In this episode, Peter explores the critical topic of breast cancer screening, examining why thousands of women continue to die from breast cancer each year despite the availability of effective screening tools. He explains the strengths and limitations of current screening strategies, reviews the recommendations from major medical organizations, and discusses why screening guidance can often seem confusing or contradictory. Peter outlines a practical framework for understanding breast cancer risk and personalizing screening decisions, including when to begin screening, how frequently to screen, and which imaging modalities may be most appropriate based on an individual’s risk profile. Throughout the episode, he emphasizes that while population-based guidelines provide an important foundation, optimizing outcomes requires a more personalized approach aimed at helping women make informed screening decisions that can improve the chances of early detection and successful treatment.
Subscribe on: APPLE PODCASTS | SPOTIFY | RSS | OVERCAST
“My mission for The Peter Attia Drive has always been to provide you with the most rigorous, evidence-informed insights on longevity. To do that without cluttering your experience with ads, we rely entirely on our premium members. If you’d like to support the work that makes this mission possible, consider becoming a premium member.”
– Peter
We discuss:
- Why women still die from breast cancer: the benefits of screening, the problem of under-screening, and the need for risk-based screening strategies [1:45];
- Current screening recommendations, why they differ between organizations, and the importance of personalized screening decisions [6:30];
- A framework for personalizing screening [8:45];
- Assessing baseline breast cancer risk: genetics, family history, breast density, lifestyle factors, and the role of risk calculators in personalized screening [9:30];
- Balancing cancer detection and false positives: how breast cancer risk influences screening intensity and imaging choices [17:45];
- Mammography as the foundation of breast cancer screening: detecting ductal carcinoma in situ (DCIS) and the advantages of 3D versus 2D mammography [21:00];
- MRI for high-risk women: the benefits of supplemental screening, abbreviated MRI, and the emerging role of contrast-enhanced mammography [23:00];
- The role of ultrasound: supplemental cancer detection, diagnostic evaluation, and limitations compared with mammography and MRI [26:00];
- Choosing the right breast cancer screening strategy: imaging modality selection, screening hierarchies, and the importance of imaging center quality [28:00];
- How often should you screen for breast cancer? [30:15];
- At what age should you start screening? [37:30];
- Breast cancer in younger women: aggressive tumor biology, BRCA-related risk, breast density, and individualized decisions about when to begin screening [41:45];
- Inflammatory breast cancer, the limitations of screening mammography for symptomatic disease, and the importance of promptly evaluating new breast symptoms in both women and men [44:45];
- From risk assessment to personalized screening: a practical framework for reducing breast cancer mortality through earlier and more effective detection [46:30]; and
- More.
Show Notes
*Notes from intro:
- Today, we’re diving into breast cancer screening
- Why women are still dying from breast cancer despite effective screening tools
- Where current screening strategies fall short
- And how to think about personalizing your own screening
This episode is really about one central question: How do you give yourself the best possible chance of not dying from breast cancer?
- As we consider this to be a really important public service announcement, the full episode and the detailed show notes for this discussion will be available to everyone, regardless of whether or not you’re a premium subscriber
Why women still die from breast cancer: the benefits of screening, the problem of under-screening, and the need for risk-based screening strategies [1:45]
Breast cancer statistics
- Most of us have heard that terrible statistic: about 1 in 8 women will develop invasive breast cancer over the course of their lifetime
- In the United States, roughly 42,000 women die every year from this disease
- That makes it one of the leading causes of cancer death behind only lung, colorectal, and pancreatic
- [the table below summarizes the top 10 cancer deaths in both sexes]
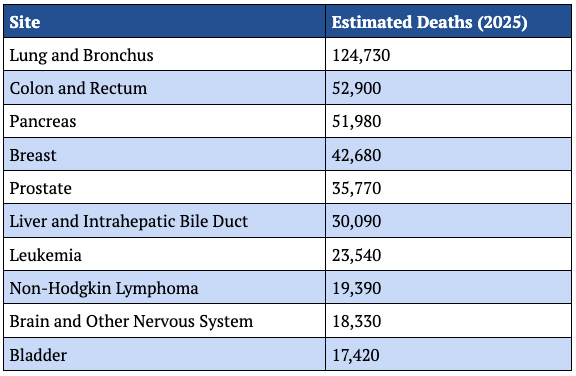
Figure 1. Top 10 cancer sites responsible for death in 2026. Source: The Surveillance, Epidemiology, and End Results Program (SEER)
- And yet, despite how common and consequential this disease is, many women have questions about screening
- Including when it should start, how often to do it, and what factors actually matter
- Even women who have looked at the guidelines often come away more confused than before
- Because the guidance differs between organizations
- And it’s also shifted over time
That confusion has real consequences because breast cancer screening works
- Cancers found through screening are more likely to be caught early before they’ve spread when treatment is easier and outcomes are better
- And that stage shift (as it’s called) matters enormously
- When breast cancer is caught at stage I, the 10-year survival is over 96%
- By stage IV, 5-year survival is only around 30%
- [the figure below shows the stages of cancer]
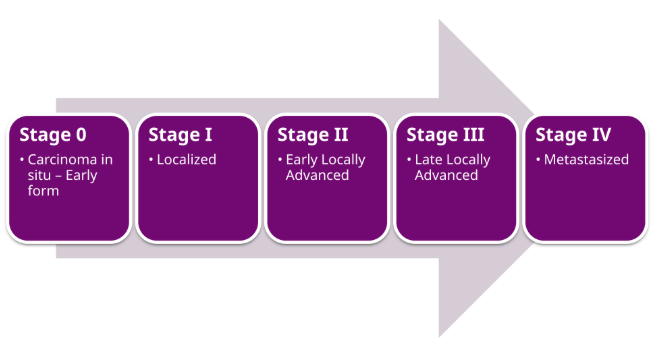
Figure 2. Cancer staging. Image credit: Wikipedia
⇒ It’s no surprise then that women who screen regularly are up to 40% less likely to die from the disease
Screening is not without trade-offs
- Overdiagnosis of lesions that would never progress to cancer can increase healthcare burden with no real benefit, and remains an area of ongoing uncertainty
- We’ll get into these considerations later, but they do not negate the core point:
Screening is one of the most effective tools we have for reducing breast cancer mortality
- And if you’re optimizing for your individual risk of dying from breast cancer
- Not population efficiency
- Not total societal cost
- But your own outcome–the default should be to err on the side of more effective screening and certainly not less
Which raises the obvious question: If screening works so well, why are so many women still dying from breast cancer every year?
- Part of the answer is biology
Some breast cancers are simply more aggressive than others
- They grow quickly, they spread early, and can be difficult to intercept even with a very good screening system
- Some back of the napkin math suggests that somewhere around 7-10% of cases are the ones we are unlikely to catch even with perfect screening
- But those biologically aggressive cases are NOT the only reason this disease is still taking so many lives
- A major, and much more solvable part of the problem, is far more mundane
We are still under screening
- Peter doesn’t just mean that some women never get a mammogram, though that is certainly part of it
Even among women who have been screened before, screening may be inconsistent
- Roughly a third of women over 40 have not had a mammogram in the past 2 years
- And even among women aged 50-74, where the evidence is most universally agreed upon, about 20% are not up-to-date
Under screening has 2 layers
- 1 – Most women are not even getting routine mammography at the right time
- 2 – The second is more nuanced: some women are getting screened, but not with the right strategy for their risk profile
Peter explains, “This is one statistic that I think captures this perfectly. According to the criteria laid out by major screening guidelines, at least 9% of women meet the threshold for breast MRI as part of their screening protocol. And yet the actual utilization rate is just 0.4%.”
- It’s not that MRI is unproven or controversial for these women, this is a pure execution failure
- We already know who these high-risk women are, and we already have a tool that materially improves detection
- We’re simply not connecting the two
Goal for this episode
- What Peter wants to do today is NOT simply tell you to get screened (you already know that)
- He wants to give you a practical framework for smarter screening
- One that starts with understanding your actual risk and helps you make informed decisions about when to start, how often to screen, and what imaging to use
- Population guidelines form a great starting point, but they’re not the finish line
- To get there, we need to start with the guidelines themselves
- What do the major organizations actually recommend and how should we talk about personalizing them?
Current screening recommendations, why they differ between organizations, and the importance of personalized screening decisions [6:30]
If you’re confused about breast cancer screening, you’re not alone
- A recent survey found that roughly 50% of women aren’t sure when to start mammography
- And frankly, that confusion is understandable
- The guidance has shifted multiple times over the past two decades, most recently in 2024
- There are several organizations that publish screening recommendations and they do NOT all agree
- Rather than walking through all of them individually, Peter will first give you the composite picture of the most rigorous guidelines
- Included at the end of these notes is a full comparison table
The big picture
- Every woman should have a formal risk assessment by about the age of 25
- If you are average risk, annual mammography should begin at 40
- If you are high risk (and Peter will define that in a minute), you may need an MRI and eventually mammography much earlier
- And screening should continue for as long as you would be willing to pursue treatment if cancer were found
- That composite comes from groups like the American Cancer Society, the National Comprehensive Cancer Network, and the American College of Radiology
- The one notable outlier is the US Preventive Service Task Force (USPSTF), whose guidance tends to inform insurance coverage decisions
- The USPSTF currently recommends mammography only every other year for average risk women aged 40-74, with NO explicit recommendation for high-risk women
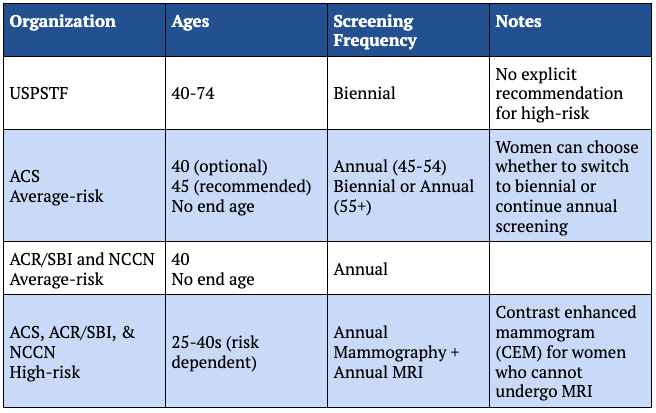
Figure 3. Summary of screening recommendations by major cancer and radiology groups.
These are population-level guidelines
- They’re created by looking at large studies and evaluating the optimal strategy for maximizing cancer detection while minimizing false positives across millions of women
- And of course, they take into account the societal cost of screening
A framework for personalizing screening [8:45]
When you move from populations to actual people, personalization matters
- Questions to ask when we think about how to personalize screening (for any cancer)
- 1 – What is my baseline risk?
- 2 – Then, given that risk: How much false positive burden am I willing to tolerate in exchange for potentially earlier detection?
- 3 – Which screening plan (both modality and frequency) best match both of these objectives?
This is not about trying to outsmart the guidelines. It’s about deciding whether the default plan actually fits you
- For some women, the default plan will fit, but for others, it will fall short
- The aim is NOT to get as much imaging as possible
The aim is to land on a strategy most likely to help someone with your particular risk profile
Assessing baseline breast cancer risk: genetics, family history, breast density, lifestyle factors, and the role of risk calculators in personalized screening [9:30]
- While most people immediately think of BRCA-level risk when they think about breast cancer, most women who develop breast cancer do NOT have 1 dramatic obvious risk factor
- It is far more common to have several smaller risk factors that together add up to a higher risk
- So, we are not just looking for the rare woman with the obvious red flag
- We want to identify the women whose overall risk is meaningfully above average
However, risk assessment is only useful if it happens early enough to change the plan
“You do not want to find out at age 42 that you should have been the patient who started MRI years earlier.”‒ Peter Attia
- That is why some groups recommend formal risk assessment by age 25
- Not because everyone needs imaging at 25
- But because by then you want to know whether or not you are truly average risk or not
- Peter thinks this is exactly right: a risk assessment should be done in your mid-20s
What are the risk factors we need to consider?
- The most basic are the ones we don’t usually think of as risk factors: sex, and age
1 – Breast cancer is overwhelmingly more common in women: 1 in 8 versus 1 in about 750 for men
- Keep in mind, men can develop this as well
2 – There’s age: which is one of the strongest breast cancer risk factors overall
- The median age at diagnosis is around 62
- And the vast majority of breast cancers are diagnosed after age 40
- While age alone is an imperfect guide, it is important to keep in mind that risk accumulates over time
3 – But once you get past these 2 obvious risk factors, the most obvious high impact category is genetics
- Mutations in genes like BRCA1 and BRCA2 are the most recognized inherited breast cancer risk factors
- And for good reason, they can substantially increase risk and often shift that risk earlier in life
- But these mutations are actually much rarer than people tend to think
- In the general population, only about 1 in 400 people carry a pathogenic mutation in BRCA1 or BRCA2
- Though prevalence is higher in some groups, including people of Ashkenazi, Jewish ancestry
- There are also other important genes, but the broader point is that inherited mutations matter a great deal for screening, even if they account for a minority of breast cancer cases
4 – And genetics ties directly into the next vector: family history
- Peter separates these because family histories capture more than just the known single gene mutations
“Family history is a proxy for high impact mutations like the BRCA mutations, but it also reflects the cumulative effect of lower penetrant genetic variants, shared environmental exposures, and other inherited factors that no single genetic test currently covers.”‒ Peter Attia
- Having multiple first-degree or second-degree relatives, parents, siblings, grandparents, aunts with breast cancer can substantially increase your risk
But keep in mind that lack of family history does not automatically equate to low risk
- Some families are small
- Some relatives may have died young of other causes
- And importantly, some mutations that increase breast cancer risk can show up in the family as other cancers like prostate or pancreatic cancer, rather than an obvious pattern of breast cancer
So, family history matters, but it should be interpreted thoughtfully, and the absence of a family history of breast cancer does not guarantee that you are of average risk
In addition, ancestry related differences can influence both risk and tumor biology
- In the US, for example, Black women are more likely to be diagnosed younger and with more aggressive subtypes
- Which has implications for how early and how aggressively screening should be considered
5 – Another important category is prior chest radiation
- The classic example is radiation treatment for Hodgkin’s lymphoma in adolescence or early adulthood
- Cumulative high dose exposure, particularly around the time when breast tissue is still developing, carries the greatest risk
- Now to be clear, this does not mean you should avoid a diagnostic x-ray if your doctor recommends one
⇒ A single chest x-ray or CT delivers a tiny fraction of the dose used in cancer treatments and the evidence that the occasional routine chest imaging study meaningfully increases breast cancer risk is very weak at best
6 – Breast density is important for 2 separate reasons
- First, dense breasts are associated with a somewhat higher baseline risk of breast cancer
- But just as importantly, dense tissue makes mammograms harder to interpret because both dense tissue and tumors appear white on the image
So, breast density is not just a biological risk factor, it’s also one of the main reasons our most common screening test becomes less effective
- And this is where things get a little tricky
- You usually cannot actually know your breast density until you’ve had an imaging study
- Which for most otherwise average risk women does not happen until screening begins at around age 40
- This creates a bit of a catch-22
- Density matters for screening decisions, but you often do not learn until it’s potentially too late
⇒ There’s a partial workaround though, breast density is fairly heritable, roughly 60-70%
- So, if your mother or grandmother was told she had dense breasts, that’s worth knowing
- It is just not something most women tend to think about
Peter points out, “Density matters enough that the FDA now requires imaging centers to notify women of it.”
- That is typically reported with the BI-RADS density category
- A and B are considered non-dense
- While C and D are considered dense
⇒ While density declines with age, about 50% of screening age women have dense breast tissue
7 – Then, there are the reproductive and hormonal factors, which tend to be more cumulative in nature
In general, the factors that point toward higher risk include earlier onset of menstruation, later menopause, never having had a full-term pregnancy, or having a first pregnancy after age 40 and not breastfeeding
- Individually, none of these risk factors typically change the screening plan on its own, but they do contribute slightly to overall risk, especially when several are present together
- The same is true of modifiable risk factors
8 – Modifiable risk factors: alcohol use, obesity, poor metabolic healthy, and physical activity
- You don’t need to change your screening protocol based on these alone, but they can shift risk and are factors you should actually do something about
Peter’s takeaway
- The big picture here is that risk is usually NOT 1 thing–it is the sum of multiple inputs
- Some large, some small, that together determine whether someone is truly average risk, somewhat above or below average, or clearly high risk
- And because no one is going to accurately estimate all of that in their head, this is where formal tools can help
Calculators used to estimate breast cancer risk
- Calculators like Tyrer-Cuzick combine family history, personal risk factors, and breast density to estimate 10-year and lifetime risk
- These models are not perfect, but they are much better than guessing
- And they help identify women whose risk is high enough to justify earlier or more intensive screening
Most screening guidelines classify lifetime risk above 20% as high risk, though factors such as ancestry may shift that threshold
- You can find these calculators online, and it’s a good idea to complete one so you can get a more concrete understanding of where your risk falls
Peter emphasizes, “If you take anything away from this, know your risk and know it early enough that you still have time to act on it.”
- But risk alone doesn’t tell you what to do.
Balancing cancer detection and false positives: how breast cancer risk influences screening intensity and imaging choices [17:45]
The next question is, given that risk, how aggressively do you want to be screening?
- Because every time you push screening towards higher sensitivity, that is finding more cancers
- You also accept more downside, more false positives, and more follow-up testing
- Not to mention the anxiety that can come with those
- In a perfect world, screening would find every meaningful cancer early and spare everyone the downside of a false alarm
- But in the real world, the balance is never that straightforward
⇒ In the US, about 10% of screening mammographies lead to a callback for additional testing, but only about 5% of those callbacks end in a cancer diagnosis
- In other words, for every 1,000 women who undergo a screening mammogram, about 100 will be called back because something looked abnormal
- But about 95 of those 100 will NOT actually have cancer, and those numbers add up over time
⇒ More than half the women screened annually for 10 years will experience at least 1 false positive result
Harms from screening
- The most common harms from breast cancer screening are not major physical injuries from the test itself, but the anxiety and uncertainty that comes from a return visit for more imaging
- When a callback leads to an earlier cancer diagnosis, it’s obviously worthwhile
- But when most callbacks do not end in cancer, we need to think carefully about what screening strategy makes sense for each individual woman
How should a woman think about that trade-off?
- The higher your baseline risk, the easier it is to justify accepting more false positives in exchange for finding more cancer earlier
- If you’re very high risk, say you carry a BRCA mutation or have a combination of factors that pushes your lifetime risk well above average, then a more aggressive strategy is easy to defend
- If you’re truly average risk or even lower than average risk, the decision is based largely on preference
- That does not necessarily mean less screening
- It means being thoughtful about how much extra testing you’re willing to accept for what may be smaller incremental benefits
Peter emphasizes, “That’s really the key here. More screening is not automatically better screening.”
- The right question is NOT: How much imaging can I get?
- But which strategy is most likely to help someone with my risk profile
- And am I comfortable with the trade-offs that come with that
- There’s no universal answer to that question–it depends on the person
- But once you know your baseline risk and you have a sense of your tolerance for false positives, you’re ready for the next piece
Which screening tools actually exist and how should you think about choosing between them?
- When we talk about breast cancer screening, it’s often treated as if breast imaging were just one thing, but it’s not
“Breast imaging is a toolkit consisting of different varieties of mammography, MRI, and ultrasound.”‒ Peter Attia
- Some of these are best for routine screening while others are more appropriate for follow-up on an abnormal finding or as a supplemental option in higher risk women
- Peter will go through each of these here, summarized in the detailed comparison table at the end of these notes
Mammography as the foundation of breast cancer screening: detecting ductal carcinoma in situ (DCIS) and the advantages of 3D versus 2D mammography [21:00]
- The foundation of screening is mammography
- Mammograms use low dose x-rays to look for breast cancer, and for most average risk women, they remain the starting point
- One important strength of mammography is that it is particularly good at detecting calcifications such as those seen in ductal carcinoma in situ (DCIS)
DCIS is sometimes called stage zero breast cancer
- The abnormal cells are still confined to the ducts rather than invading surrounding tissue
⇒ If left untreated, estimates suggest that somewhere between 25-60% of DCIS cases may eventually become invasive cancer
- This is a wide range that reflects how much we still don’t know about the natural history of DCIS
But that uncertainty is precisely why early detection matters and mammography is well suited for finding it
That said, not all mammograms are the same
- In 2000, the FDA approved the first full field digital mammography system, and this is what most of us are thinking of when we hear mammogram
- Standard digital mammography–sometimes called 2D mammography–is the technology that many research studies have historically used
- Most recently in 2011, digital breast tomosynthesis (DBT), commonly referred to as 3D mammography was rolled out
- DBT takes multiple images from different angles to create a more layered view of the breast
- This results in better cancer detection with lower recall rates, particularly for women with dense breasts
- Not every imaging center offers DBT, however, and sometimes there is still an added cost
DBT is the version of mammography Peter would prioritize–especially for women with dense breasts
MRI for high-risk women: the benefits of supplemental screening, abbreviated MRI, and the emerging role of contrast-enhanced mammography [23:00]
- Mammography is the right foundation for virtually everyone, but for women at higher risk, mammography alone may not be sensitive enough
- This is where MRI comes in
While not a complete replacement for mammography, MRI is an important supplemental option
- MRI uses magnetic fields and intravenous gadolinium-based contrast to detect abnormal blood flow or tissue behavior that mammography can miss, making it the most sensitive screening tool available
- It is better for detecting very small invasive tumors and atypical cancers than any other imaging modality
- But it’s not perfect for everything: mammography still does a better job with certain calcifications
So MRI is generally used in addition to, but NOT instead of mammography
The downsides of MRI
- The downsides are cost, access, and the use of IV contrast
- Along with a higher callback burden because of the higher sensitivity
Peter makes the point, “But if your goal is maximum cancer detection, MRI’s sensitivity tends to outweigh these downsides.”
- The full breast MRI is what most very high-risk women are recommended for initial screening and may also be used for diagnostics after an abnormal test
More recently, many patients are opting for the abbreviated breast MRI
- In Peter’s mind, abbreviated breast MRI is the most underutilized tool we have
- Based on current diagnostic accuracy data, the abbreviated protocol preserves nearly all of the sensitivity of the full exam, but takes only 10-15 minutes
- Compared to 30-60 minutes for the full [MRI] exam
- That makes it cheaper, faster, and more scalable while still providing dramatically better cancer detection than mammography alone
⇒ For women with extremely dense breasts, adding MRI after a negative mammogram, cut the rate of interval cancers, meaning cancers found between screens in half from 5 per 1000 to 2.5 per 1000 with mammography alone [the DENSE trial]
“For women who are high risk, have dense breasts or simply want a more sensitive complement to mammography, MRI is the strongest option we have.”‒ Peter Attia
- In many screening settings, an abbreviated MRI is likely sufficient
- While the full protocol may be more useful for diagnostic workup and select edge cases
If MRI is not feasible, the next best modality is contrast-enhanced mammography (CEM)
- CEM is a newer modality introduced in 2011 that is basically mammography plus intravenous iodine-based contrast
It gives more functional information than a standard mammogram and can be a very reasonable alternative when MRI is unavailable or contraindicated
- This technology isn’t yet widely available, but Peter thinks it will become more popular in the future
The role of ultrasound: supplemental cancer detection, diagnostic evaluation, and limitations compared with mammography and MRI [26:00]
- Ultrasound uses sound waves rather than radiation or magnetic fields to create images of breast tissue
- As with the other imaging modalities, ultrasound comes in different flavors
- Handheld where a technician or radiologist moves the probe manually
- And automated where the machine acquires images more systematically
- Both are more operator-dependent than mammography or MRI
- And both carry a higher false positive burden than you would see in those modalities
Ultrasound can be useful as a supplemental imaging modality, but its value is highly dependent on 2 things
- 1 – Who performs the ultrasound
- 2 – What baseline imaging you are adding it to
Benefits of ultrasound screening
- In one study, adding physician-performed handheld ultrasound to a standard 2D mammography increased the rate of cancer detection by 4.2 per 1000 women screened
- A second study paired technician performed ultrasound with DBT, the more sensitive mammogram, and the detection boost was much smaller, only about 1.1 per 1000
Peter points out, “When the base imaging is better or the technician is less experienced, the incremental benefit of ultrasound shrinks.”
- [Your base imaging should be DBT and with better imaging, ultrasound doesn’t add as much benefit for detecting cancer]
- [If the technician is less experienced, again ultrasound doesn’t add as much benefit
- Because ultrasound is a supplemental imaging modality added on to the mammogram]
That doesn’t mean ultrasound is not worth doing, but it does mean its benefits are more variable than what we see when adding MRI to mammography
Where does ultrasound best fit into practice?
- Because handheld ultrasounds allow for real-time visualization, they’re an excellent option for getting more clarity on something suspicious seen on other imaging or guiding biopsies
- And while ultrasound can boost cancer detection over mammography alone, it’s not going to do it to the same extent seen with adding MRI
Ultimately, ultrasound is a viable tool, but for average risk women, it is not a substitute for mammography, and for high-risk women, it’s not a substitute for MRI
Choosing the right breast cancer screening strategy: imaging modality selection, screening hierarchies, and the importance of imaging center quality [28:00]
How do we actually pull all of this together in a way that is useful?
- At a practical level, the hierarchy looks like this
- The foundation for all women is mammography–ideally, digital breast tomosynthesis (DBT)
- If your risk is elevated or if dense breast tissue is likely to reduce the sensitivity of mammography, MRI is the most effective supplemental tool
- If MRI is not feasible due to cost, access or contraindication, contrast-enhanced mammography is the next best option
- Ultrasound can add incremental detection, but its benefit is more variable and highly dependent on operator’s skill and on the baseline imaging that it’s paired with
The key point is that these tools are NOT interchangeable
- They have a clear hierarchy in terms of sensitivity and consistency
- And your goal is to choose the combination that best matches your risk
Regardless of the screening tool you decide on, keep in mind that where you get screened matters
- Not every imaging center offers every modality and not every center has the same level of experience with the tests it offers
“Simply having imaging done is not the same thing as having high quality imaging done.”‒ Peter Attia
Hallmarks of quality imaging
- For mammography, positioning and complete tissue capture matter
- MRI and CEM [contrast enhanced mammogram] are more standardized, but they still depend on good protocol execution, contrast timing, and experienced interpretation
- For the reasons Peter discussed a moment ago, ultrasound is the most operator-dependent modality
- A routine mammogram can usually be done well in many places, but the quality of imaging and interpretation still varies
- High volume centers and dedicated breast imaging centers tend to have more experience, better protocols, and more consistent interpretation
Peter’s advice, “If you are pursuing more advanced imaging, such as MRI or contrast enhanced-mammography or even ultrasound in dense breast tissue, you should strongly consider going to a center that performs these studies frequently and has specialized expertise.”
- The difference is not trivial, and in some cases, it can directly affect whether a cancer is detected or not
Bottom line here is that each imaging modality has strengths and weaknesses, and which one or which option you choose is a personal choice based on your risk, your preferences, and your access
How often should you screen for breast cancer? [30:15]
Once you think about imaging in that way, the next question becomes: How often should you screen?
- The USPSTF recommends biennial mammography for average risk women aged 40 to 74
- Most other groups recommend annual mammography starting around the age of 40, or a hybrid approach with annual screening from 45 to 54 and biennial screening thereafter
- Though Peter has never really understood that given that risk is always going up with age
Peter adds, “It’s worth acknowledging upfront that no randomized control trial has ever directly compared annual versus biennial screening with mortality as its primary endpoint.”
- Every interval recommendation we have is based on modeling studies and observational data
- That does not mean we’re flying blind
- But it does mean we are working with a slightly different kind of evidence than we have for, say, the question of whether screening reduces mortality at all
The most important modeling data come from the Cancer Intervention and Surveillance Modeling Network (CISNET)
- This is a consortium of independent modeling groups funded by the National Cancer Institute
- CISNET has been commissioned 3 times to run simulations for the USPSTF, and the task force has leaned heavily on these models to justify biennial mammography recommendations
- Interestingly, other cancer and radiology groups have looked at the same CISNET data to conclude that annual screening is better
So, which is it?
- The answer depends on your question
- If the question is: How to maximize efficiency across an entire population, balancing cost, false positives, and resource utilization?
- Biennial screening is a defensible answer
- But if the question is: What gives an individual woman the best chance of avoiding death from breast cancer?
- The answer is different
- And that distinction is critical for everything that Peter about to say
The argument for biennial mammography
- This traces back to the original 2009 CISNET analysis, which found that biennial screening retained about 81% of the mortality benefit of annual screening with roughly half as many false positives
- This was done using data from film-based mammography, the technology that came before digital mammography and certainly before DBT was introduced
- The conclusion from this modeling study was NOT that biennial mammography was best for mortality, but that it offered the best trade-off between benefit and resource use at a population level
- In 2024, CISNET published its most comprehensive analysis using multiple models and imaging strategies, including both two-dimensional digital mammography and DBT
A secondary analysisof those results showed, in essence, that annual screening is better for saving lives
⇒ When compared to no screening, annual screening of women aged 40 to 79 produced a 42% mortality reduction, while biennial screening produced only a 30% mortality reduction
- In absolute numbers, this corresponded to 230 life years gained per 1000 women for annual screening versus 165 for biennial
What about the false positives generated from annual screening?
- The cumulative number for false positives is higher for annual screening
- As we would expect, given that we’re performing twice as many tests
- However, the rate of false positives and benign biopsies per exam is actually lowest with annual screening
- Likely because the radiologist has a more recent image to compare to, making it easier to distinguish cancerous changes from normal variation
- Peter thinks this is a very important statistic that gets overlooked
Peter’s takeaway
- The bottom line is that the case for biennial screening rests on population level efficiency, not on maximizing the benefits for any individual woman
- If the question is what gives you the best chance of not dying from breast cancer, CISNET’s own data answers it clearly, screen annually
The observational datatell a similar story
- Among women aged 40 to 84 who developed breast cancer, those screening annually had far fewer interval cancers
- 11% versus 38% for biennial screeners
- And were more likely to have an early stage diagnosis: 76% stage I with annual screening versus 56% with biennial
Taken together the modeling and observational data, the conclusion is straightforward, if your goal is to maximize your chances of avoiding death from breast cancer as an individual, annual mammography is the better strategy
- But all of these studies have focused entirely on mammography
What about when to add in other imaging modalities such as MRI?
- The most common approach in clinical practice is to alternate the 2 tests every 6 months
- Say mammography in January and MRI in July, rather than stacking them at the same time
- The logic is kind of intuitive: by spacing them out, you’re effectively creating a 6-month screening interval instead of a 12-month one
- Which in theory gives the fastest growing cancers less time to develop between the screens
- But the evidence here is thinner than you might expect, in large part because these studies are genuinely hard to do well
- When 2 tests are given at 2 different times, it becomes very difficult to fairly credit a cancer detection to one test versus the other
- Which makes comparing the 2 scheduling approaches unreliable
- One small study found that the combined sensitivity of MRI plus mammography was higher than either test alone, while another found no significant difference between stacking and alternating
- Neither is definitive
- For ultrasound plus mammography, the timing question has essentially never been studied directly
- All major ultrasound trials performed both tests simultaneously and annually
- Any rationale for staggering ultrasound is purely extrapolated from the already limited MRI literature
The bottom line on multi-modality scheduling is rather unsatisfying
- We do not yet have compelling evidence to favor one schedule over another
- Peter might lean towards the alternating schedule for high-risk women who are more likely to develop rapidly growing cancers
- But until better prospective data exists, the scheduling decision is really more about logistics and personal preference
The practical takeaway
- All women should screen annually with mammography
- If you are high risk and you are getting multiple imaging modalities, alternating them every 6 months is reasonable
- But the evidence is not strong enough to insist on that schedule
- Right now, the bigger issue is not whether the tests are staggered, it’s whether both tests are getting done consistently each year
At what age should you start screening? [37:30]
- At this point, we know we should do a risk assessment in our mid-20s
- And we know how often to screen and which imaging modalities make sense
The next question is, when should we actually start screening?
- Peter saved this for last because this is the area where we have the least concrete data beyond the whole scheduling thing
- The intuitive assumption is that if screening saves lives, then starting earlier should save more of them
But whether earlier screening actually helps depends on many factors, and the answer is more nuanced than you might expect
First, the risk for developing breast cancer before age 40 is genuinely low
- Only about 5% of breast cancer diagnoses occur in women under 40
- The cumulative risk through age 90 is about 13%
- Which is where that familiar 1 in 8 statistic comes from
- But the cumulative risk through age 40 is less than 1%
Now, the obvious next question, how do we know incidence is actually low if we’re not routinely screening women under 40?
- Maybe we are just not finding cancers that are there
- But these data come from cancer registries, which capture all diagnosed cancers, including cancers found symptomatically and cancers caught in women who began screening earlier because of elevated risk
- On top of that, the age incidence curves rise smoothly and continuously through the 30s and 40s
- The figure below shows risk of breast cancer over a woman’s lifespan
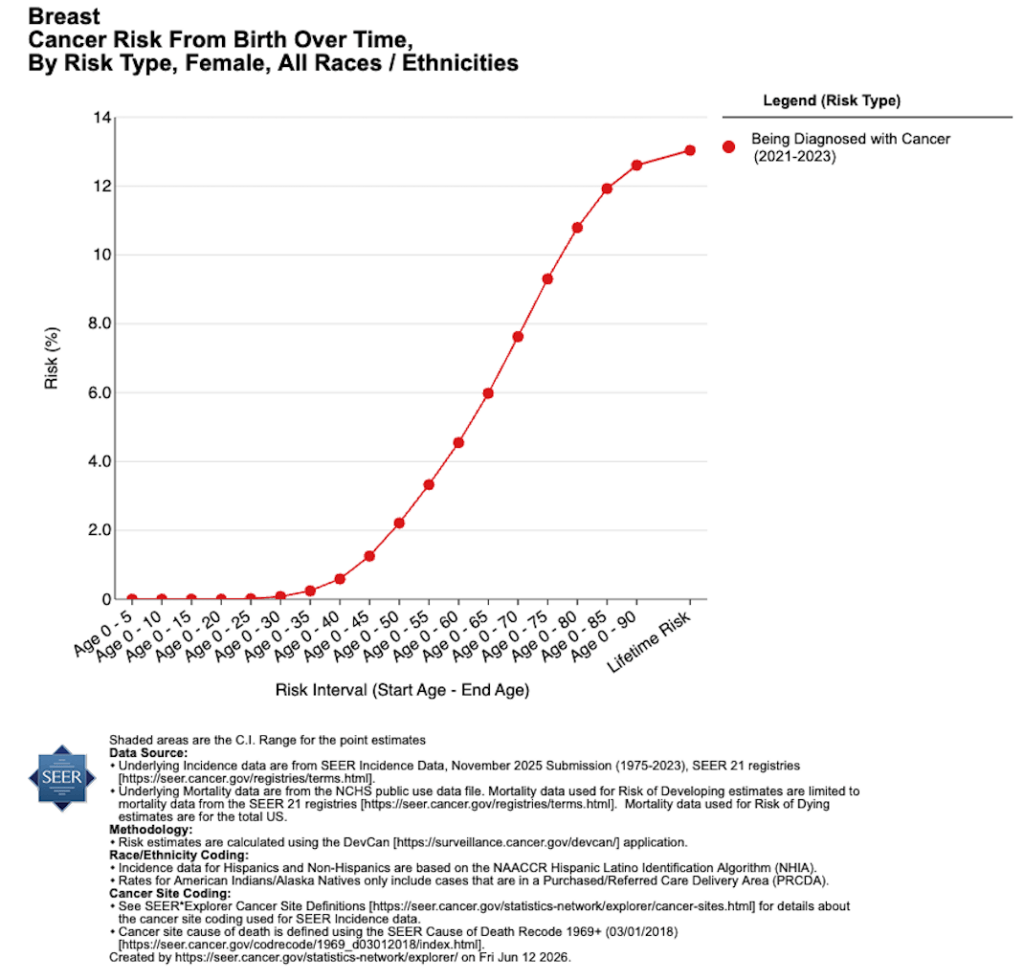
Figure 4. Cumulative risk for breast cancer by age. Image credit: National Cancer Institute SEER
Notice that there is NO sharp spike at age 40
- Which is what you would expect to see if screening were suddenly uncovering a large hidden backlog of disease
- So, the low incidence under 40s appears to be real, not an artifact of under detection
But low risk does NOT mean no risk, so could there still be a case for screening before 40?
- This is where we run into the limits of evidence
- We have no randomized trials and no mortality data on screening average risk women under 40
- The best study we have looked at
- About 6 million mammograms from facilities across the US
- About 12% of these mammograms were from women under 40
- And the researchers compared cancer detection rates across age groups broken down by whether a woman had at least 1 risk factor [1 of the 3 risk factors listed below]
⇒ Risk factors were defined as: a personal history of breast cancer, a family history in a first degree relative, or dense breasts
- Among women aged 35-9 with at least 1 risk factor, the cancer detection rate was 2.1 per 1,000 women screened
- For average risk, women in the same group with no family history, no personal history, and non-dense breasts, the rate was just 0.59 per 1,000
- This is about a 3.5-fold difference driven by risk factors, not age alone
- And here’s where the comparison gets especially interesting, for average risk women age 40-44, the detection rate was only 0.71 per 1,000
In other words, women in their late 30s with risk factors were being diagnosed with cancer at roughly 3x the rate of average risk women who were screening in their 40s
Peter emphasizes, “Those risk factors are not just nudging the needle. They are effectively shifting a woman’s screening profile forward by a decade.”
- Once you get to women 45 and older, incidence rises enough that detection rates exceed what we would see in women under 40, regardless of risk
- But below that threshold, risk factors may matter more than age
“This brings us back to the point I’ve made throughout this discussion, knowing your baseline risk is what makes the difference.”‒ Peter Attia
Peter’s takeaway
- The age 40 cutoff for screening makes sense on average, but for women with 1 or more of these 3 risk factors we’ve just discussed, earlier screening may be the right call
- And the women who are diagnosed with breast cancer in their 20s and 30s are NOT a random cross-section of the population, they are disproportionately women who could have been identified as above average risk earlier on
Breast cancer in younger women: aggressive tumor biology, BRCA-related risk, breast density, and individualized decisions about when to begin screening [41:45]
On top of this, breast cancer doesn’t look the same in younger women as it does in older women
- Younger women are much more likely to develop aggressive subtypes
⇒ About 20% of breast cancer in women under 40 are the so-called triple-negative, the most aggressive form compared with roughly 6-12% in women over 40, and these tumors grow fast
- Triple-negative cancers can double in size in under 4 months, which means even annual screening may not catch them in time
- On the other end of the spectrum, the slower growing cancers that screening is best at detecting, the ones with doubling times closer to a year, make up only about a third of cases in women under 40 compared to well over a half in older women
For high-risk women, this biology has direct implications for which screening tool to use
- Mammography alone may not be enough
- Consider how risk from a BRCA1 mutation plays out over a lifetime
- It’s not spread evenly
- It’s heavily front loaded
- A woman in her late 20s carrying a BRCA1 mutation has a breast cancer risk roughly 100x that of a non-carrier
- By her 30s, it’s about 44x
- And by her 60s, it drops to about 3x
In other words, these mutations don’t just increase risk, they shift the entire risk curve earlier
Peter makes the point, “Because the cancers that develop in these younger, high-risk women tend to be fast growing and harder to see in mammography, MRIis the more appropriate screening tool for this group.”
There is one more practical consideration worth mentioning–breast density
- 1 of the 3 risk factors in the study Peter just discussed was breast density
- And as he mentioned earlier, you cannot know your breast density without imaging, at least definitively
⇒ About half of women have dense breasts and density is higher in younger women than older women
“There’s a reasonable argument for getting a single baseline mammogram in your 30s, not primarily to find cancer, but to establish whether you have dense breasts.”‒ Peter Attia
- If you do have dense breasts, that changes your risk profile and may change your screening strategy
- To be clear, this is LESS about cancer detection and MORE about risk stratification
- And while there is no direct evidence supporting this approach, it’s something that Peter thinks is worth considering
So, when should you start screening?
- As with everything else we’ve talked about, it depends on your risk
- If you are truly average risk, beginning annual mammography at 40 is well-supported
- Though you may want to consider getting a baseline mammogram in your 30s at a minimum to establish your breast density
- If you are above average risk, there is a small amount of evidence that mammography in your 30s can be worthwhile
- And if you’re clearly high risk: a known BRCA carrier, a strong family history or prior chest radiation
- The conversation is different entirely and more aggressive screening protocol should be started in your 20s or early 30s
Inflammatory breast cancer, the limitations of screening mammography for symptomatic disease, and the importance of promptly evaluating new breast symptoms in both women and men [44:45]
- Everything we have discussed so far is about routine screening, finding cancer before it causes symptoms
- But there’s one type of breast cancer that does not follow those rules and Peter wants to make sure we address it before we wrap up
Inflammatory breast cancer
- Inflammatory breast cancer is a rare type of cancer, roughly 1-5% of all breast cancers, but it is aggressive and it does not present the way most people expect breast cancer to present
- There is often no discrete lump
- Instead, what you may notice is rapid swelling or heaviness of the breast, redness or rash, warmth, or changes in skin texture or thickness
- Because these symptoms can look like skin irritation or something else relatively benign, diagnosis is frequently delayed
And this is the key point: normal screening mammography does not rule-out inflammatory breast disease
- These cancers may NOT be visible on mammography, so a diagnostic workup is necessary
Peter emphasizes, “This is an important reminder that screening tests are designed for women without symptoms.”
“If you notice something new, a lump, skin changes, nipple discharge, pain that does not resolve, do NOT wait for your next scheduled screening.”‒ Peter Attia
A recent normal screen does NOT guarantee everything is fine
- Go and get evaluated in person by your doctor
- And this applies to men too
A word about men
- Peter has focused this discussion on women because the vast majority of breast cancers occur in women, but men do develop breast cancer
- Because we do not routinely screen men, symptoms are typically the only path to diagnosis
A new symptom in a man should NOT be dismissed. It should be evaluated just as it would be in a woman.
From risk assessment to personalized screening: a practical framework for reducing breast cancer mortality through earlier and more effective detection [46:30]
Where does all of this leave us?
- We started this episode with a question: If screening works so well, why are 42,000 women still dying from breast cancer every year?
- Part of the answer is biology
- Some cancers are aggressive enough that they will evade even the best screening
- But the far larger part and the one that we can actually do something about right now is that we are not screening intelligently enough
- A quarter of eligible women are not up-to-date on basic mammography
- A quarter of eligible women are not up-to-date on basic mammography
- The vast majority of women who qualify for MRI are not getting it
- And most women have never had a formal risk assessment
“The science here is not the bottleneck. The tools exist. The evidence is strong. What is missing is the bridge between what we know and what women are actually doing.”‒ Peter Attia
To be clear, this is NOT an individual failure
- Access to MRI is limited in many areas
- Insurance coverage is often tied to the USPSTF recommendations–which do not fully address high risk populations
- Imaging quality varies across centers
All of these system level factors contribute to underscreening and suboptimal screening, but there is still a great deal that is within your control
If you take nothing else from this episode, let it be this
- 1 – Complete a risk assessment using a validated risk calculator so you have a quantitative sense of your baseline risk
- 2 – Find out your breast density from prior imaging or plan to establish it when you begin screening
- 3 – Choose a cancer screening strategy
- With both a modality and frequency that matches your level of risk and your tolerance for false positives.
- 4 – Execute that plan consistently over time
Peter makes the point, “None of these steps are complicated, but taken together, they are what separates passive screening from intentional personalized screening.”
- With the current technology, we cannot reduce breast cancer deaths to zero, but far too many lives are still being lost because we are applying the right tools too late, too inconsistently, or to the wrong people
- At least at the individual level, this problem is more solvable than most people realize
- If risk is assessed, the right screening strategy is chosen ,and the screening is actually carried out
****
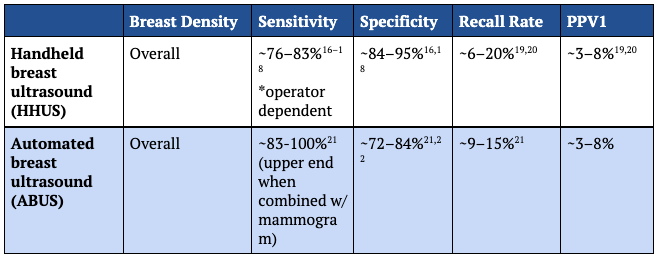
CHARTS: comparison of screening tools used to detect breast cancer
Positive Predictive Value 1 (PPV1) is the percentage of abnormal screening tests that result in a cancer diagnosis within 12 months. (In other words, how likely is it that a woman who gets recalled has cancer.)
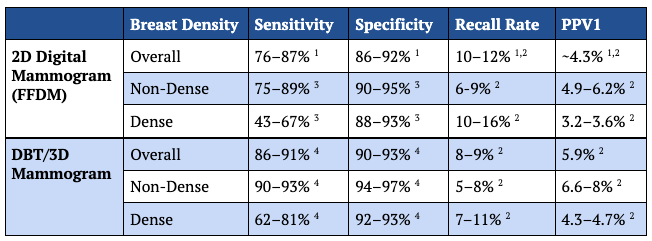
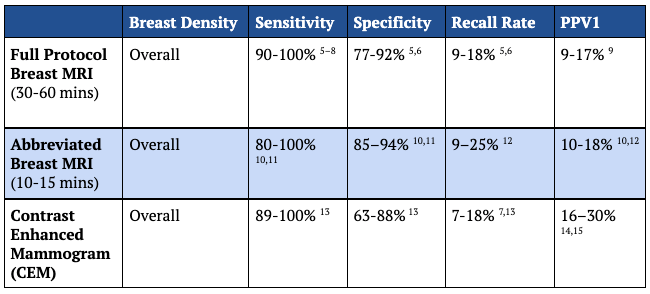
^ Variability in several categories is due to study populations; MRI and CEM are typically evaluated in higher-risk populations and/or for patients recalled after abnormal digital mammography. High recall rate and PPV1 is generally due to use as a secondary imaging modality in at-risk individuals.
1. Lehman CD, Arao RF, Sprague BL, et al. National performance benchmarks for modern screening digital mammography: Update from the Breast Cancer Surveillance Consortium. Radiology. 2017;283(1):49-58. doi:10.1148/radiol.2016161174
2. Conant EF, Talley MM, Parghi CR, et al. Mammographic screening in routine practice: Multisite study of digital breast tomosynthesis and digital mammography screenings. Radiology. 2023;307(3):e221571. doi:10.1148/radiol.221571
3. Payne NR, Hickman SE, Black R, Priest AN, Hudson S, Gilbert FJ. Breast density effect on the sensitivity of digital screening mammography in a UK cohort. Eur Radiol. 2025;35(1):177-187. doi:10.1007/s00330-024-10951-w
4. Kniss AS, Mercaldo S, Bahl M. Impact of breast density on screening performance metrics: An analysis of 301,400 screening digital breast tomosynthesis (DBT) examinations. Acad Radiol. 2026;0(0). doi:10.1016/j.acra.2025.12.042
5. Raikhlin A, Curpen B, Warner E, Betel C, Wright B, Jong R. Breast MRI as an adjunct to mammography for breast cancer screening in high-risk patients: retrospective review. AJR Am J Roentgenol. 2015;204(4):889-897. doi:10.2214/AJR.13.12264
6. Warner E. Screening BRCA1 and BRCA2 mutation carriers for breast cancer. Cancers (Basel). 2018;10(12):477. doi:10.3390/cancers10120477
7. Lawson MB, Partridge SC, Hippe DS, et al. Comparative performance of Contrast-enhanced mammography, abbreviated breast MRI, and standard breast MRI for breast cancer screening. Radiology. 2023;308(2):e230576. doi:10.1148/radiol.230576
8. Melnikow J, Fenton JJ, Whitlock EP, et al. Supplemental screening for breast cancer in women with dense breasts: A systematic review for the U.s. preventive services task force. Ann Intern Med. 2016;164(4):268-278. doi:10.7326/M15-1789
9. Lo G, Scaranelo AM, Aboras H, et al. Evaluation of the utility of screening mammography for high-risk women undergoing screening breast MR imaging. Radiology. 2017;285(1):36-43. doi:10.1148/radiol.2017161103
10. Kwon MR, Choi JS, Won H, et al. Breast cancer screening with abbreviated breast MRI: 3-year outcome analysis. Radiology. 2021;299(1):73-83. doi:10.1148/radiol.2021202927
11. Grimm LJ, Mango VL, Harvey JA, Plecha DM, Conant EF. Implementation of Abbreviated Breast MRI for Screening: AJR Expert Panel Narrative Review. American Journal of Roentgenology. 2022;218(2):202-212. doi:10.2214/AJR.21.26349
12. Gilbert FJ, Payne NR, Allajbeu I, et al. Comparison of supplemental breast cancer imaging techniques-interim results from the BRAID randomised controlled trial. Lancet. 2025;405(10493):1935-1944. doi:10.1016/S0140-6736(25)00582-3
13. Jochelson MS, Lobbes MBI. Contrast-enhanced mammography: State of the art. Radiology. 2021;299(1):36-48. doi:10.1148/radiol.2021201948
14. Sung JS, Lebron L, Keating D, et al. Performance of dual-energy contrast-enhanced digital mammography for screening women at increased risk of breast cancer. Radiology. 2019;293(1):81-88. doi:10.1148/radiol.2019182660
15. Patel BK, Carnahan MB, Northfelt D, et al. Prospective study of supplemental screening with contrast-enhanced mammography in women with elevated risk of breast cancer: Results of the prevalence round. J Clin Oncol. 2024;42(32):3826-3836. doi:10.1200/JCO.22.02819
16. Rehman H, Ahmad I, Rashid S, Mukhtar M, Khan AA, Khaliq H. Comparison of diagnostic accuracy of ultrasound and mammography in detecting breast cancer in radiographically dense breasts. Cureus. 2025;17(9):e92637. doi:10.7759/cureus.92637
17. Chen HL, Zhou JQ, Chen Q, Deng YC. Comparison of the sensitivity of mammography, ultrasound, magnetic resonance imaging and combinations of these imaging modalities for the detection of small (≤2 cm) breast cancer. Medicine (Baltimore). 2021;100(26):e26531. doi:10.1097/MD.0000000000026531
18. Sood R, Rositch AF, Shakoor D, et al. Ultrasound for breast cancer detection globally: A systematic review and meta-analysis. J Glob Oncol. 2019;5(5):1-17. doi:10.1200/JGO.19.00127
19. Brem RF, Lenihan MJ, Lieberman J, Torrente J. Screening breast ultrasound: past, present, and future. AJR Am J Roentgenol. 2015;204(2):234-240. doi:10.2214/AJR.13.12072
20. Berg WA, Blume JD, Cormack JB, et al. Combined screening with ultrasound and mammography vs mammography alone in women at elevated risk of breast cancer. JAMA. 2008;299(18):2151-2163. doi:10.1001/jama.299.18.2151
21. Choi WJ, Kim SH, Shin HJ, et al. Automated breast US as the primary screening test for breast cancer among East Asian women aged 40-49 years: a multicenter prospective study. Eur Radiol. 2021;31(10):7771-7782. doi:10.1007/s00330-021-07864-3
22. Gatta G, Cappabianca S, La Forgia D, et al. Second-generation 3D automated breast ultrasonography (prone ABUS) for dense breast cancer screening integrated to mammography: Effectiveness, performance and detection rates. J Pers Med. 2021;11(9):875. doi:10.3390/jpm11090875
Selected Links / Related Material
USPSTF breast cancer screening guidelines: Breast Cancer Screening | U.S. Preventive Services Task Force (April 30, 2025) | [2:15]
American Cancer Society breast cancer screening guidelines: Breast Cancer Screening Guidelines | American Cancer Society (October 20, 2015) | [7:45]
National Comprehensive Cancer Network breast cancer screening guidelines: NCCN Guidelines | National Comprehensive Cancer Network® (2026) | [7:45]
American College of Radiology breast cancer screening guidelines: New ACP Breast Cancer Screening Guidelines May Cost Lives | American College of Radiology and Society of Breast Imaging Statement (April 17, 2026) | [7:45]
Risk calculator, Tyrer-Cuzick: Breast Cancer Risk Calculator | Ikonopedia® | [17:00]
DCIS progression to invasive cancer: Progression from ductal carcinoma in situ to invasive breast cancer: molecular features and clinical significance | Signal Transduction and Targeted Therapy (J Wang et al. 2024) | [21:30]
Abbreviated MRI protocol for women with dense breasts: Multireader Diagnostic Accuracy of Abbreviated Breast MRI for Screening Women with Extremely Dense Breasts | Radiology (S van Grinsven et al. 2025) | [24:15]
DENSE trial recommended MRI screening for women with extremely dense breasts: Supplemental MRI Screening for Women with Extremely Dense Breast Tissue | NEJM (M Bakker et al. 2019) | [24:45]
Rate of cancer detection using a standard mammogram and handheld ultrasound: Combined screening with ultrasound and mammography vs mammography alone in women at elevated risk of breast cancer | JAMA (W Berg et al. 2008) | [26:30]
Rate of cancer detection using DBT (a more sensitive mammogram) and handheld ultrasound: Prospective Multicenter Diagnostic Performance of Technologist-Performed Screening Breast Ultrasound After Tomosynthesis in Women With Dense Breasts (the DBTUST) | Journal of Clinical Oncology (W Berg et al. 2023) | [26:45]
Secondary analysis of CISNET data shows annual screening is better for saving lives: Outcomes of Breast Cancer Screening Strategies Based on Cancer Intervention and Surveillance Modeling Network Estimates | Radiology (D Monticciolo, R Hendrick, M Helvie 2024) | [33:15]
Observational data comparing biennial and annual screening supports annual screening: Annual Screening Mammography Associated With Lower Stage Breast Cancer Compared With Biennial Screening | American Journal of Roentgenology (S Moorman et al. 2021) | [34:30]
Risk of breast cancer in women under age 40: Risk-Based Screening Mammography for Women Aged <40: Outcomes From the National Mammography Database | Journal of the American College of Radiology (C Lee et al. 2020) | [39:45]
Aggressive subtypes of cancer: Has tumor doubling time in breast cancer changed over the past 80 years? A systematic review | Cancer Medicine (M Dahan et al. 2021) | [42:00]
BRCA1 mutation increases risk of cancer earlier in life: Breast Cancer Screening: Common Questions and Answers | American Family Physician (M Khan, A Chollet 2021) | [43:00]



