Renato Tomioka is a leading expert in reproductive medicine and gynecologic surgery whose unique skills allow him to diagnose and treat some of the most impactful yet frequently overlooked conditions affecting women’s health. In this episode, Renato explores endometriosis and adenomyosis, explaining what these conditions are, why they often go undiagnosed for years despite affecting millions of women worldwide, and how advances in MRI and specialized ultrasound are transforming diagnosis beyond traditional surgical laparoscopy. He discusses the decision-making process behind hormonal therapy versus surgery, how treatment strategies change when fertility preservation is a priority, and where IVF fits into the care pathway for women with endometriosis, adenomyosis, or age-related fertility decline. Renato also examines the profound effects of female age on egg quality and quantity, including the accelerating rise in chromosomal abnormalities after age 35, highlights common mistakes in both surgical and fertility management, and shares promising developments on the horizon for treating these conditions and preserving fertility.
Follow Dr. Tomioka’s work: Instagram: Instagram: @dr.renatotomioka; Website: Renato Tomioka, M.D., Ph.D.
Subscribe on: APPLE PODCASTS | SPOTIFY | RSS | OVERCAST

“My mission for The Peter Attia Drive has always been to provide you with the most rigorous, evidence-informed insights on longevity. To do that without cluttering your experience with ads, we rely entirely on our premium members. If you’d like to support the work that makes this mission possible, consider becoming a premium member.”
– Peter
We discuss:
- Endometriosis: definition, prevalence, infertility risk, and theories of disease development [3:00];
- The biology of endometriosis: estrogen dependence, progesterone resistance, and tumor-like growth mechanisms [11:15];
- Adenomyosis explained: how it differs from endometriosis, why it develops, and its impact on reproductive health [15:15];
- Recognizing endometriosis and adenomyosis: the “6 Ds” of endometriosis and key differences in clinical presentation [20:30];
- Uterine fibroids: classification, symptoms, and the importance of fibroid location for bleeding and fertility [23:30];
- Understanding endometriosis pain: lesion-driven pain, nerve involvement, central sensitization, and the importance of early treatment [25:30];
- Endometriosis in young women: rising prevalence, delayed diagnosis, and barriers to care [29:30];
- Modern diagnosis of endometriosis: specialized ultrasound, MRI, and the decline of diagnostic laparoscopy [34:00];
- Clinical case example #1: Managing endometriosis in a young woman seeking pain relief while preserving future fertility [46:00];
- Clinical case example #2: Comparing treatment strategies for symptom control versus fertility [53:45];
- Endometriosis and fertility: the roles of age, embryo quality, IVF, and surgery [1:00:30];
- Clinical case example #3: Managing adenomyosis after failed IVF transfers to improve implantation and pregnancy outcomes [1:10:30];
- The funding gap in endometriosis research: disease burden, economic impact, and growing awareness [1:19:15];
- Clinical case example #4: Surgical decision-making in endometriosis—balancing pain relief, fertility preservation, and common treatment pitfalls [1:20:30];
- Common misconceptions about fertility: maternal age, embryo aneuploidy, the inefficiency of human reproduction, and the limits of IVF [1:26:00];
- Elective egg freezing: timing, success rates, the fertility funnel, and the tradeoffs of fertility preservation [1:32:00];
- Emerging fertility technologies: mitochondrial replacement, ovarian tissue preservation, stem-cell-derived eggs, and current limitations [1:43:00];
- The future of endometriosis treatment: new guidelines, biologic therapies, and unanswered questions about IVF [1:52:00];
- Why earlier diagnosis matters: reducing years of suffering from endometriosis and adenomyosis [1:55:30]; and
- More.
Show Notes
Endometriosis: definition, prevalence, infertility risk, and theories of disease development [3:00]
- First, Peter wants to talk about diseases of the uterus–most notably endometriosis, but also others
- Then he wants to talk about infertility and some of its treatments
- There’s an overlap between those two
Orient us to what endometriosis is
The first point is to remember the layers of the uterus
- The uterus has 3 main layers [shown in the figure below]:
1 – The outside layer, called the serosal [or the perimetrium]- 2 – The middle layer, which is the muscular layer called the myometrium
- 3 – The inner layer, where the embryo implants and the placenta develops, called the endometrium
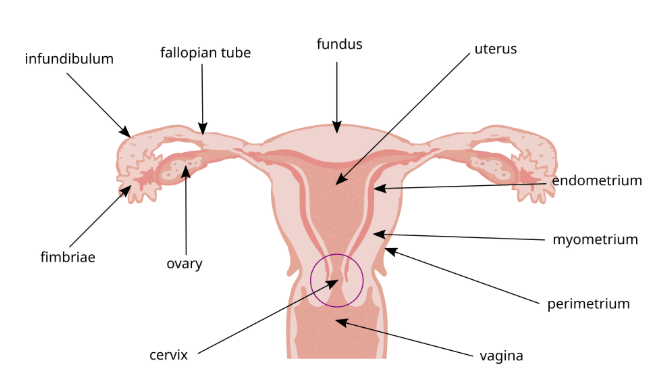
Figure 1. Anatomy of the uterus. Image credit: Wikipedia
The endometrium is very important because endometriosis is a chronic disease where an endometrial-like tissue, very similar to the endometrium [grows] outside the uterus
- Instead of being inside that layer, it goes into the fallopian tubes, on the ovaries, on the bowel, the bladder, sometimes the appendix, and even the diaphragm
Endometriosis is an important disease
- Around 10% of reproductive women have endometriosis, which means around 200 million women globally
- And if you look into the data of infertile women, about 30-50% of women, they can have endometriosis
- Endometriosis is causal
“If you have endometriosis, you have a chance of around 40% of being infertile.”‒ Renato Tomioka
Back to the 3 layers of the uterus
The endometrial layer is the inner layer of the uterus, and that’s the part that sheds every month during a woman’s cycle
- The endometrial layer is very dynamic depending on where you are in the cycle and the duration of the cycle
- The muscular layer is presumably functional
- During childbirth, it’s contracting the uterus
- The outer layer (the visceral peritoneum) doesn’t add much, but you can have endometriosis on that layer
- And then sometimes it infiltrates and transforms to external adenomyosis [he’ll talk about this later]
Do we have a sense of the features or characteristics that predict endometriosis?
How genetic is it and are there any environmental triggers for it?
- Endometriosis has a heritability of about 50%
⇒ If you have a first degree relative with endometriosis, you have about a 7x higher chance of having it
- A first degree relative would be a mother or a sister
- We know from twin studies that they share some genes, but they are not that penetrant
- Triggers may be pollution
A very important trigger is one we call “repetitive ovulatory menstruation”
- That means that every time a woman is menstruating, part of the menstrual flow goes back through the fallopian tubes into the pelvis
- We know this from surgeries
Peter adds, “It goes into the pelvis by going retrograde towards the ovary, but of course the fallopian tube doesn’t enter the ovary, it enters back into the pelvis.”
- Correct, remember the fimbriae (the distal part of the tubes [shown in the previous figure]), they are not directly connected to the ovary
- They are moving around and they can pick up the oocytes
- Most of the time, the oocyte is just on the surface of the ovary
- Sometimes it’s inside the pelvis on the cold side
- But the fimbriae can pick it up and that permits the fertilization inside the ampulla [not the isthmus, Renato misspoke here] (inside the middle, the longest and widest part of the uterine tube)
⇒ We know from old studies that around 90% of women have this retrograde menstruation
- Which is amazing–you would think: Why is that then just 10% have endometriosis?
- Because sometimes it’s not sufficient to have endometriosis, but it’s probably necessary in most cases
There are some nuances, but patients with endometriosis might have immune dysregulation
- The macrophages can’t cope with that overload of menstrual flow and endometrial tissue
- Also, if you have many, many, many years of retrograde menstruation, that can be bad
There’s an interesting story here–if you look 200 years ago
- A woman back then would have around 100 ovulatory cycles in their lifetime
- Menarche was about at the age of 16 (now it’s 12)
- First pregnancy, around 20 (now 30 or more)
- Breastfeeding for 2 years per child–and during that time, you’re not ovulating
- Women used to have 5-7 children
- So there was many times when they were not ovulating
If you compare that woman to a modern woman, it’s about a fourfold increase in this retrograde ovulatory menstruation–and this may be the main cause of why we are seeing much more endometriosis
- Not only diagnosing, but probably the prevalence is getting higher and higher
- So the Darwinian evolution didn’t anticipate this modern woman’s reproductive pattern that we have nowadays
Renato suggests, “That’s probably the best proxy for us to use and to think about using oral contraceptives or any hormonal treatment to block [ovulation and menstruation], to mimic that woman back then.”
Peter’s takeaway
- A woman 200 years ago would’ve had 100 ovulatory cycles in her lifetime, and that would’ve been driven by many changes
- She’s not cycling when she’s pregnant or breast feeding (you can do the math)
- A woman today might have 400 cycles (if uninterrupted or not intervened with), and every cycle produces the risk of retrograde flow
- Then when you get retrograde flow of blood into the fallopian tube, the macrophages that need to come and take care of it can’t always do the job
- So presumably, you’re creating a nidus for infection or something that the immune system is upset about
The biology of endometriosis: estrogen dependence, progesterone resistance, and tumor-like growth mechanisms [11:15]
If you look into mechanisms here [underlying endometriosis]
1 – Estrogen dependence
- The endometrial-like lesions, they produce by themselves estrogen
- They overexpress aromatase–there’s an upregulation in aromatase
- So sometimes just blocking the ovaries is not sufficient to block the disease
2 – We also have this progesterone resistance
{end of show notes preview}
Would you like access to extensive show notes and references for this podcast (and more)?
Check out this post to see an example of what the substantial show notes look like. Become a member today to get access.

Renato Tomioka, M.D., Ph.D.
Dr. Renato Tomioka is a Brazilian gynecologist specializing in reproductive medicine, minimally invasive surgery, and gynecologic endocrinology. He graduated from the University of São Paulo School of Medicine, completed his residency in Obstetrics and Gynecology at the Hospital das Clínicas of University of São Paulo, and holds a PhD from the same institution. He is also certified in minimally invasive surgery and robotic surgery. Dr. Tomioka practices at Clínica Tomioka and is a partner at Clínica VidaBemVinda, part of Fertgroup, Brazil’s leading assisted reproduction center. He is also the Director of the Scientific Board at Centeni, a healthcare start up in Brazil. [RenatoTomioka.com]
Facebook: RenatoTomioka, M.D.
Instagram: dr.renatotomioka
YouTube: @DrRenatoTomioka
Website and clinic: Renato Tomioka, M.D., Ph.D.



