
See Full Series:
-
- (September 19, 2021) Does low cholesterol cause cognitive impairment? | Part I
- (September 26, 2021) Does low cholesterol cause cognitive impairment? | Part II
- (February 2, 2022) Low LDL cholesterol and neural development | Part III
Last week I discussed the theoretical possibility that lipid-lowering drugs might negatively impact cognitive function, specifically, whether PCSK9 inhibitors had such an impact. The answer appears to be no, at least according to studies addressing this question. While PCSK9 inhibitors are the most potent drugs to lower apoB and LDL-C, they are not the most common—a distinction that belongs to a class of drugs you are no doubt familiar with: statins. Is it possible that statins may alter brain cholesterol synthesis in a way that is unique to their mechanism of action (and distinct from all other pharmacological mechanisms that lower cholesterol)?
Based on their mechanism of action, one of the biggest concerns with potent statin use is that it may increase the risk of cognitive impairment, dementia, or hemorrhagic strokes. Fortunately, after decades of research and billions of patient-years of use data, it doesn’t appear that people taking statins are at greater risk of these conditions. In fact, population studies actually suggest that statin use is associated with a reduced incidence of dementia, but observational studies like these are incapable of determining a cause-and-effect relationship. Why would statins reduce Alzheimer’s disease (AD) risk? Perhaps because there’s a reduction in vascular risk when taking statins, and there’s likely a vascular component to AD. If you recall from last week, there’s a widely held notion that what is good for the heart is good for the brain. This may be particularly relevant in the context of vascular health. (Listen to my podcast with Francisco Gonzalez-Lima where we explore this topic in more detail.) One of the limitations to population-level observational studies is that they might not tell you the whole story about individual differences. The old adage, you can still drown in a body of water that is, on average, 3 feet deep holds—some parts are likely much deeper. Similarly, just because on average, statins seem to reduce the risk of dementia, it does not mean we should assume this is true across the board. Is it still possible that statins might over-suppress cholesterol synthesis in the brain in at least some individuals and increase the risk of cognitive impairment in this subset?
If you recall from Part I, cholesterol is critical to normal brain function, but it’s unlikely that plasma cholesterol affects cognition because there’s no relationship between plasma cholesterol and tissue pools of cholesterol. However, it’s still possible that cholesterol levels in the brain can affect cognition, and because some statins have a variable ability to cross the blood brain barrier (BBB) and reduce cholesterol synthesis (unlike PCSK9 inhibitors or ezetimibe which have no effect on synthesis) potentially lowering brain cholesterol below the level required for normal cognitive functioning. At least that’s the question we want to explore. First, a word on cholesterol synthesis.
There are two pathways for cholesterol to be synthesized within each cell in your body. One is called the Kandutsch-Russell pathway, which is believed to be the predominant pathway, where lathosterol is the penultimate sterol (i.e., the molecule that is converted into cholesterol via the final step of this pathway). The other is called the Bloch pathway, which is thought to be by some a less prominent path, where desmosterol is the penultimate sterol. Since cholesterol is ubiquitous, and highly recycled, a clever way to measure cholesterol synthesis is to measure direct levels of lathosterol and desmosterol. There is some evidence that the Bloch pathway is the predominant pathway in the brain, especially during infancy and childhood. This raises the hypothesis that desmosterol, specifically, may serve as a biomarker of cholesterol synthesis in the brain.
It turns out that the brain tissue in AD patients are depleted in desmosterol and that desmosterol levels are relatively low in the cerebrospinal fluid (CSF) compared to individuals without AD. Unfortunately, it’s not especially pleasant or convenient to get a spinal tap to assess the desmosterol levels bathing your brain.
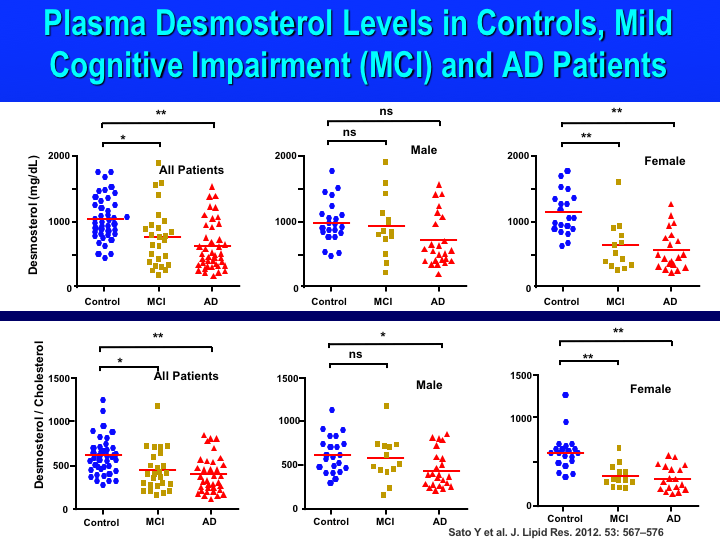
So, instead we can look at plasma levels of desmosterol which are, fortunately, highly correlated with CSF levels. A 2012 study was the first to report decreased plasma desmosterol levels in patients with AD and mild cognitive impairment (MCI). MCI is the stage between the expected cognitive decline associated with aging and the more severe decline of dementia. The investigators in this study measured cholesterol and desmosterol in both the plasma and CSF in Caucasian patients and looked at the relationship between the two locations. Their analysis revealed that the desmosterol-to-cholesterol ratio in the CSF correlated well with its plasma ratio, suggesting that plasma levels of desmosterol reflect brain sterol synthesis and metabolism. In the same paper, the investigators found a significant change in desmosterol and the desmosterol-to-cholesterol ratio in the plasma of both MCI and AD patients compared with healthy elderly controls, as shown in the Figure below. They also found a significant correlation with worsening Mini-Mental State Examination (MMSE) scores, which is a widely-used test of cognitive function among the elderly.
Figure (from Sato et al., 2012). Plasma desmosterol levels and plasma desmosterol-to-cholesterol ratios in controls, mild cognitive impairment (MCI), and Alzheimer’s disease (AD) patients.
In 2015, the same group from this 2012 paper measured plasma desmosterol and cholesterol samples from about 400 Japanese participants — approximately half of which had AD with the other half serving as healthy controls — and followed a subset of them over a range of two to three years to see if there was an association between the desmosterol-to-cholesterol ratio and cognitive decline in patients with AD over time. The investigators found that the plasma desmosterol-to-cholesterol ratio was reduced in Japanese AD patients. They also found that after two to three years of follow-up, the ratio was relatively stable in normal controls whereas it significantly decreased in AD patients. In those with MCI or AD with a more rapid disease progression, there was a more rapid decline in the plasma desmosterol-to-cholesterol ratio compared with those with slower progression. The change in the plasma desmosterol-to-cholesterol ratio also tracked with the change in the MMSE score over time. The more pronounced the decrease in the plasma desmosterol-to-cholesterol ratio, the lower the MMSE score, the greater the cognitive impairment.
One of the most common causes of reduced desmosterol is statin therapy. Statins can cross the BBB — and while the data is conflicting — a recent study confirmed the hypothesis that lipophilic versions including simvastatin (Zocor) and atorvastatin (Lipitor) may more easily cross the BBB than hydrophilic ones including rosuvastatin (Crestor) and pravastatin (Pravachol), and therefore may inhibit cholesterol synthesis in the brain. Is low desmosterol a cause of cognitive impairment and dementia or the result of it? The short answer is we don’t know. What we do know is that cholesterol is critical to brain function and there are observational studies like the ones above (and more recent ones) suggesting low plasma desmosterol is a biomarker for MCI and AD. Unfortunately, the 2012 and 2015 papers discussed above don’t include patients on statins, which would be helpful for us to elucidate any links between statin use, desmosterol levels, and cognitive decline. It may sound cliché to hear this, but more, and better, research is needed to understand whether statins have an effect on cognition or neurological disorders like AD, in at least a subset of users.
From a clinical perspective, low desmosterol levels in patients with cognitive symptoms may serve as an indication that cholesterol synthesis is over-suppressed and the statin dose should be decreased (or stopped altogether in favor of a different drug class). We don’t like to see absolute concentrations of desmosterol below 0.8 mg/L in our patients. We also treat patients with one or two copies of the APOE e4 alleles or a family history of dementia with kid gloves and make sure they have a desmosterol level greater than 1.0 mg/L. While we don’t know for sure whether low desmosterol from statin use increases the risk of dementia, a personalized approach may be necessary. Population data are helpful and RCTs are important, but as any doctor will tell you, the only patient that matters is the one in front of you.



