Nearly three weeks into 2026, many are still riding the wave of motivation that comes with setting a New Year’s resolution to exercise more. But as the weeks go on, a number of those who have been showing up to the gym more frequently will start to fall out of the habit—often when the reality of the time commitment begins to feel unsustainable.
It’s not surprising, then, that people want to optimize time, especially when it comes to exercise. We all want to know: how can we get the most benefit for the least amount of time?
According to a recent paper, the answer is almost irresistibly simple: opt for intensity over duration. Using wearable data from more than 73,000 adults, the authors investigated the role of intensity in driving health benefits of exercise, and the results have grabbed headlines and social media attention over the last few weeks. The most eye-catching finding? For some health outcomes (i.e., cancer mortality reduction), the investigators report that each minute of vigorous activity corresponded to 156 minutes—over two and a half hours—at light intensity.
Throughout our content, we’ve advocated for a training program that includes sessions covering a range of intensities, with at least as much time devoted to moderate-intensity, steady-state exercise (zone 2) as to vigorous-intensity training (zone 5). But why spend hours doing light or moderate intensity exercise when you could simply knock out a few minutes of full-press effort and call it a day? Have we been wrong all this time?
It’s a tempting notion, but no. This interpretation oversimplifies the true results of the study, and more importantly, it fails to reflect how exercise works in the real world.
What they did
For this study, researchers Biswas et al. analyzed activity data from 73,485 adults from the UK Biobank (mean baseline age 61.6±7.9 years) and tracked various health outcomes among these individuals for a mean follow-up period of eight years. Rather than relying on self-reported activity (which is notoriously imprecise), activity was tracked using wrist-worn wearable devices, which participants wore continuously for up to seven days. Movement intensity was then classified in 10-second windows using device-based, machine-learning algorithms.
Intensity was defined using established acceleration thresholds—measured in milligravities (mg)—and mapped to approximate metabolic equivalents (METs), a unit that reflects the energy cost of an activity relative to resting metabolism (with 1 MET corresponding to resting energy expenditure). Movements producing less than 100 mg of acceleration were classified as light intensity, generally corresponding to activities under 3 METs, such as standing and other utilitarian movements (for example, washing dishes or ironing), as well as slow walking. Activities that generated higher acceleration signals were classified as moderate intensity when they reached or exceeded 100 mg, aligning roughly with activities in the 3 to 6 MET range (e.g., brisk walking). Higher-energy movements that exceeded 400 mg were classified as vigorous intensity, typically corresponding to activities of 6 METs or greater (e.g., jogging or running).
Time spent in each intensity category was then related to outcomes including all-cause mortality, cardiovascular events, type 2 diabetes, cancer incidence, and cancer mortality. The contribution of each intensity was isolated by statistically correcting for the time spent in the other intensity categories (a technique called “mutual adjustment”—we’ll return to this).
To estimate “equivalencies,” the authors compared how much light or moderate activity corresponded to the same modeled risk reduction as one minute of vigorous activity. For example, if one minute of vigorous activity corresponded to a given decrease in all-cause mortality risk, how many minutes of light or moderate movement would correspond to the same risk reduction?
Our research team spends hundreds of hours each month vetting studies and distilling dense literature to deliver evidence-informed insights on health and longevity. If you find value in our work, consider becoming a premium member and supporting our mission.









What they found
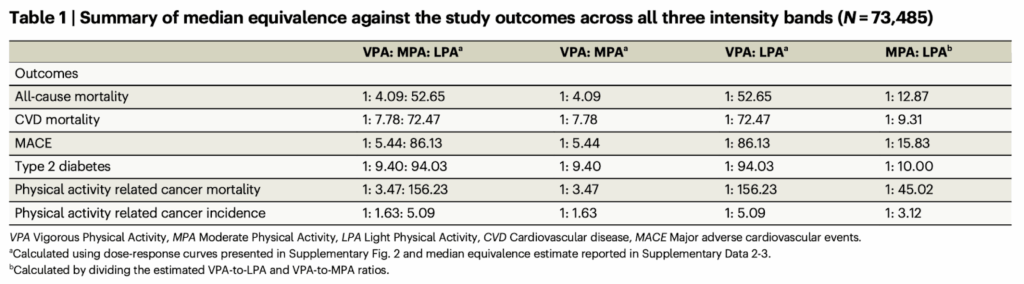
For all-cause mortality and cardiometabolic outcomes, one minute of vigorous movement corresponded to roughly 4–9 minutes of moderate activity and about 50–95 minutes of light activity. The contrast was even larger for cancer mortality, where we find the widely shared ratio of one minute of vigorous activity corresponding to similar risk reductions as 156 minutes of light movement. As shown in Table 1 from the original article (below), across outcomes, moderate activity consistently showed stronger associations per unit time than light activity, but vigorous activity appeared the most time-efficient.
Case closed—right? If that were the whole story, the implication would be simple: focus on increasing vigorous activity and you’ve covered your bases (and successfully minimized the amount of time you need to spend at the gym).
Unfortunately, that interpretation runs well ahead of what these data can actually support.
Where the interpretation breaks down
High-intensity work may indeed be more efficient in the sense that you get greater adaptations on a per-minute basis compared to low- or moderate-intensity work, so the general directions of the relationships reported by Biswas et al. agree with what was previously known. But unfortunately, that’s the most that we can conclude from these data. The limitations of this study exist on many layers, and as we peel them back, we find constraints all the way to the core.
First, the exposure here was brief and observational. Movement was measured over just three to seven days at some point in the study and then used to model outcomes years later. Over that span, training habits, fitness, injuries, and capacity can change substantially. What was captured was a short snapshot of behavior, which was then projected forward without any control over total volume of activity or how activity patterns evolve over time. That alone limits how precisely these results can inform individual decisions—but the constraints don’t stop there.
Let’s now return to the mutually adjusted regression models that we mentioned earlier, which sit at the center of the analysis. This approach is meant to account for the fact that people move at multiple intensity levels throughout the day and don’t perform light, moderate, and vigorous activity in isolation. Those behaviors tend to cluster together, and the model’s job is to untangle that overlap. It does this by asking how time spent at one intensity is associated with health outcomes after accounting for the time spent at the other intensities—similar to how other observational studies adjust for age, sex, or smoking when estimating disease risk. What the model is not doing is simulating a real-world replacement, when someone deliberately replaces one type of activity with another.
So while it’s fair to conclude from this model that one minute of vigorous activity is associated with a similar adjusted reduction in all-cause mortality risk as roughly 50 minutes of light activity, it’s not fair to conclude that one can automatically replace the other.
The reliability of this statistical framing becomes even shakier when we peel back the next layer and consider what’s actually being measured. The data come from wrist-worn accelerometers. This is likely an improvement over self-reported activity, but accelerometers measure movement, not physiological load. In other words, they capture how much and how fast someone moves, not how demanding that movement is for the person performing it. Consider two walks that could plausibly produce similar acceleration patterns at the wrist: a cool spring walk through rolling hills, and that same walk on a hot summer day while carrying a 50-pound pack. Or, imagine an untrained individual and a marathon runner doing the same hike. From the device’s perspective, these may look similar. From the body’s perspective, they are not.
As a result, the intensity categories used in this study—light, moderate, and vigorous—are device-defined, not physiology-defined. The same category may represent steady aerobic work in a trained individual and near-maximal effort in someone deconditioned or under load. When equivalence ratios are built on top of those categories, the apparent precision reflects the structure of the model more than the fidelity of the underlying signal. To think of it another way, the high degree of uncertainty in defining the movement categories means that any attempts to isolate one type of movement by statistically “correcting” for time spent engaging in the others will involve an enormous margin of error, such that the reported ratios provide virtually zero quantitatively reliable information about movement intensity and disease.
We could continue to peel layers back, but to keep our discussion from running off the rails, we’ll leave it at this: these data describe population-level associations between movement intensity (not exercise intensity) and long-term health outcomes. They do not resolve how intensity should be allocated within an individual training plan. Treating these results as time-conversion formulas substitutes statistical neatness for physiological reality—where durability, progression, and total volume still do most of the work.
So what do we do?
It’s worth returning to the level at which this paper is operating. The authors are asking a population-level question: what patterns of movement are associated with better outcomes across tens of thousands of people? That’s a fair question—but it’s not the same as asking what will produce the best result for a given individual.
Individual outcomes depend on individual context. Time availability, training history, injury risk, and current capacity all shape what is sustainable and effective. For most people, the answer is not choosing one intensity over another, but combining intensities with a clear purpose.
Steady-state work, for example, allows us to accumulate meaningful volume while keeping joint stress and fatigue in check. That volume builds the foundation that makes higher-intensity work safe and tolerable in the first place. Over time, it also allows us to extend the duration and frequency of harder efforts, rather than simply touching high intensity briefly and hoping it’s enough to see improvements.
The goal of high-intensity work isn’t to check a box or hit a zone for a minute or two. It’s to develop the capacity to handle more of that work, more often, with less fatigue and lower injury risk. That only happens when intensity is layered on top of a base that can support it.
We’ve covered this topic across multiple pieces of prior content. So much so that it would take hours to wade through it all—which, incidentally, is why we just released an AMA to cover the most valuable points in one episode. We walk through how to think about cardiorespiratory fitness, how different intensities fit into a coherent training strategy, how to progress them over time, and what common misconceptions to avoid.
The bottom line
Most of us don’t have unlimited time for exercise, so it’s understandable to seek efficiency. We all want to maximize the health and fitness returns for a given amount of exercise. So when we hear claims that a single minute of vigorous movement provides the same benefits as over two hours of light movement, it’s tempting to react by cutting down total physical activity—swapping hours at light or moderate intensity per week for a few minutes at vigorous intensity. But those claims are built on a very shaky study, and even if we ignore the questions of data reliability, the work by Biswas et al. tells us nothing about replacing one type of movement with another.
All intensities of movement matter, but they are not interchangeable. Vigorous work is necessary to push cardiorespiratory capacity, but it only delivers its benefits when layered on top of enough lower-intensity volume to make that stress tolerable and repeatable. Moderate, steady-state work provides that foundation, while light movement contributes to total activity without substituting for training. The right balance depends on the individual—their history, their constraints, and their goals—not on time-conversion ratios derived from high-uncertainty population data.
For a list of all previous weekly emails, click here.
References
- Biswas RK, Ahmadi MN, Bauman A, Milton K, Koemel NA, Stamatakis E. Wearable device-based health equivalence of different physical activity intensities against mortality, cardiometabolic disease, and cancer. Nat Commun. 2025;16(1):8315. doi:10.1038/s41467-025-63475-2