Tom Dayspring is a world-renowned lipidologist and one of the most thoughtful teachers in the field of lipid metabolism. In this episode, Tom returns to The Drive for a deep dive into the relationship between lipids and brain health, beginning with the fundamentals of cholesterol transport before exploring why the brain’s cholesterol system operates almost entirely independently from the rest of the body. Tom examines the roles of apoB, apoA-I, and especially apoE in cholesterol homeostasis, discusses how APOE genotype influences Alzheimer’s disease risk, and unpacks the complex links between cholesterol metabolism, amyloid, and tau pathology. He also reviews what is currently known—and still uncertain—about the effects of statins, ezetimibe, omega-3 fatty acids, and emerging CETP inhibitors on brain health and neurodegenerative disease risk. Although highly technical, this conversation provides an essential framework for understanding the nuanced relationship between lipid-lowering therapies, cardiovascular disease prevention, and neurodegenerative diseases in an area often clouded by misinformation.
Subscribe on: APPLE PODCASTS | SPOTIFY | RSS | OVERCAST
“My mission for The Peter Attia Drive has always been to provide you with the most rigorous, evidence-informed insights on longevity. To do that without cluttering your experience with ads, we rely entirely on our premium members. If you’d like to support the work that makes this mission possible, consider becoming a premium member.”
– Peter
We discuss:
- The fundamentals of cholesterol transport in the body, and how peripheral cholesterol metabolism differs from cholesterol handling in the brain [2:45];
- How cholesterol is transported through plasma and stored within cells, and why lowering LDL cholesterol does not deplete the body or brain of cholesterol [11:45];
- How apoB particles drive atherosclerosis, why lowering lipids matters, and the factors that influence individual cardiovascular risk [20:00];
- How the brain produces and transports its own cholesterol using apoE lipoproteins independently of circulating cholesterol and apoB-containing lipoproteins [29:00];
- How apoB structure influences LDL receptor binding and LDL clearance [39:00];
- How neurons acquire cholesterol from apoE-containing lipoproteins and why desmosterol serves as a unique marker of cholesterol synthesis in the brain [41:45];
- The difference between the APOE gene and the apoE protein, the major APOE genotypes found in humans, and how APOE4 influences Alzheimer’s disease risk [48:45];
- HDL function beyond cholesterol: immune function, protein cargo, and communication with the brain [53:30];
- How APOE4-associated defects in brain cholesterol transport may promote Alzheimer’s disease: amyloid production, neuronal cholesterol homeostasis, and cholesterol clearance [58:00];
- Statins and brain health: reviewing the evidence of the potential impact of statins on cognition and Alzheimer’s disease risk [1:09:00];
- Desmosterol and 24S-hydroxycholesterol as biomarkers of brain cholesterol metabolism and statin effects [1:17:15];
- Possible cognitive benefits of ezetimibe beyond lowering apoB [1:19:30];
- EPA, DHA, and the evidence for omega-3 fatty acids in brain health [1:23:15];
- Obicetrapib: an emerging CETP inhibitor with potential implications for both cardiovascular and brain health [1:31:00]; and
- More.
Show Notes
The fundamentals of cholesterol transport in the body, and how peripheral cholesterol metabolism differs from cholesterol handling in the brain [2:45]
- Today we’re going to focus on a topic that’s become an enormous passion of Tom’s
- And his curiosity drives so much of his learning, and by extension the learning in Peter’s practice
- We are going to go on a journey into this idea of cholesterol in the brain
- It’s a very important topic for reasons that we’ll get into
- It’s worth making sure that everybody is starting from the same knowledge base as it pertains to lipids
- Let’s start at the very beginning in a short 5-minute version
Talk through the idea of cells in the body making cholesterol and how they have to move that cholesterol around the body in the periphery
- Cholesterol is essential for human life because it’s used for making some critical things
- But its most important function is that it positions itself in the cell membranes in every cell in our body
- And cholesterol regulates the integrity of cell membranes: what gets in, what gets out of cell
- Evolution has given every cell in the body the power to de novo synthesize cholesterol a little bit
Now each cell needs a minor number of molecules of cholesterol or so, and if it does that, we’ve got great cell membranes and those cells are functioning happily
But we also know, like so many things, an excess of anything can be harmful
- If any cell somehow has oversynthesized cholesterol, accumulated cholesterol and has excess molecules, cholesterol has the ability to crystallize, which is toxic to a cell
- It will kill the cell
- So evolution has also given cells the ability to export cholesterol out of its cytosol into the plasma
- But as talked about many times, lipids are hydrophobic
- They cannot circulate in plasma, which is an aqueous or water solution
- So again, evolution said, “No problem”
- Evolution has given us proteins that can bind and adhere to lipids and enwrap them into particles–they are the lipoproteins
- And that’s how lipids, cholesterol, triglycerides, and numerous other lipids that we don’t have to mention circulate in our bloodstream
- So if a cell effluxes cholesterol out, it joins on a protein
- The protein happens to be called apoA-I, which is sort of the structural protein of our high density lipoproteins (HDL)–that’s how HDLs are created
HDLs accept cholesterol from whatever cell in the body is effluxing it
We have another family of lipoproteins (LDL) that are much bigger than the HDLs and those are produced in the liver
- One type is produced in the small intestine and they belong to the apoB family of lipoproteins
- And the difference between them and HDLs is their structural protein is this very large peptide called apolipoprotein B
- [the figure below shows the family of apoB containing lipoproteins (including LDL) and the apoA-I containing lipoproteins (HDL)]
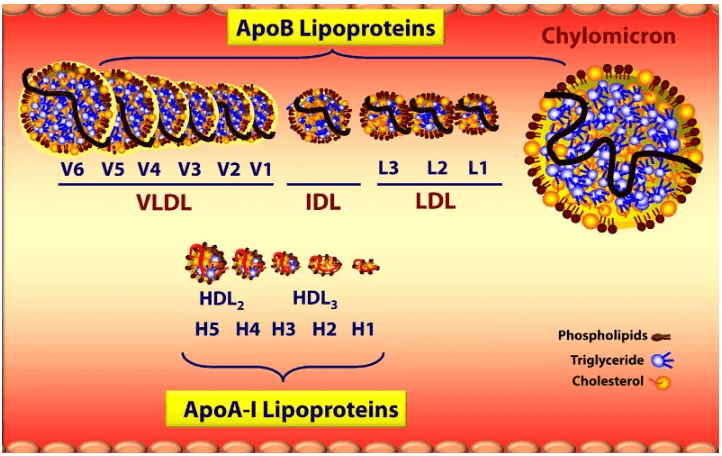
Figure 1. Two families of lipoproteins are defined by their surface protein: apoB or apoA-I. Image credit: Tom Dayspring
- The liver makes a full size apoB; the intestine makes a truncated one [these are 2 different isoforms]
- We call the hepatic apoB: apoB-100
- We call the intestinal produced apoB: apoB-48 (because it has 48% of the molecular weight of 100)
- So when the intestine makes a chylomicron, it’s in an apoB-48 particle, a very transient postprandial particle
- Chylomicrons traffic absorbed fatty acids–which become triglycerides, and absorbed cholesterol into the bloodstream [these are dietary fats and cholesterol]
- The liver manufactures apoB particles, and one is a very low-density lipoprotein (VLDL)
- It’s quite big because it’s packing the triglycerides, which like the chylomicrons, it transports to muscles and fat cells primarily, and then returns to the liver
- Some of the VLDLs as they lose the triglycerides, they shrink and they become something called either a VLDL remnant: a very transient particle called an intermediate-density lipoprotein (IDL), which rapidly becomes a low-density lipoprotein (LDL)
- The liver also has the ability to de novo manufacture and secrete LDLs also
So our LDLs that are floating around [in the blood] have 2 sources: they’re sort of like the son of a VLDL or they’re a liver produced one
Now, the apoB particles carry a lot of lipids
- Triglycerides [are carried] primarily in the VLDL
- The LDL is very interesting: it’s pretty much a cholesterol carrying particle
- It will carry X amount of triglycerides
- But it has the longest plasma residence time of anything in the apoB family
- It can last 3-4, even 5 days in some circumstances
Ultimately (just like the VLDL), LDL gets cleared by the liver via the LDL receptor
- The liver expressed LDL receptor sticks out into the plasma and binds to these apoB particles and pulls them into the liver
- And then the liver digests them and does whatever it wants with the component parts of the lipoprotein
The LDLs hang around for that amount of time, and this is not well recognized because they interact with the HDLs
- This is something that is NOT totally well known
⇒ If we look at all the lipoproteins in the body, 90% of them are HDLs, and the rest of the apoB family
- Now, the apoB family traffics far more lipids because of their size
- The volume of the sphere is a third power of the radius
- So a couple of nanometer increase in diameter–boy, a lot more lipids can be carried
After the HDL has sucked out all of the cholesterol from wherever it has, it becomes a big, fat mature HDL
- And now it has to do things with that cholesterol
- It has the option of
- Delivering it to steroidogenic tissue that makes cortisone or gonadal hormones
- It can bring it to the adipocytes (the cholesterol storage organ)
- Or it can return it to the liver, and even now the small intestine
But a lot of what an HDL does is it transfers its cholesterol mass into the apoB particles, the majority of which are LDLs because of its long plasma residence time
We’ve always been taught that HDLs do reverse cholesterol transport
- And they can: HDLs can bring cholesterol back to the liver or the gut
⇒ Tom explains reverse cholesterol transport at the beginning of episode #22
- Interestingly, if HDLs send their cholesterol to an LDL, the HDL becomes very small and it starts its journey all over again
- And then the LDL says, “Thank you, HDL. I’ll take your cholesterol and I’ll return it to the liver.”
So what we used to think was a very simple reverse cholesterol transport system becomes an indirect RCT, meaning LDLs bring it back to the liver, or direct where the HDL will bring it back
- Total RCT is the sum of both
“Most people are not aware that the primary function, why we have LDLs, is to return cholesterol to the liver.”‒ Tom Dayspring
- Everybody thinks the job of LDLs is delivering cholesterol to cells
- Almost never because every cell can make all the cholesterol it needs
⇒ In an emergency, any cell can upregulate an LDL receptor and pull in the LDL if it needs cholesterol, but just doesn’t happen for the most part
- Why? One reason we’re going to talk about it because it’s pertinent to the brain
- If LDLs are bringing cholesterol back to the liver, and if we can induce that with some of the drugs that we have that make LDL receptors expressed and stay expressed longer–we will drop LDL cholesterol levels in the plasma extremely low
- And as we get deeper into the brain, unfortunately, a prevalent belief out there in the real world is, “I don’t ever want to lower LDL cholesterol too much, because I’ll deprive the brain and I’ll injure the brain,” and soon we’ll talk about why that is NOT true
This is the peripheral way that our body handles cholesterol
- By peripheral we mean anything that is NOT in the brain
Tom emphasizes, “The brain lipid and lipoprotein system that we’re going to talk about has almost nothing to do with the plasma transportation of lipids and lipoproteins.”
How cholesterol is transported through plasma and stored within cells, and why lowering LDL cholesterol does not deplete the body or brain of cholesterol [11:45]
Peter’s synthesis of some of Tom’s points
{end of show notes preview}
Would you like access to extensive show notes and references for this podcast (and more)?
Check out this post to see an example of what the substantial show notes look like. Become a member today to get access.
Tom Dayspring, M.D.
Thomas Dayspring MD is certified in internal medicine and clinical lipidology. He is a Fellow of the American College of Physicians and a Master of the National Lipid Association (MNLA, the highest honor bestowed by the National Lipid Association). In 2012 after practicing in New Jersey for 37 years, he moved to Virginia and served as an educational director for a nonprofit cardiovascular foundation and until mid-2019 as a Chief Academic Advisor for two major CV laboratories. Since then, he has been a Lipid Specialist at Early Medical. Career-wise he has given over 4000 domestic (in all 50 states) and several international lectures, including over 600 CME programs on atherothrombosis, lipids/lipoproteins (and their treatment), vascular biology, biomarker testing, and women’s cardiovascular issues. He was the first physician in the US certified in both Clinical Lipidology and as a Menopausal Practitioner by the Menopause Society. He has authored several manuscripts and lipid textbook chapters and performed numerous podcasts. For several years he was an Associate Editor of the Journal of Clinical Lipidology. He was the recipient of the 2011 National Lipid Association’s President’s Award for services to clinical lipidology and the 2023 Foundation of NLA Clinician/Educator Award. He is the leading global influencer on social media and has over 104K followers on his educational X feed (@Drlipid). He has Gold Heart Member status as a professional member of the American Heart Association and serves as a Social Media Ambassador for the European Atherosclerosis Society and for the National Lipid Association.