If you’re a regular listener of The Drive podcast or reader of our newsletter, you’re aware of a powerful class of lipid-lowering therapies known as PCSK9 inhibitors. PCSK9 (proprotein convertase subtilisin/kexin type 9) is a protein that binds to receptors for low-density lipoprotein (LDL) on the surface of liver cells and directs them to be disassembled inside the cell, thus keeping the steady-state concentration of LDL receptors low. By hindering the action of PCSK9 in different ways, PCSK9 inhibitors boost the number of LDL receptors on the liver cell surface, allowing them to clear more LDL particles from the plasma.
For instance, in the Phase III trial of evolocumab/Repatha®, the drug slashed LDL cholesterol (LDL-C) concentration by 59% compared with placebo, despite the fact that the subjects’ LDL-C was already a respectably low median of 92 mg/dL, thanks to aggressive use of statins.1 This potent reduction led to a rapid fall in health crises related to atherosclerotic disease (ASCVD): in a little over 2 years, evolocumab reduced the risk of death from cardiovascular causes, heart attacks, strokes, hospitalization for unstable angina, or coronary revascularization (procedures like bypass surgery or angioplasty) by 15% (HR 0.85; 95% CI 0.79 to 0.92; P<0.001).1
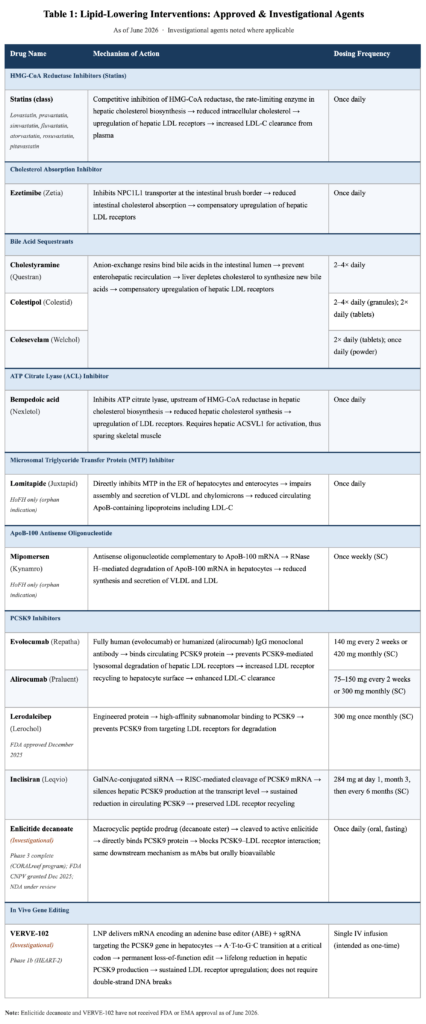
The first PCSK9 inhibitor was approved in 2015; since then, drug developers have invented multiple additional drugs in this class, targeting PCSK9 in several distinct ways (see Table 1).
But we are about to enter a new era.
PCSK9 is no longer an interesting biological target. We solved that problem more than a decade ago. The interesting question today is whether we can safely and permanently reproduce the effect of lifelong PCSK9 deficiency with a one-time intervention.
Let’s start at the beginning.
Mystery, mutations, medicine
In 2003, Nabil Seidah at the Clinical Research Institute of Montreal discovered a new protein that he initially called NARC-1.2 He found that the gene was overwhelmingly expressed in the liver, with a smaller amount in the testicles and even less in the kidneys. But as he and colleagues wrote, “no information is available on NARC-1 activity, cleavage specificity, cellular and tissue expression, and biological function.”
With the limited tools available at the time, one thing that he could say was that the gene responsible for it was located somewhere within a defined region of chromosome 1. And coincidentally, French scientists Marianne Abifadel and Catherine Boileau had spent the previous 5 years searching this same region for the mutation responsible for the astronomically high levels of LDL cholesterol (LDL-C) in some families. When Seidah reached out to Boileau and suggested that NARC-1 might be the mystery gene, she told him he was crazy. Seidah challenged her to a wager: a bottle of champagne said that the gene was NARC-1. Within two weeks, Boileau happily conceded the bet.3
When Seidah and Boileau’s team jointly published a paper identifying the mutation,4 the journal editors insisted on a new name. Today, we know that protein as PCSK9.
Helen Hobbs, a professor at the University of Texas Southwestern Medical Center, learned that forcing the liver to produce high levels of PCSK9 caused the LDL receptor to disappear from the liver cells’ surface. This explained why Boileau’s patients had such alarmingly high levels of LDL-C: without that receptor, their livers could not capture circulating LDL particles and dispose of them. It was as if you had torn up all the exits from a major highway, but cars just kept ramping onto it: with no way to get off the highway, the vehicles pack together more and more densely, and cars start driving on the median and crashing into the side rails.
So Hobbs went looking for the opposite: mutations that would disable PCSK9, leading to a thicket of LDL receptors on the liver’s surface and rock-bottom LDL-C (or apolipoprotein B (apoB), the true target of therapy for which LDL-C is just a surrogate). And sure enough, she found them: four mutations that completely disrupted PCSK9, and a healthy, fertile, 40-year-old aerobics instructor with an LDL-C of 14 mg/dL.3,5 Carriers of less severe mutations had a 28% reduction in LDL-C, and an astonishing 88% reduced risk of heart attack, death from cardiovascular causes, or revascularization.6
These discoveries rapidly led to medicines that interfere with PCSK9 in different ways. The first of these were the monoclonal antibodies alirocumab/Praluent® and evolocumab/Repatha®, which bind to PCSK9 and prevent it from interacting with the LDL receptor. Then came inclisiran/Leqvio®, which is a small interfering RNA (siRNA) that targets PCSK9 protein production: when the cell produces a “working copy” (mRNA) of the gene for PCSK9, which contains the instructions to build PCSK9 protein, inclisiran binds to it and recruits cellular machinery that destroys it before the protein can be produced. So where the antibodies disable PCSK9 protein, inclisiran prevents PCSK9 from being produced from the gene that encodes it.
Drug companies have subsequently come up with even more novel strategies to disable PCSK9, including binding it using small molecule drugs (enlicitide decanoate, still in development) or proteins (Lerodalcibep/Lerochol®) instead of antibodies (Table 1).
But now we have early human data on an even more sophisticated approach: disable the PCSK9 gene itself, so it never produces the protein. Effectively, give the patient the same mutations that Hobbs’ most remarkable patients bore, giving them the same rock-bottom apoB levels and protection from ASCVD for life.
Our research team spends hundreds of hours each month vetting studies and distilling dense literature to deliver evidence-informed insights on health and longevity. If you find value in our work, consider becoming a premium member and supporting our mission.









From genes to medicines … and back again
In the New England Journal of Medicine, Vasfai and colleagues have reported the preliminary safety and efficacy of VERVE-102, Eli Lilly’s gene-editing therapy that disables patients’ PCSK9 genes.7 At its core, VERVE-102 comprises a “seek” component and a “destroy” component. The “seek” module (called a guide RNA (gRNA)) is a genetic sequence whose “letters” (bases) are the binding partners for each “letter” in the PCSK9 gene, like the teeth of a key mirror the pins of a tumbler lock. This allows the whole construct to precisely identify and bind to the PCSK9 gene. The “destroy” component is a DNA-cutting enzyme that damages one specific “letter” in the gene (an adenine—on which basis it is called an adenine base editor (ABE)).
With this one change, the PCSK9 gene is rendered permanently non-functional, and no PCSK9 protein is produced—like the more extreme mutations in Hobbs’ patient cohort. The whole construct is packaged into a lipid nanoparticle that ensures that almost all the payload is delivered to the liver, where disrupting PCSK9 allows LDL receptors to stay on the surface of cells longer, leading to remarkably low levels of LDL-C.
In the Phase I trial for VERVE-102 published late in May, researchers reported that the gene therapy profoundly lowers LDL-C.7 To participate in the trial, volunteers had to have either established premature coronary artery disease or a heterozygous familial hypercholesterolemia (FH), a genetic disorder that causes wildly high LDL-C. Additionally, subjects had to have a fasting LDL-C of at least 70 mg/dL, despite being on the maximum dose of a statin they could tolerate (with or without ezetimibe). Despite this aggressive use of medication, the average LDL-C in the 35 participants was 129±42 mg/dL—well above the acceptable range even for people with no other risk factors, let alone for this high-risk group.
Subjects received one of 6 doses of VERVE-102 as a single intravenous infusion. Higher doses meant more liver cells genetically modified, so less PCSK9 protein produced and more intensive lipid lowering. After 28 days, circulating PCSK9 protein levels fell from 51% at the lowest dose to 88% at the highest dose. And despite their LDL already being held down as well as possible with standard-of-care medications, the resulting LDL-C reductions ranged from 9% up to a whopping 62%, respectively, corresponding to an absolute drop of 78 mg/dL LDL-C at the highest dose. Although not all patients had reached 1 year of followup at the time of publication, data from those subjects who had showed that the reductions were durable for at least that long.7
The perfect compound-interest account
You might wonder whether an approach as biotechnologically advanced and expensive as gene therapy is actually necessary to achieve control of LDL-C. Indeed, reductions in LDL-C reported in the VERVE-102 trial are similar to, and perhaps not quite as impressive as, the results of the Phase III trial of evolocumab: at 48 weeks, evolocumab reduced LDL-C by 59% as compared with placebo, despite the subjects having started from a median of 92 mg/dL—an even lower baseline than the one in the VERVE-102 trial.1
The big advantage of a gene therapy approach is that it would keep apoB down to exceptionally low levels continuously, for the rest of a person’s life. Although a person could in principle obtain the same consistent reductions of apoB through exacting adherence to an existing PCSK9 inhibitor regimen, such ideal dosing is often not achieved in the hurly-burly of people’s lives. Studies show that somewhere between 30 and 50% of people prescribed a lipid-lowering therapy stop taking it within a year,8,9,10 and many people fail to take at least 80% of their doses.10 And when people discontinue lipid-lowering therapies11,12,13,14 don’t consistently take their medicine,15 or have trouble with their insurance,16 their risk of having a heart attack or a stroke rises, even if they had not previously suffered one.14
Simply reducing the number of times a person has to take their medication is already enough to improve adherence and reduce discontinuation. For instance, inclisiran only has to be dosed twice a year after the first two injections, whereas PCSK9 inhibitor antibodies like alirocumab and evolocumab need to be dosed twice a month. A study that found that less than a third of people on inclisiran discontinued their medication over their first year, versus 45% of people on antibodies; they also kept up with their dosing for 77% of the year on average, versus 68% for people on the antibodies.9
Adherence would likely be even greater in people’s second year of therapy, with the two front-loaded infusions out of the way. Inclisiran’s twice-annual dosing leaves fewer opportunities for insurance snags, pharmacy shortages, short-term financial squeezes, travel mishaps, refrigeration problems, and simple forgetfulness to keep a person from taking their dose on time. A therapy that disables the PCSK9 gene would allow a person to stick to their medicine permanently, no matter what else came up in their life.
People who are born with the mutations that inspired PCSK9 inhibitors enjoy perfect, lifelong adherence to their inborn PCSK9 inhibition: their apoB is low from the day they are born to the day they die, whereas most people only get on lipid-lowering therapies in midlife or beyond, and (as we’ve seen) don’t always stick to their medication or take it on time. This reduction in lifelong integrated apoB exposure (or “LDL years,” analogous to “pack years” of smoking) explains why lowering LDL-C with a statin by 39 mg/dL over the course of a 5-year trial reduces the risk of heart attacks and strokes by “only” 22%,17 whereas people who carry minor PCSK9 gene variants that lower LDL-C by the same amount (to about 100 mg/dL) enjoy an 88% lower lifetime risk of heart attack, death from ASCVD, or revascularization.6
The same compounding effect is evident for the duration of therapy. In FOURIER, the pivotal trial for evolocumab, the PCSK9 inhibitor reduced the risk of cardiovascular death, heart attack, or stroke in very high risk patients who already had cardiovascular events by 16% during the first year, but by 25% for the remaining 1.2 (median) years of followup of the trial.1
When the trial participants were followed up for an additional 5 years in the FOURIER Open-Label Extension (FOURIER-OLE), the people originally randomized to evolocumab continued to benefit from those years of early treatment: even though the former placebo group patients were themselves given evolocumab during the extension, those who had received the drug during the FOURIER trial itself continued to have 20% lower risk of these outcomes than the former placebo group.18 Having been on the drug for the first 2.2 years, the FOURIER evolocumab patients went into the extension with fewer “LDL years” and a lower burden of disease, and that saved them from bad outcomes suffered by those who got protection late.
For whom, and when?
Should VERVE-102 show safety and the anticipated efficacy in subsequent Phase II and III trials and ultimately be licensed, it will likely not be indicated for primary prevention of ASCVD, or even for secondary prevention of heart attacks and strokes in people who are otherwise not remarkable in their risk profile. Instead, the gene therapy will likely initially only be indicated for people like those in the Phase I trial: people with FH, or who have developed extensive ASCVD at a relatively young age and who don’t respond adequately to existing lipid-lowering medicines. And while physicians can in principle use their judgements to prescribe therapies for purposes other than their labeled indications, it is unlikely that many will initially do so for lower-risk patients, or that insurance will cover it—and the price will be prohibitive.
When (if) VERVE-102 first hits the market, this will be a good balance of risks. People such as those in the Phase I trial need the strongest and most consistent protection against apoB-containing lipoproteins, and gene therapy may well be the best way to achieve that goal. But the risk calculus looks different for people with mildly elevated risk, or who are at low risk by conventional standards but want to nearly eliminate their risk of ASCVD. While the advantages of perfect, potentially lifelong PCSK9 inhibition via gene therapy are evident, the known and still unknown risks that will remain when (if) VERVE-102 is licensed argue for caution in lower-risk people until we have years of postmarket surveillance to assure us of VERVE-102’s long-term safety.
The gene edit is likely forever: this is one of its strong advantages, but also a source of risk. While base editors that convert an adenine to guanine do exist (this was the genetic “letter” switch in VERVE-102), none have been developed that can do the reverse, and there do not appear to be any efforts underway to develop a means to reverse the VERVE-102 edit should something go awry.* The fact that people with fully disabling PCSK9 mutations enjoy an exceptionally low risk of ASCVD and suffer no ill effects suggests that a gene therapy such as VERVE-102 would be safe in the long term; however, VERVE-102 does not itself replicate any of the specific mutations seen in patients, which leaves open the possibility that some long-term effect not seen in people who get their PCSK9 mutations the old-fashioned way may at some point emerge—perhaps only in a subset of people that will only be identified after it has been out on the market and in relatively wide use for many years.
Similarly, the short-term observations reported in the new paper preclude an assessment of the potential risks of off-target editing or editing in unintended tissues, and any such problems may only emerge after years of postmarket surveillance.
And the gene therapy payload itself is not the only possible source of risk. Prior to VERVE-102, Verve Therapeutics originally trialed VERVE-101, a version of the therapy packaged in a different liver-targeting nanoparticle. The trial had to be halted earlier after one out of six patients developed Grade 3 drug-induced elevations of liver enzymes and a Grade 3 crash in their platelets (cells required for blood clotting).19 (Grade 3 events are severe or medically significant enough to often require hospitalization or significant intervention, but are not immediately life-threatening). In the Phase I trial of VERVE-2 itself, there was one case of Grade 3 aspiration pneumonitis in a participant who received one of the lower doses. It occurred roughly 2 weeks after the infusion and was not judged likely to be related to therapy, but at this early stage we can’t say with confidence.
Today and tomorrow
These questions will be resolved with greater confidence in forthcoming Phase II and III trials of VERVE-102. In the meantime, people at low to moderate risk and seeking potent protection against the First Horseman can look to existing medications that (in the case of PCSK9 inhibitors) have already been trialed in tens of thousands of subjects that have been followed up formally for up to a decade, and nearly 80,000 more people observed “in the wild” for just as long.20 Similarly, we have hard outcomes data on 174,149 subjects at relatively low risk of ASCVD that have received statins in clinical trials.21 Within the last six months, PCSK9 inhibitor drugs were shown for the first time to reduce the composite of death from coronary heart disease, myocardial infarction, or ischemic stroke in people who had not suffered any of these outcomes previously,22 and also in people without significant known pre-existing atherosclerosis but with diabetes.23
It will be a decade or more before we have such evidence in hand for VERVE-102. Whether VERVE-102 clears the bar or another succeeds in its place, it opens up a future of gene therapies so safe and effective that they will be the standard of care for otherwise-healthy people working to resist the ravages of aging and age-related disease. For today, we have many tools at our disposal—exercise, sleep hygiene, an abundance of healthy foods (and tools to avoid overeating them), and highly effective medications. Judicious and consistent use of these tools can greatly increase our odds of living longer and better while we await technological advances that might make some of them—and some of today’s greatest killers—obsolete.
* To put into context how little we know about gene therapy in humans, consider that the longest reported duration of followup on any gene therapy in the liver in humans is 3 years.24 So the true durability of VERVE-102 will only emerge with followup in real time, with each year of maintenance in living recipients extending the record for its persistence.
For a list of all previous weekly emails, click here.
References
- Sabatine MS, Giugliano RP, Keech AC, et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med. 2017;376(18):1713-1722.
- Seidah NG, Benjannet S, Wickham L, et al. The secretory proprotein convertase neural apoptosis-regulated convertase 1 (NARC-1): liver regeneration and neuronal differentiation. Proc Natl Acad Sci U S A. 2003;100(3):928-933.
- Hall SS. Genetics: a gene of rare effect. Nature. 2013;496(7444):152-155.
- Abifadel M, Varret M, Rabès JP, et al. Mutations in PCSK9 cause autosomal dominant hypercholesterolemia. Nat Genet. 2003;34(2):154-156.
- Zhao Z, Tuakli-Wosornu Y, Lagace TA, et al. Molecular characterization of loss-of-function mutations in PCSK9 and identification of a compound heterozygote. Am J Hum Genet. 2006;79(3):514-523.
- Cohen JC, Boerwinkle E, Mosley TH Jr, Hobbs HH. Sequence variations in PCSK9, low LDL, and protection against coronary heart disease. N Engl J Med. 2006;354(12):1264-1272.
- Vafai SB, Täubel J, Ashdown T, et al. In vivo base editing of PCSK9 with VERVE-102 for hypercholesterolemia. N Engl J Med. 2026;(NEJMoa2601283). doi:10.1056/NEJMoa2601283
- Navar AM, Electricwala B, Multani JK, et al. Lipid management in United States commercial and Medicare enrollees with atherosclerotic cardiovascular disease: Treatment patterns and low-density lipoprotein cholesterol control. Am J Cardiol. 2025;242:1-9.
- Popadic L, Ma X, Ali Y, et al. Treatment patterns among early inclisiran vs anti–PCSK9 mAbs users: A retrospective analysis of US claims databases. J Clin Lipidol. 2024;18(4):e515-e516.
- Ofori-Asenso R, Jakhu A, Zomer E, et al. Adherence and persistence among statin users aged 65 years and over: A systematic review and meta-analysis. J Gerontol A Biol Sci Med Sci. 2018;73(6):813-819.
- Accessed June 2, 2026. https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2780952
- Blanco M, Nombela F, Castellanos M, et al. Statin treatment withdrawal in ischemic stroke: a controlled randomized study. Neurology. 2007;69(9):904-910.
- Heeschen C, Hamm CW, Laufs U, et al. Withdrawal of statins increases event rates in patients with acute coronary syndromes. Circulation. 2002;105(12):1446-1452.
- Thompson W, Morin L, Jarbøl DE, et al. Statin discontinuation and cardiovascular events among older people in Denmark. JAMA Netw Open. 2021;4(12):e2136802.
- Mazhar F, Hjemdahl P, Clase CM, et al. Intensity of and adherence to lipid-lowering therapy as predictors of major adverse cardiovascular outcomes in patients with coronary heart disease. J Am Heart Assoc. 2022;11(14):e025813.
- Myers KD, Farboodi N, Mwamburi M, et al. Effect of access to prescribed PCSK9 inhibitors on cardiovascular outcomes. Circ Cardiovasc Qual Outcomes. 2019;12(8):e005404.
- Cholesterol Treatment Trialists’ (CTT) Collaboration, Baigent C, Blackwell L, et al. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376(9753):1670-1681.
- O’Donoghue ML, Giugliano RP, Wiviott SD, et al. Long-term evolocumab in patients with established atherosclerotic cardiovascular disease. Circulation. 2022;146(15):1109-1119.
- Philippidis A. Verve pauses enrollment in base editing trial after adverse events. Hum Gene Ther. 2024;35(9-10):313-316.
- Huang CH, Wang SI, Fan FS, Lu HJ, Wei JCC. Association of PCSK9 inhibitors with mortality: insights from a retrospective cohort analysis. Eur Heart J Cardiovasc Pharmacother. 2024;10(6):505-514.
- Cholesterol Treatment Trialists’ (CTT) Collaborators, Mihaylova B, Emberson J, et al. The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular disease: meta-analysis of individual data from 27 randomised trials. Lancet. 2012;380(9841):581-590.
- Bohula EA, Marston NA, Bhatia AK, et al. Evolocumab in patients without a previous myocardial infarction or stroke. N Engl J Med. 2026;394(2):117-127.
- Marston NA, Bohula EA, Bhatia AK, et al. Evolocumab to reduce first major cardiovascular events in patients without known significant atherosclerosis and with diabetes: Results from the VESALIUS-CV trial: Results from the VESALIUS-CV trial. JAMA. 2026;335(16):1400-1407.
- Intellia Therapeutics Presents Positive Longer-Term Phase 1 Data of Nexiguran Ziclumeran (nex-z) in Patients with Transthyretin (ATTR) Amyloidosis with Cardiomyopathy. Intellia Therapeutics, Inc. November 10, 2025. Accessed May 31, 2026. https://ir.intelliatx.com/news-releases/news-release-details/intellia-therapeutics-presents-positive-longer-term-phase-1-data