
A few months ago, I wrote about a study that showed metformin diminished improvements in skeletal muscle mitochondrial respiration, cardiorespiratory fitness, and whole-body insulin sensitivity after a 12-week aerobic exercise training (AET) program compared to a placebo in participants at risk for type 2 diabetes in their early 60s. I have also spent the last year doing endless self-experiments with and without metformin, examining the relationship between mitochondrial performance and metformin, using lactate testing at zone 2 (more on this topic another day).
Today, I want to cover a more recent study, that looked at the effects of metformin on the response to progressive resistance training (PRT) in relatively healthy seniors. A question you may be asking yourself is: why would you give relatively healthy people a drug for diabetes in the first place?
The two endpoints you should consider anytime you’re making a decision about a treatment or intervention are mortality and morbidity. Will this treatment help me live longer? Will this treatment relieve my symptoms or free me from future disability?
In that context, here’s what the investigators had in mind:
- As age progresses, the amount of skeletal muscle is highly correlated with disability and mortality, and resistance training (RT) is the most effective way to combat the loss of muscle mass and has been shown to increase strength.
- However, older adults may be non-responsive or less responsive to RT because of chronic low-grade inflammation and muscle-specific inflammation.
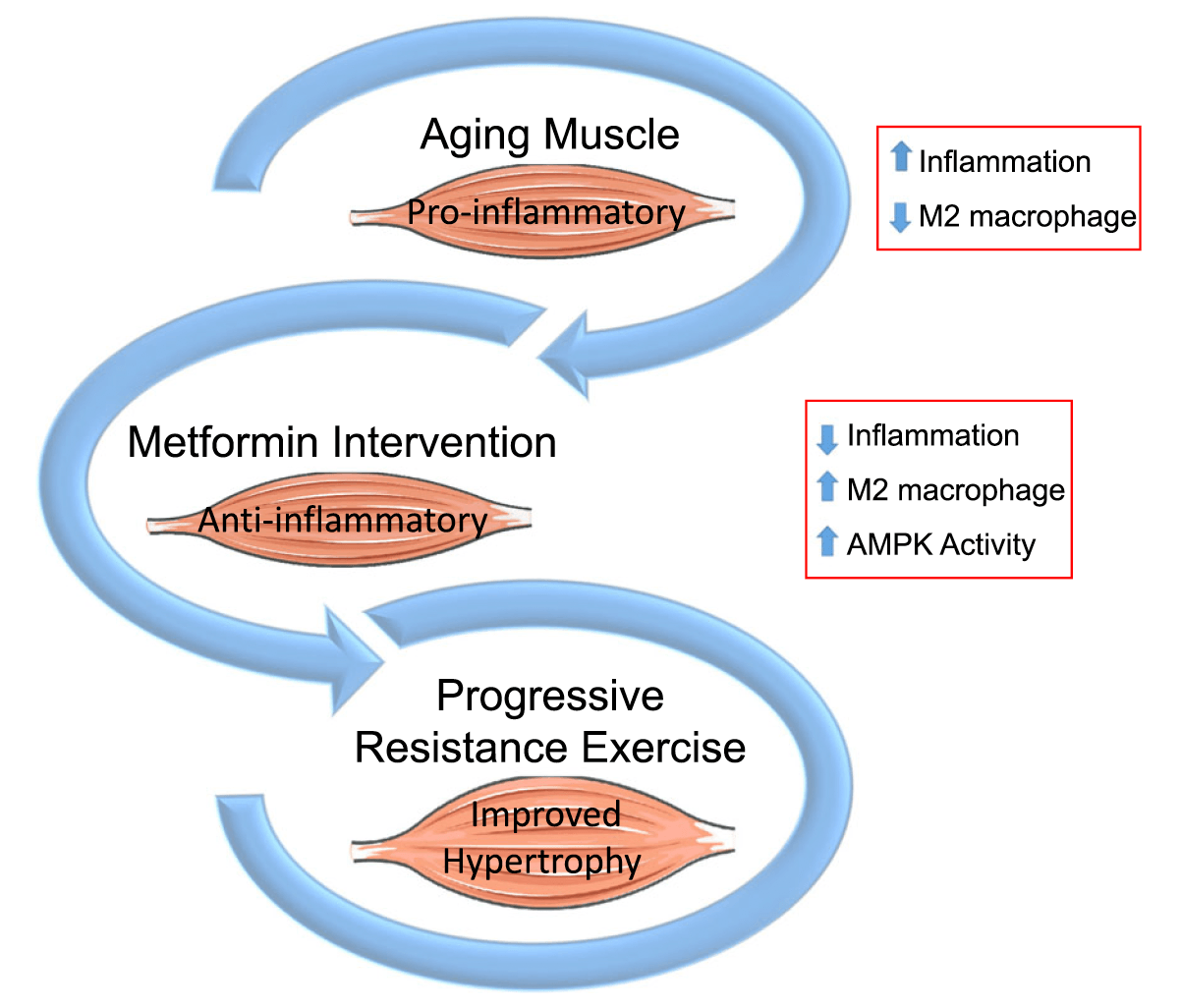
- Metformin has been shown to reduce inflammation in muscle, and the investigators believe this may be due to a shift in muscle macrophages from an inflammatory M1 state to an anti-inflammatory M2 state.
- In their preliminary analysis of muscles in insulin-resistant patients, metformin increased M2 macrophage abundance and decreased inflammatory cytokine gene expression.
- M2 macrophages facilitate muscle growth and repair by stimulating the activity of satellite cells.
Putting it all together, the investigators hypothesized that metformin would increase the abundance of M2 macrophages, reducing muscle inflammation,1The investigators wrote in their protocol paper: “The resolution of inflammation following injury in muscle is a product of both repressed inflammatory cytokine production and transcriptional up-regulation of anti-inflammatory genes like insulin-like growth factor (IGF)-1 and IL-4 and IL-10 from M2 macrophages.” and improving skeletal muscle hypertrophy with PRT.
Here’s a graphical figure from their study protocol paper:
 In order to test this hypothesis, the investigators put 94 relatively healthy men and women aged 65 and older (median age: 69.3) on a supervised 14-week PRT program (3d/wk of high, low, and high intensity resistance training on Monday, Wednesday, and Friday, respectively), and gave them either 1,700 mg (titrated up during a 2-wk wash-in period) metformin (n = 46), or placebo (n = 48) in a double-blinded fashion. To determine changes in muscle growth (i.e., hypertrophy), increases in satellite cells, and M2 macrophage abundance, they employed the use of thigh (vastus lateralis) muscle biopsies. The investigators also used dual‐energy X‐ray absorptiometry (DEXA) scans, mid‐thigh CT scans, and oral glucose tolerance tests to assess the effects of the intervention.
In order to test this hypothesis, the investigators put 94 relatively healthy men and women aged 65 and older (median age: 69.3) on a supervised 14-week PRT program (3d/wk of high, low, and high intensity resistance training on Monday, Wednesday, and Friday, respectively), and gave them either 1,700 mg (titrated up during a 2-wk wash-in period) metformin (n = 46), or placebo (n = 48) in a double-blinded fashion. To determine changes in muscle growth (i.e., hypertrophy), increases in satellite cells, and M2 macrophage abundance, they employed the use of thigh (vastus lateralis) muscle biopsies. The investigators also used dual‐energy X‐ray absorptiometry (DEXA) scans, mid‐thigh CT scans, and oral glucose tolerance tests to assess the effects of the intervention.
The good news was that 14 weeks of PRT resulted in significant gains in total lean mass (determined by DEXA) and thigh muscle mass overall. The not-so-good news was that metformin blunted these gains. In other words, so much for the hypothesis that metformin would enhance skeletal muscle hypertrophy in response to PRT. Metformin also did not affect increases in satellite cells or increases in M2 macrophages.
Here’s the graphical abstract of the current paper:
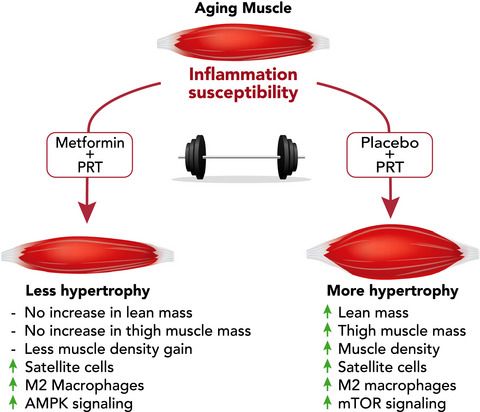
Note that statistically significant differences between the groups were found for gains in lean mass (placebo gained 1.95% versus 0.41% for metformin; p = 0.003), thigh muscle mass (placebo gained 3.90% versus 0.45% for metformin; p < 0.001), and average muscle density (placebo increased by 4.13% versus 2.49% for metformin; p = 0.020). While satellite cells and M2 macrophages increased in the metformin group, these were not significantly (statistically speaking) different compared to increases in the placebo group. Metformin had a higher change in basal AMPK (not statistically significant) and ACC (p = 0.035) phosphorylation, and a blunting of RPS6 activation, a downstream target of mTORC1 (not statistically significant) compared to placebo.
The results actually shouldn’t be surprising, given that emerging data indicate metformin blunts some of the beneficial effects of AET, RT, and combined exercise training, according to the investigators (and reviewed in this paper).
Why is metformin not playing nicely with exercise? I don’t think we have a concrete answer, but I think, as I elaborated on in a previous email on the subject, the anti-inflammatory and antioxidant effects of metformin are disrupting the body’s adaptive response to the pro-inflammatory and reactive oxygen species (ROS)-promoting effects and the biological signals they elicit.
Acute inflammation is a physiological response that promotes the healing and repair of tissues. As many as 600 “myokines”—cytokines synthesized and released by myocytes during muscular contractions—have been identified, for example, and some of these can have long-term anti-inflammatory effects. Chronic inflammation can result in the opposite. Similarly, acute oxidative stress can lead to beneficial adaptive responses, while excessive concentrations of ROS can have deleterious effects. (The individual credited with the formulation of the concept of oxidative stress, Helmut Sies, refers to the terms oxidative eustress and oxidative distress, in this context.) It’s also possible that metformin is attenuating muscle hypertrophy because of inhibition of mTORC1.
While there was a statistically significant difference in skeletal muscle hypertrophy between the two groups, when the investigators tested the strength of the two groups, the differences were not statistically significant. Three strength parameters were measured, including a one-rep maximum (1RM) in knee extension, knee extension isometric strength, and peak knee extension power. While strength increases were higher in the placebo group for all three, none of them reached statistical significance. In addition, when the investigators looked at the 1RMs of participants relative to their thigh mass via DEXA, the gains were similar in both groups (placebo improved 19.7% versus 14.5% for metformin; p = 0.188).
I don’t think this study is a nail in the coffin for the arguments against taking metformin if you’re relatively healthy and exercise regularly. In this study, men and women in their mid-60s and older increased muscle mass and strength following 14 weeks of PRT, as expected, regardless of whether they were on metformin or not. Yes, metformin appeared to inhibit these gains, but one of the potential reasons why may be due to an inhibition mTORC1, which may have benefits independent of these findings. Metformin not only may have decreased mTORC1 in the skeletal muscle, but it may have inhibited in other tissues, like the liver, where it may have more positive effects. In other words, it’s possible that the metformin group may have benefitted from an increased activation of AMPK, enhanced autophagy, and global inhibition of mTORC1, but it won’t be captured in the study.
Also, this was a relatively short-term (14-weeks) study that introduced two variables at the same time (PRT and metformin). Two quite potent interventions with remarkable physiological effects on their own. Both of these variables may be beneficial to continue long-term for extension of healthspan. (I think it’s hard to argue at this point that seniors won’t benefit from a healthspan perspective by engaging in regular resistance training over their lifetime.) For the individuals in the study (median age: 69), that would mean resistance training, and taking metformin (or placebo), for about a decade, on average. If this study was continued for another 10 years, would we see a regression toward the mean, with the training benefits (i.e., power, strength, hypertrophy/prevention of sarcopenia) looking very similar in the metformin and placebo group? Or would we see the opposite: the placebo group continues to progress and the attenuated effects in the metformin group accumulates over time and widens the training-benefits gap between the two groups? Or is it possible that the relative strength (i.e., improvement in strength / skeletal muscle hypertrophy) of the participants taking metformin increases beyond that of the placebo group? What if another arm in the long-term study engaged in PRT on Monday, Wednesday, and Friday, and took 1,700 mg of metformin 1x/d on Tuesday, Thursday, Saturday, and Sunday afternoons: would that make a difference? I don’t think the answers to any of these questions are clear at the moment.
I think we are further from resolving this question—Is metformin a drug healthy people should take to live longer?—than I would have guessed a year or two ago. So it goes with science. I stopped taking metformin this year (after doing so for 9 years) based on entirely different data and rationale. Perhaps I will resume at some point, pending more information.
Should you continue to take metformin as an anti-aging compound if you regularly engage in resistance training and aerobic exercise? I think that depends on a number of factors, including your metabolic status, your body composition, and your risk/reward tolerance. It likely comes down to who we are, what we are optimizing for, and looking for more ways we can improve our knowledge of the risks and benefits of these interventions, and their various interactions with each other. Sorry I don’t have a more prescriptive answer.
– Peter



