This video clip is from episode #210 – Lp(a) and its impact on heart disease with Benoît Arsenault, Ph.D., originally released on June 13, 2022.
Show Notes
There are 2 independent types of analyses that make it very clear that Lp(a) is playing a causal role in the development of atherosclerotic cardiovascular disease, independent of LDL
- 1 – The regular observational epidemiology, now that assays more accurately measure Lp(a)
- 2 – Mendelian randomization studies that are effectively nature’s randomized experiments
- 3 – Benoît adds a 3rd assumption, that the effect of LPA variants on cardiovascular disease are explained by higher Lp(a) levels
Clinical tests to measure Lp(a) [22:00]
Over the past decade, Peter has seen 3 different types of commercial assays for measuring Lp(a)
- 1 – Lp(a) cholesterol content; measured cholesterol of LDLs that had apolipoprotein(a) on them
- Some labs may still use this one
- The cholesterol within certain lipoprotein does not necessarily tell you a lot of information about the number of particles that are in the bloodstream, which is the most important thing to measure if you want to estimate risk
- The same is true for LDL
- For LDL and ApoB, there is some discordance in the amount of cholesterol
- But for LDL and Lp(a), the discordance is even higher
- 2 – Most labs report mg/dL of Lp(a); they are simply telling you the mass of Lp(a)
- Measuring the mass of the Lp(a) particle is much better than measuring the cholesterol in Lp(a) particles
- 3 – What you really want to do is try to find a lab that will give you an Lp(a) measurement in nanomoles per liter
- Don’t let good be the enemy of perfect here; if you have an Lp(a) measurement in mg/dL and it puts you in a high-risk range (an Lp(a) level above 50), then the chances of the Lp(a) assay that will give you a result in nmol/L will also give you a high level
- Keep in mind that if you have an Lp(a) of 50 mg/dL, the measurement in nmol/L will be around 125 nmol/L
- Lp(a) remains remarkably stable over time, so most guidelines tell you to measure it once in a lifetime
- The figure below shows the levels of Lp(a) associated with increased risk of CVD (in yellow and red)
- Most people are in the normal, low risk range (shown in green)
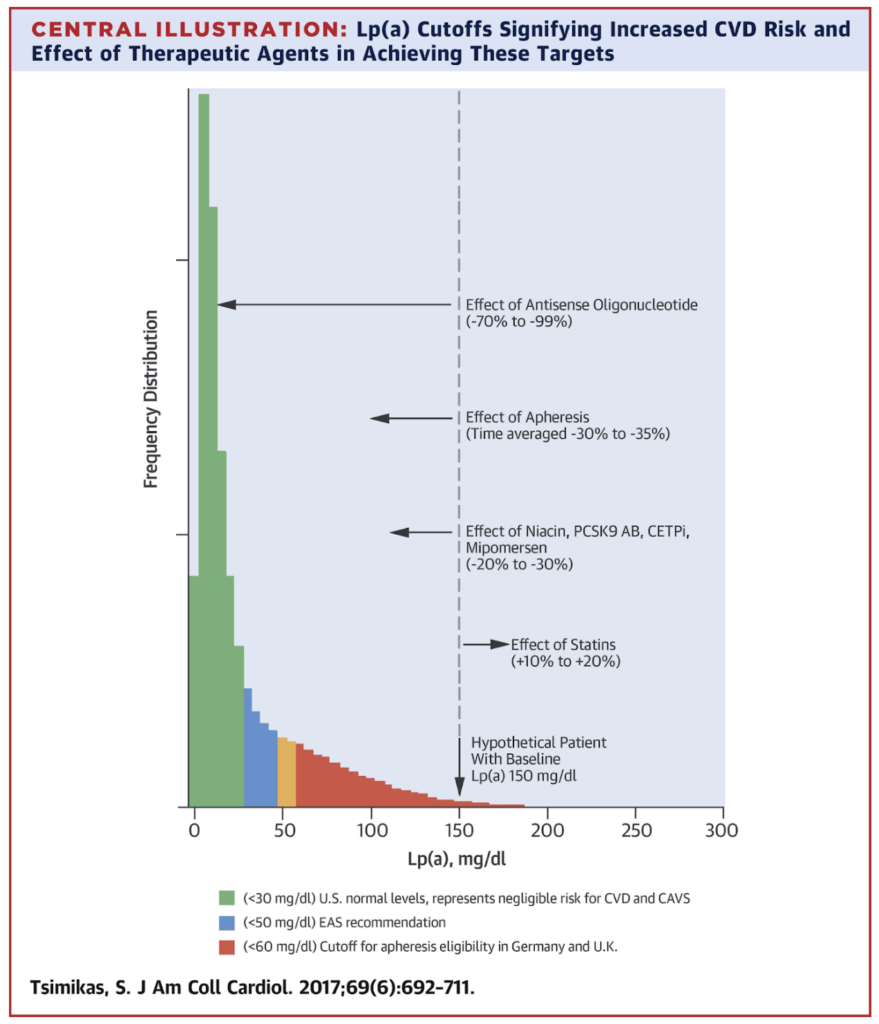
Figure 3. Lp(a) levels above 50-60 mg/dl are associated with increased risk of CVD. Image credit: Journal of the American College of Cardiology 2017
Peter’s takeaway: Lp(a) is something we measure to determine risk, after which point we don’t need to measure it; now you need to take measures elsewhere
Benoît Arsenault, Ph.D.
Benoît Arsenault obtained his doctoral degree in Physiology-Endocrinology from Université Laval in Québec City, Canada in 2009. He did postdoctoral research at the Academic Medical Center in Amsterdam and at the Montreal Heart Institute. Benoît is currently an Assistant Professor in the Department of Medicine at the Université Laval and a research scientist in the cardiology axis at the Centre de recherche de l’Institut universitaire de cardiologie et de pneumologie de Québec, in Canada.
The research of Benoît’s team is focused on understanding the risk of cardiovascular diseases such as atherosclerosis and aortic stenosis in relation to lifestyle and inherited risk factors. This includes extensive research in unraveling the role of Lp(a), HDL metabolism, PCSK9, and lipid-lowering therapies. [iucqp.qc.ca]