dayspring explains the causal role of apoB in atherosclerotic cardiovascular disease (ASCVD) and the therapeutic goals for apoB concentration, and Peter explains how early and aggressive lowering of apoB could change the landscape of cardiovascular disease prevention.
Subscribe on: APPLE PODCASTS | RSS | GOOGLE | OVERCAST | STITCHER
We discuss:
- The importance of understanding atherosclerosis early in life [2:25];
- Defining ASCVD, its causes, and the role of cholesterol [8:00];
- Why early prevention of atherosclerosis is critical [13:45];
- Preventing atherosclerosis—two fatal flaws with the “10-Year Risk” approach [16:00];
- Intro to lipids and lipoproteins: why there is no “bad” or “good” cholesterol [23:00];
- Limitations of standard blood panels [35:45];
- How Mendelian randomization is bolstering the case for apoB as the superior metric for risk prediction [39:30];
- Therapeutic goals for apoB concentration [58:15];
- How early and aggressive lowering of apoB could change the course of ASCVD [1:10:45]; and
- More.
Get Peter’s expertise in your inbox 100% free.
Sign up to receive An Introductory Guide to Longevity by Peter Attia, weekly longevity-focused articles, and new podcast announcements.
The importance of understanding atherosclerosis early in life [2:25]
From episode #203 – AMA #34: What Causes Heart Disease?; discussed from [2:20] – [8:00]
Atherosclerotic cardiovascular disease (ASCVD) is ubiquitous
- 1 – This disease is inevitable and ubiquitous
- 2 – It has a major impact on human longevity
“Not everybody dies from atherosclerosis, but… everybody dies with it”‒ Peter Attia
- Cancer and dementia are both prevalent with aging, but they are not inevitable
- We know a lot about ASCVD
- Peter adds, “The reason you really want to understand this is because the impact is huge and the tools we have are also huge”
Extending lifespan comes down to delaying the onset of chronic disease, and atherosclerosis is the most common chronic disease
2 main paths to atherosclerosis (risk factors)
- 1 – Hypertension (high blood pressure)
- 2 – Lipid abnormalities (we’ll focus on this one)
- Smoking is a behavioral risk factor (we’ll put this aside for the moment)
Studies of pathology show ASCVD begins at a young age
What is the most common presentation for a 1st heart attack?
- Sudden death
- A 1st heart attack in over 50% of people is fatal
- Today this number is a little less but still staggering
What is the age distribution of people who have their 1st major adverse cardiac event?
- Adverse cardiac events are a heart attack or a stroke (or death)
- Figure 1 shows the incidence of cardiovascular events for both males and females in the US
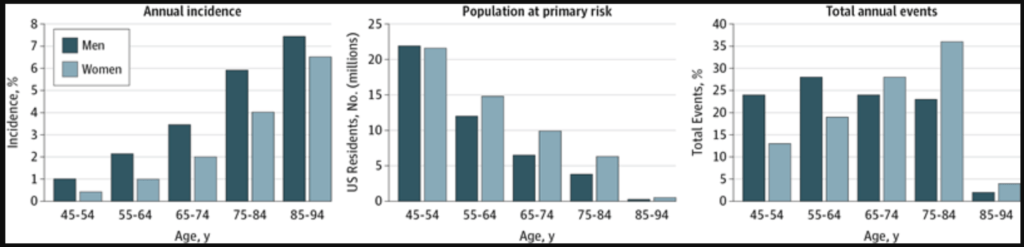
Figure 1. Incidence pf cardiovascular events by age and sex. Image credit: JAMA Cardiology 2016
- The graph on the right shows total annual events
- The 1st 2 sets of bars show the number of events for people under 65
- Men are shown in the darker bars comprising slightly below 25% and slightly above 25% of all cardiac events
- The implication is that 50% of men who are going to have a cardiac event in their life will have it before the age of 65
- For women, a third of women will have their 1st cardiac event before the age of 65
- The total annual events is not the whole story; it’s important to understand how long it takes for this disease to take hold
- Early prevention is key
- Almost 25% of these events are in men younger than 54
- When you think of someone who is 45, 50, this disease didn’t start 2 years before
When you see these stats laid out, it creates a shift in your mind around why you should care about this
Defining ASCVD, its causes, and the role of cholesterol [8:00]
From episode #203 – AMA #34: What Causes Heart Disease?; discussed from [9:00] – [15:00]
Atherosclerotic cardiovascular disease (ASCVD) is disease state characterized by the deposition or the buildup of cholesterol (sterols) in the artery wall
- It begins with a fatty streak that later consolidates into plaques that can ultimately lead to a reduction in blood flow
- Reduction in blood flow is called ischemia
- Ischemia results in tissue damage to the heart and this is what results in a heart attack
- A heart attack can be fatal depending on the amount of cardiac tissue that is damaged from loss of oxygenation
Causes of ASCVD
{end of show notes preview}
Would you like access to extensive show notes and references for this podcast (and more)?
Check out this post to see an example of what the substantial show notes look like. Become a member today to get access.



