Amanda Grant Smith is a geriatric psychiatrist with decades of experience treating patients with dementia and Alzheimer’s disease. In this episode, Amanda shares how she developed a passion for geriatric psychiatry as a means to support dementia patients. She explains how to recognize, define, and diagnose dementia—a process that still remains somewhat elusive. They also talk about the significance of ApoE genotype and compare the various forms of dementia including differentiating between Alzheimer’s disease and Lewy body dementia. They discuss the current landscape of clinical trials, the drug pipeline, and talk about a very promising monoclonal antibody directed at amyloid beta that has the potential to be a disease-modifying drug. They conclude with a discussion about how to define “healthy aging” and reflect on how understanding dementia can shape one’s life philosophy.
Subscribe on: APPLE PODCASTS | RSS | GOOGLE | OVERCAST | STITCHER
We discuss:
- How Amanda developed a passion for geriatric psychiatry [3:15];
- Defining and diagnosing dementia and Alzheimer’s disease [13:30];
- Medical tests for dementia and their relationship to clinical symptoms [22:45];
- The pathology of dementia, and the role of the tau and beta-amyloid protein in Alzheimer’s disease [33:15];
- The significance of ApoE genotype, and differentiating Alzheimer’s disease from Lewy body dementia [43:15];
- The evolution of Alzheimer’s disease prevention, care, and medications over the last 20 years [52:45];
- Psychiatric support for dementia patients (and caregivers) with depression and anxiety [1:02:45];
- Drug pipeline, clinical trials, and major challenges to overcome [1:13:45];
- Redefining Alzheimer’s disease and designing effective trials [1:23:00];
- The promise of monoclonal antibody treatments for Alzheimer’s disease [1:34:15];
- How we should measure outcomes in dementia trials and define “healthy aging” [1:42:30];
- How understanding dementia can reshape our life philosophy [1:53:45]; and
- More.
Get Peter’s expertise in your inbox 100% free.
Sign up to receive An Introductory Guide to Longevity by Peter Attia, weekly longevity-focused articles, and new podcast announcements.How Amanda developed a passion for geriatric psychiatry [3:15]
- Peter and Amanda met at a Zoom event for Hilarity for Charity, a non-profit organization focused on Alzheimer’s disease
- They appeared with Richard Isaacson to discuss Alzheimer’s disease research and treatment
- Peter was impressed by Amanda’s focus on the impact that Alzheimer’s disease has on the family as much as it does on the patient
- Amanda specializes in geriatric psychiatry
- She grew up in Philadelphia with active grandparents who owned and operated a nursing home
- “Seeing the vibrant lives they led even into their 70s and 80s, that to me was normal aging”
- But in medical school, she “really saw the pathologic side of aging and the things that can go wrong as we get older”
- She noticed an attitude of ageism among physicians
- One day she was sent in to talk to a woman who had come in from a nursing home with chest pain
- The doctors wondered how she had obtained a history because they said the woman did not make sense, but it turned out that the EMT had forgotten to bring the woman’s dentures, but she was mentally sound
- The doctors would have known this if they had taken the time to listen to her
“I realized how quick people are to brush off the elderly. And it kind of lit a fire in me so to speak so that that became my passion.” —Amanda Smith
- There are many ways to interact with elderly patients, like cardiology and other subspecialties
- When Amanda was starting out, there was not much that we could do about the cognitive side of things
- She graduated med school in 1997, the year that donepezil (Aricept) was first approved
- has witnessed the evolution of Alzheimer’s treatments
- The behavior problems that can occur in people with dementia (e.g., anxiety, depression, psychosis) have always been treatable
- These are common reasons to see people on the geriatric psychiatry unit (e.g., taking apart the ceiling tiles and their apartment to find these wires that weren’t really there)
- we can control some of these behaviors so that patients can have a better quality of life and caregivers can have a little more peace of mind
- Peter wonders if the patients typically already have a dementia diagnosis or if the presenting feature of the dementia can be some of these psychotic symptoms so the doctors need to rule out schizophrenia or other forms of psychosis
- Amanda says it’s both
- When psychosis presents first, patients sometimes get diagnosed with schizophrenia or bipolar illness or another illness that does not have an onset in the mid-70s
- Have a misdiagnosis for a few years until it becomes really apparent that there is an underlying neurodegenerative process
- Peter observes that the early stages of dementia can be quite unnerving and some of the behavior might be driven by legitimate and understandable fear that something is wrong
- Amanda says that some people are blissfully unaware throughout the entire course of their illness even in the very mild stages
- while others are acutely aware that something’s not right and know for two or three years before doctors can find any discernible changes on their testing
- The second group suffers much more
- Lewy body dementia
- a type of dementia that has characteristics of Alzheimer’s, characteristics of Parkinson’s, and very prominent visual hallucinations
- A few of Amanda’s patients are aware that their visual hallucinations are not real
Defining and diagnosing dementia and Alzheimer’s disease [13:30]
- Dementia is an umbrella term that denotes changes in memory and other areas of cognition
- represents a change from previous state (e.g., not born with it)
- interferes with your day-to-day function
- There are many causes of dementia, but Alzheimer’s is the most common
- Diagnosis
- have been advancements in many of our tests
- more sophisticated imaging techniques
- blood biomarkers
- But the real crux of diagnosis is a good clinical interview with the patient and with an observer
- Interview a family member or friend separately to get info about changes over time
- Specific tests
- cognitive testing to look for patterns that support one diagnosis over another
- brain imaging to look for things like strokes or shrinking in certain parts of the brain
- lab tests to rule out reversible causes of memory loss: thyroid disturbance, vitamin deficiencies, tertiary syphilis (very uncommon these days), etc.
- with this info can typically figure out the right label for them
- Sometimes we need formal neuropsych testing with a neuropsychologist
- Sometimes we do need PET scanning to look at certain patterns
- have been advancements in many of our tests
- Frontotemporal dementia
- relatively preserved memory, but significant changes in language or behavior
- It’s often the diagnosis when a relative says the patient’s memory is not too bad, BUT … they can’t really talk anymore, or they’ll get up in church and take the microphone from the pastor
- sometimes are erroneously diagnosed with bipolar illness because of these sudden and really profound behavior changes
- Problems with judgment: get labeled as being manic because of judgement issues like they’re spending lots of money, etc.
- Clinical story is very important for Alzheimer’s disease
- Very unlike cancer, where the diagnosis is typically based on imaging and the gold standard is a histological diagnosis – you don’t biopsy the brain
- A few formal tests are useful to confirm a diagnosis
- Lumbar puncture (LP) (“spinal tap”): sampling cerebrospinal fluid (CSF) to look for amyloid-β or tau protein
- PET to look for amyloid
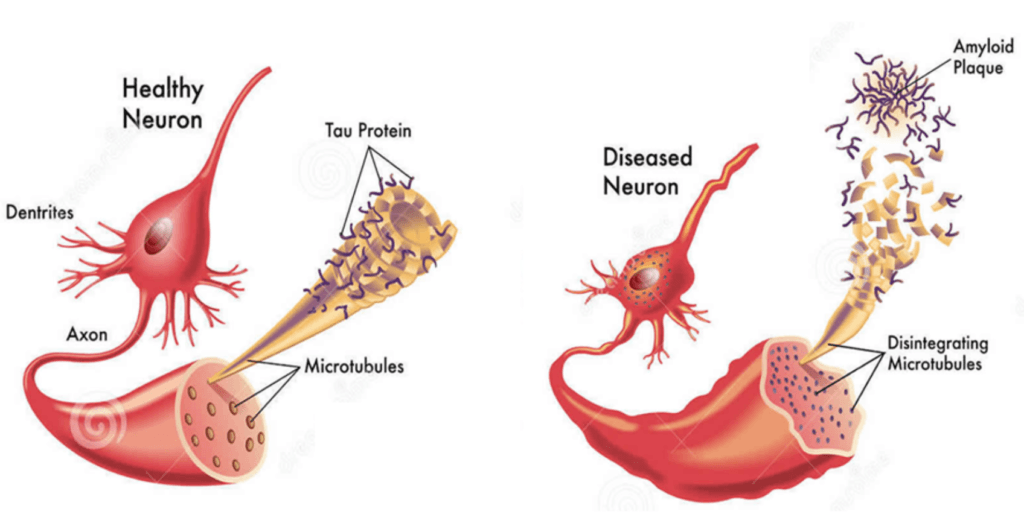
Figure 1. Amyloid-β plaques and tau protein (neurofibrillary) tangles are the microscopic signs of Alzheimer’s disease. Amyloid-β clumps together in plaques between neurons. Tau is a protein that normally stabilizes microtubules, structures that help transport nutrients and molecules. In Alzheimer’s, tau detaches from the microtubules and forms tangles inside neurons. Both plaques and tangles disrupt normal cell function and communication between neurons. Image credit: Health Jade
{end of show notes preview}
Would you like access to extensive show notes and references for this podcast (and more)?
Check out this post to see an example of what the substantial show notes look like. Become a member today to get access.
Amanda Smith, M.D.
Dr. Amanda Grant Smith is the Director of Clinical Research at the USF Health Byrd Alzheimer’s Institute in Tampa, FL, and a professor at the University of South Florida Health Morsani College of Medicine. Dr. Smith is on the University of South Florida Institutional Review Board and is a diplomate of the American Board of Psychiatry and Neurology, with subspecialty certification in geriatric psychiatry. Her work focuses on the diagnosis and treatment of memory disorders, caregiver education and support, and clinical research in Alzheimer’s disease. She did her internship, residency in psychiatry, and fellowship in geriatric psychiatry at the University of South Florida College of Medicine. She received her undergraduate degree from Emory University and her medical degree from Jefferson Medical College.
Academic website: https://health.usf.edu/medicine/psychiatry/faculty/asmith2
Twitter: @AlzDoctor



