When you think of a heart attack, a classic scene might come to mind: an older man is chowing down on a bacon burger when all of the sudden, he clutches his chest. Cut to the hospital, where a cardiologist explains that a ruptured atherosclerotic plaque in his arteries blocked blood flow and caused a heart attack—more formally known as a myocardial infarction (MI). He’s booked for a triple bypass surgery to help restore blood flow to his heart and is put on lipid-lowering medication (and told to rethink the bacon burgers).
Indeed, the version of events described above is the most common pathway to an MI: atherosclerosis progresses to the point that it obstructs an artery and triggers a heart attack, an event defined by insufficient oxygen reaching the heart. But although atherosclerosis may be the most common root cause of MIs, it isn’t the only possible cause. A recent study explored the relative contribution of other causes, investigating how often they are misdiagnosed and how these mechanisms differ between men and women.1
Alternative causes of heart attacks
If we were to look at the arteries of the hypothetical man described above, we’d see a buildup of lipid-rich plaque. Plaques originate with apoB cholesterol-carrying particles (the majority of which are LDLs) that accumulate within the arterial wall. The vessel responds with an inflammatory remodeling process that generates plaques of varying composition and stability. Critically, when a plaque ruptures or erodes, it can trigger formation of a blood clot (a thrombus). It’s this clot that narrows or blocks the artery acutely, immediately reducing blood flow and thus oxygen supply to the heart (ischemia), or blocking it altogether (infarction)—much like pinching a hose to stem water flow. This combined process of plaque plus clot is known as atherothrombosis, and it drives most heart attacks.
But several other less common mechanisms that reduce oxygen supply to the heart can cause injury or produce an MI without plaque rupture. These include:
- Supply/demand mismatch (SSDM): a mismatch between the amount of oxygen that is supplied and the amount needed, often resulting from artery narrowing due to stable atherosclerotic plaque, but also potentially caused by anemia or fast, irregular heartbeats and hypotension.
- Spontaneous coronary artery dissection (SCAD): a tear within the coronary artery wall that restricts blood flow.
- Coronary embolism: a clot traveling through circulation and blocking a coronary artery, which can sometimes result from atherosclerotic plaques moving more distally in circulation.
- Vasospasm: a transient constriction of a coronary vessel that sharply limits blood flow.
- Myocardial infarction with non-obstructed coronary arteries-unknown (MINOCA-U): a term to describe heart attacks for which no clear cause is identified (i.e., a patient shows a diagnostic electrocardiogram signal but not significant coronary obstruction is detected).
In addition to these alternative causes for MI, a number of other mechanisms can result in other types of heart injury. While most of these mechanisms are beyond the scope of this discussion, two are relevant here because they can mimic many features of an MI, and thus are often treated as possible MIs upon presentation at a hospital:
- Myopericarditis: inflammation involving both the myocardium (heart muscle) and the pericardium (the sac surrounding the heart).
- Takotsubo syndrome: stress-induced weakening and ballooning of the heart muscle (the left ventricle).
Identifying these alternative mechanisms is not just a matter of semantics. These conditions vary in their implications for both immediate treatment and long-term management, and a misdiagnosis of the underlying cause of an apparent MI can therefore have life-threatening consequences. For instance, angioplasty—which involves insertion of a catheter with a balloon to reopen a blocked artery—is often employed as an emergency procedure to restore blood flow in the event of an MI, but this procedure could lead to catastrophic damage if performed on a patient who has experienced SCAD. Thus, investigators Raphael et al. sought to characterize the prevalence of these other causes of heart injury and determine how they might differ between the sexes.
Our research team spends hundreds of hours each month vetting studies and distilling dense literature to deliver evidence-informed insights on health and longevity. If you find value in our work, consider becoming a premium member and supporting our mission.









What they did
To identify patients with heart injury in a cause-agnostic manner, the researchers relied on troponin—a highly sensitive blood biomarker of myocardial injury. When heart muscle is injured by any mechanism, it releases certain proteins—cardiac-specific troponins—into the bloodstream. Circulating levels of troponin increase regardless of whether the cause is a classic atherothrombotic event or one of the alternative mechanisms listed above, so by selecting patients based on troponin data, Raphael et al. could cast a wide net for various cardiac injury causes.
They utilized the Rochester Epidemiology Project, a comprehensive medical-records linkage system that captures nearly all healthcare encounters within Olmsted County, Minnesota. The investigators focused on adults 65 and younger, a group more likely to experience non-atherothrombotic causes of MI. From this population, the team performed a detailed retrospective review spanning 15 years (January 2003 through March 2018), and only cases in which troponin levels reached the 99th percentile (≥0.01 ng/mL)—the clinical definition of myocardial injury—were included. Two expert cardiologists independently reviewed each case to determine the most likely underlying mechanism.
These troponin cutoffs yielded 4,116 total events across 2,790 individuals. Of those, 1,606 met criteria for one of the eight mechanisms described above (i.e., atherothrombosis plus the seven alternative causes listed earlier), while the remainder were classified as other forms of heart injury and were excluded from further analysis. The resultant sub-grouping was a far more accurate map of heart injury—one that exposed historical misdiagnoses and revealed sex differences that available studies had not yet captured.
What they found
After expert review, approximately 4% of cases (61 events) were reclassified from their original diagnoses of X to Y. Most of these reclassifications involved patients initially diagnosed with either an atherothrombotic MI or an MI of unknown cause (MINOCA-U) who were ultimately determined to have SCAD or coronary embolism. Although the proportion was modest, these revisions illustrate how misidentification of underlying mechanisms can and does occur and may lead to inappropriate treatment.
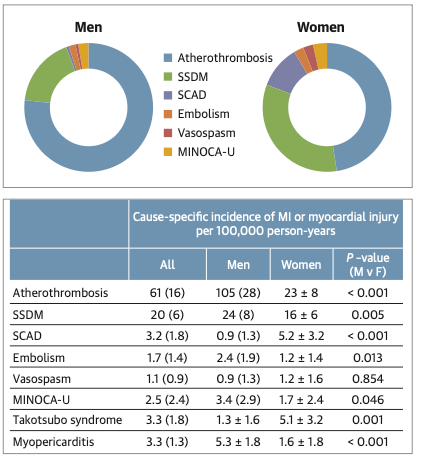
More strikingly, incidence patterns differed by sex, both in overall MI rates and in the distribution of underlying mechanisms (see Figure). Overall MI incidence was nearly three times higher in men under 65 compared to women under 65, with 137 events per 100,000 person-years among men compared with 48 among women. For men, the “classic” cause of a heart attack—atherothrombotic MI—accounted for the majority of cases, representing roughly three-quarters of all MIs and occurring at a rate of 105 per 100,000 person-years.
But remarkably, this pattern was reversed in women. Though atherothrombosis still caused more MIs than any other individual mechanism, it accounted for less than half (47%) of the total number of cases in this young cohort. The majority of MIs that occurred among women arose from non-atherothrombotic mechanisms, the most common being supply/demand mismatch (SSDM). (As noted earlier, atherosclerosis can itself be a cause of SSDM, but SSDM is not considered atherothrombotic because it does not involve plaque rupture and thrombus formation). However, differences between sexes were most dramatic when examining cases of coronary dissection (SCAD), for which incidence in women was more than fivefold higher than in men (5.2 vs 0.9 per 100,000 person-years). Indeed, SCAD accounted for approximately one in ten MIs in women under 65.
Although these results come from a relatively homogeneous Midwestern population—suggesting the exact prevalence of each mechanism may not be generalizable—the overall pattern is clear. Though heart attacks are traditionally linked to rupture of atherosclerotic plaques, younger women have a substantial likelihood of experiencing an MI driven by entirely different mechanisms. This trend is corroborated by earlier research, which has shown that, among adults under age 55, women account for approximately 90% of all coronary events not attributable to atherosclerotic plaque build-up or rupture.2
A lesson in preparedness
The implications of this study extend beyond hospital recordkeeping and even beyond decisions about post-MI treatments. They also teach us an important lesson about being prepared to recognize and respond to symptoms of a heart attack when they arise.
Knowing the role of apoB-containing lipoproteins in the progression of atherosclerosis, it may be tempting to believe that as long as our apoB levels are low, our blood pressure is normal, we’re metabolically healthy, and we don’t smoke, that we have no risk of an MI. If we experience chest pain or shortness of breath, we may brush it off as heartburn or passing anxiety, especially if we’re still in our middle-age years or younger.
Make no mistake—atherosclerosis remains the top cause of cardiovascular events by a wide margin, particularly if we expand our perspective to include those over the age of 65. Monitoring LDL cholesterol and apoB and initiating lipid-lowering medications when warranted are still among the most important steps you can take to protect yourself against heart attacks.
But as this study demonstrates, atherothrombosis is not the only cause of MIs. On the contrary, for women under age 65, the majority of MIs appear to be attributable to other, non-atherothrombic mechanisms. Some proportion of these are still caused by atherosclerosis, as the build-up of plaque can lead to a narrowing of the arteries and insufficient oxygen supply to the heart (i.e., SSDM), but many other mechanisms can occur even in the absence of other cardiovascular risk factors (though classic “heart healthy” measures like regular exercise, stress management, and avoidance of smoking can reduce risk). Even in a general population, these atherosclerosis-independent (i.e., excluding SSDM) mechanisms have been estimated to account for 5–10% of all MIs—a small but significant minority—and women are disproportionately at risk across all age groups.3,4 Thus, general health and the absence of obstructive atherosclerosis are not foolproof protection against life-threatening cardiac injury and certainly should not be taken as a reason to ignore heart attack symptoms, especially for younger women.
Indeed, in addition to significant differences in the causes of heart attacks between the sexes, men and women can also differ in the symptoms of a heart attack—and again, women are more likely than men to deviate from what might be regarded as “classic” signs. While men typically experience symptoms that align with the traditional description of myocardial ischemia—such as central chest pressure, squeezing or heaviness, and pain radiating to the arm, jaw, or shoulder, often triggered or worsened by exertion—women, by contrast, often report symptoms such as shortness of breath, nausea, vomiting, unusual fatigue, lightheadedness, palpitations, or discomfort in the back, neck, or upper abdomen (though they frequently present with the symptoms seen in men, as well). These differences in presentation do not appear to be explained by differences in the underlying mechanism of MI. Rather, they are observed across both atherothrombotic and non-atherothrombotic events.
That said, not all cases of cardiac injury or MI follow these symptom patterns, and both sexes can experience so-called “atypical” symptoms. The specific location of the blockage and oxygen deficit can alter the symptom profile. For instance, an MI affecting higher and more lateral areas might present with shoulder pain, whereas an MI affecting a lower part of the heart might present with abdominal pain or a sense of indigestion. When these types of symptoms occur suddenly and persist for more than a few minutes without any clear cause, they may signal a heart attack, and the policy across US emergency rooms is to triage them as such.
The bottom line
Myocardial infarction is not a single, uniform condition. While atherothrombosis accounts for the majority of MIs, non-atherothrombotic mechanisms are more common than you might expect among people under 65, and among women in particular. Correctly identifying which mechanism is responsible is not merely a technical distinction; it shapes the treatments that are appropriate and determines whether opportunities for timely, effective care are recognized or missed.
But even before an MI occurs, recognizing the possibility of non-atherothrombotic mechanisms of cardiac injury can help to ensure that we are prepared if and when we experience cardiac symptoms such as chest pain or pressure. A healthy lipid profile and clean bill of health should never be taken as a reason to ignore serious warning signs, especially for women. Even if the symptoms do indeed turn out to be a particularly bad case of heartburn, the cost of not seeking medical attention in the event of a serious cardiac event is simply too great.
For a list of all previous weekly emails, click here.
References
- Raphael CE, Sandoval Y, Beachey JD, et al. Causes of myocardial infarction in younger patients: Troponin-elevation in persons ≤65 years old in Olmsted County. J Am Coll Cardiol. 2025;86(12):877-888. doi:10.1016/j.jacc.2025.07.012
- Safdar B, Spatz ES, Dreyer RP, et al. Presentation, clinical profile, and prognosis of young patients with myocardial infarction with nonobstructive coronary arteries (MINOCA): Results from the VIRGO study. J Am Heart Assoc. 2018;7(13). doi:10.1161/JAHA.118.009174
- Dees D, Rahimi F, Amann M, et al. Prevalence and causes of myocardial infarction with non-obstructive coronary arteries in a contemporary cohort of patients with suspected myocardial infarction. J Clin Med. 2021;10(21):5188. doi:10.3390/jcm10215188
- Pacheco C, Luu J, Mehta PK, Wei J, Gulati M, Bairey Merz CN. INOCA and MINOCA: Are women’s heart centres the answer to understanding and management of these increasing populations of women (and men)? Can J Cardiol. 2022;38(10):1611-1614. doi:10.1016/j.cjca.2022.06.016